

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
This article outlines the anatomy of the eye and bony orbit. It also discusses the various visual pathways and visual field defects.
The bony orbit
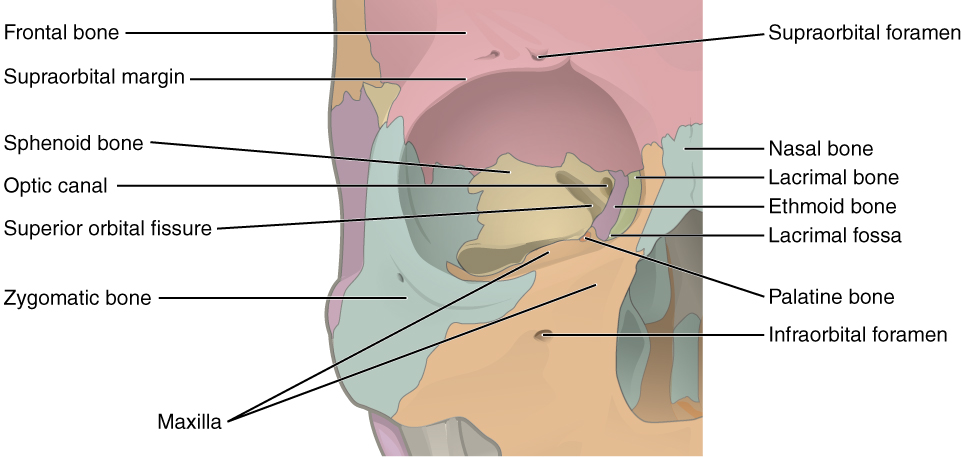
The bony orbit is composed of seven bones. They form a pyramidal structure with the apex facing posteriorly (Figure 1).
The walls of the orbit are as follows:
- Roof: the orbital part of the frontal bone, with a small contribution from the sphenoid bone
- Medial wall: lacrimal, maxilla, ethmoid and sphenoid bones
- Floor: the majority is formed by the orbital part of the maxilla, with a minor contribution from the zygomatic and palatine bones
- Lateral wall: the anterior section is formed from the zygomatic bone, with the posterior section consisting of the greater wing of the sphenoid bone
Contents of the orbit
The contents of the orbit include:
- The eye
- Extraocular muscles
- Cranial nerves II-VI
- Arterial supply and venous drainage
Any space within the orbit which is not otherwise occupied is filled with orbital fat.
The eye
The eye can be divided into fibrous, vascular and inner layers.
Fibrous layer
The fibrous layer is the outermost layer and consists of the cornea and sclera, which are continuous with one another.
- The cornea is located in the centre of the anterior aspect of the eye and is transparent
- The sclera, which covers the rest of the eye, is white
Vascular layer
The vascular layer is composed of the ciliary body, choroid and iris.
- The ciliary body is attached to the lens via the suspensory ligaments; it controls the shape of the lens and forms the aqueous humour
- The choroid is a layer of connective tissue which contains the blood vessels that supply the retina
- The iris is a structure containing a central aperture (the pupil) which contains smooth muscle that controls its diameter
Inner layer
The inner layer contains the retina, which is made of neural and pigmented layers.
- The neural layer is composed of photoreceptors and is deficient in the anterior portion of the eye. The centre of the posterior aspect of the retina is called the macula, within which lies the fovea. The fovea contains the highest concentration of photoreceptors in the retina and is