

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
What is diabetes insipidus?
Diabetes insipidus (DI) is a disease characterised by the passage of large volumes (>3L/24hrs) of dilute urine (osmolality <300 mOsmol/Kg).¹
In some cases, the volume of urine produced can be as much as 20 litres in a 24 hour period and therefore rapid dehydration can easily occur, leading to death if not managed appropriately.
Normal physiology
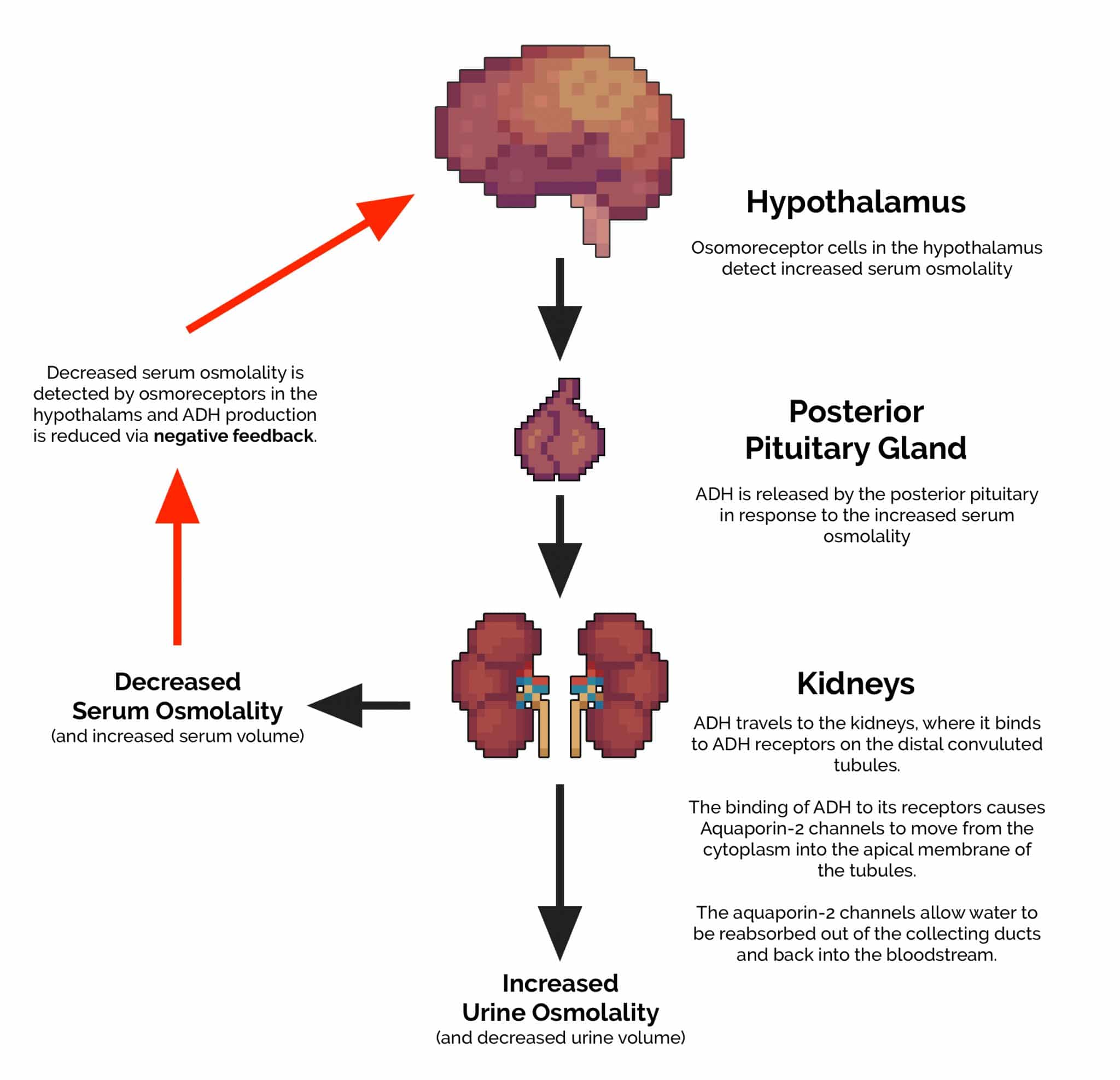
1. Vasopressin (antidiuretic hormone/ADH) is produced by the hypothalamus in response to increased serum osmolality.
2. Vasopressin is then transported to the posterior pituitary gland, where it is released into the blood.
3. Vasopressin then travels to the kidneys where it binds to vasopressin receptors on the distal convoluted tubules.
4. This binding causes aquaporin-2 channels to move from the cytoplasm into the apical membrane of the tubules:
- Aquaporin-2 channels allow water to be reabsorbed out of the collecting ducts and back into the bloodstream
- This results in both a decrease in volume and an increase in osmolality (concentration) of the urine being excreted
5. The extra water that has been reabsorbed re-enters the circulatory system, reducing serum osmolality.
6. This reduction in serum osmolality is detected by the hypothalamus as negative feedback, resulting in decreased production of vasopressin.
Causes of diabetes insipidus
Neurogenic diabetes insipidus¹
Neurogenic diabetes insipidus occurs as a result of decreased circulating levels of vasopressin (ADH). Vasopressin is responsible for promoting the kidneys to retain fluid, therefore, decreased circulating levels of ADH results in the production of increased volumes of urine. Vasopressin is produced by the hypothalamus and released by the posterior pituitary gland, meaning damage to either of these structures can cause diabetes insipidus.
Causes of neurogenic diabetes insipidus include:
- Mutations in the vasopressin gene (e.g. autosomal dominant AVP-NPII)
- Idiopathic (25% of cases)
- Tumours: pituitary adenomas or craniopharyngiomas/metastases
- Trauma
- Infections (e.g. meningitis)
- Vascular (e.g. Sheehan’s syndrome)
- Sarcoidosis: formation of granulomas in the pituitary gland.
- Haemochromatosis: deposition of iron in the pituitary gland and hypothalamic tissue.
Nephrogenic diabetes insipidus¹
The kidneys are responsible for reabsorbing fluid when ADH binds to their receptors. Anything which interferes with this binding or damages the kidneys has the potential to cause diabetes insipidus.
Causes of nephrogenic diabetes insipidus include:
- Mutations in the ADH receptor gene
- Mutations in the aquaporin-2 gene (aquaporin 2 is responsible for reabsorption of water from the urine)
- Metabolic – hypercalcaemia/hyperglycaemia/hypokalaemia
- Drugs – lithium/demeclocycline – both interfere with the binding of ADH
- Chronic renal disease
- Amyloidosis
- Post obstructive uropathy
Dipsogenic diabetes insipidus¹
Dipsogenic diabetes insipidus occurs as a result of hypothalamic disease or trauma. The hypothalamus is responsible for controlling the thirst mechanism which is a key component of maintaining normovolaemia. In dipsogenic diabetes, the thirst mechanism damaged, resulting in the affected patient being excessively thirsty regardless of their fluid status. The patient, therefore, consumes large volumes of fluid, which suppresses the secretion of ADH and increases urine output.
Gestational diabetes insipidus
During pregnancy, the placenta produces vasopressinase which breaks down vasopressin. Gestational diabetes insipidus is therefore thought to be caused by the overproduction of vasopressinase by the placenta causing a deficiency of functional vasopressin.
Primary polydipsia
Primary polydipsia is characterised by an individual consuming large volumes of fluid and as a result producing large volumes of dilute urine. The symptoms of primary polydipsia are therefore very similar to those of diabetes insipidus, however, a fluid deprivation test can help distinguish the diseases. Most often primary polydipsia is due to a behavioural disorder.
Symptoms and signs
Symptoms
Typical symptoms of diabetes insipidus include:
- Excessive urination (>3L/24hrs)
- Excessive thirst (especially for ice-cold water)
- Nocturia
- Dehydration – headache/dizziness/dry mouth
Signs
Typical clinical signs of diabetes insipidus include:
- Hypotension
- Dilute urine
- Signs of dehydration (dry mucous membranes, prolonged capillary refill time)
Investigations
24-hour urine collection
24-hour urine collection should be performed to measure the amount of urine produced.
Diabetes insipidus typically involves the production of more than 3 litres of urine in a 24-hour period.
Blood tests
Blood tests relevant to diabetes insipidus include:
- Plasma glucose (to help rule out diabetes mellitus)
- U&Es: to assess renal function and rule out electrolyte abnormalities
- Urine specific gravity
- Simultaneous plasma and urine osmolality
Fluid deprivation test 2
The patient is deprived of fluids for up to eight hours or 5% loss of body weight, following which desmopressin is given (see the table below for the interpretation of results).
MRI brain
MRI imaging of the pituitary, hypothalamus and pineal gland is used to assess for cranial causes of diabetes insipidus (e.g. pituitary tumour).
Renal tract ultrasound
Renal tract ultrasound or intravenous pyelogram is used to assess for evidence of post-obstructive uropathy.
Diagnosis
The fluid deprivation test can provide an initial indication as to the likely cause of diabetes insipidus (e.g. neurogenic, nephrogenic).
The table below shows the likely underlying cause based on the results of the fluid deprivation test.1,2
|
Urine osmolality after fluid deprivation (mOsm/kg)
|
Urine osmolality after desmopressin (mOsm/kg)
|
Likely diagnosis
|
|
<300
|
>800
|
Neurogenic DI
|
|
<300
|
<300
|
Nephrogenic DI
|
|
>800
|
>800
|
Primary polydipsia
|
Neurogenic diabetes insipidus
If the diagnosis is neurogenic DI the urine osmolality will be low after fluid deprivation but normalise after desmopressin is given.
This is because neurogenic DI is caused by the lack of ADH production, therefore, giving a synthetic form of ADH such as desmopressin normalises levels of the hormone resulting in the normalisation of serum and urine osmolality.
Nephrogenic diabetes insipidus
If the diagnosis is nephrogenic DI then the urine osmolality will remain low throughout regardless of desmopressin. This is because the kidneys are unable to respond to either synthetic or endogenous ADH.
Primary polydipsia
If the diagnosis is primary polydipsia the urine osmolality will remain high after fluid deprivation as well as after desmopressin is given. This is because the patient’s vasopressin axis is intact and otherwise completely normal.
Partial diabetes insipidus or polydipsia
If the diagnosis is that of partial DI or polydipsia the picture may be mixed and further investigations are required.
Management
Neurogenic diabetes insipidus
The primary issue in neurogenic DI is an endogenous deficiency of ADH. As a result, replacement with a synthetic form of ADH such as desmopressin is usually effective. Desmopressin can be given orally, intranasally or parenterally. Patients require ongoing monitoring due to the risks associated with desmopressin treatment (e.g. overdose results in hyponatraemia). Typically, patients require serum sodium osmolality measuring every 1 to 3 months.2
Nephrogenic diabetes insipidus
If daily urine volume is less than 4 litres/24hrs and the patient is not severely dehydrated, definitive therapy is not always necessary. Patients need access to drinking water and should be advised to drink enough to satisfy their thirst. Metabolic abnormalities should be corrected if present and any medications that could be causing the problem should also be stopped (e.g. lithium, demeclocycline). High dose desmopressin is sometimes used for mild-to-moderate cases of nephrogenic DI.2
Primary polydipsia
The underlying psychiatric disorder needs to be treated.
References
- Dr Colin Tidy. Diabetes Insipidus. Patient.info. Published December 2015. Available from: [LINK].
- Saifan C, Nasr R, Mehta S, et al; Diabetes insipidus: a challenging diagnosis with new drug therapies. ISRN Nephrol. 2013 Mar 242013:797620. doi: 10.5402/2013/797620. eCollection 2013. Available from: [LINK].
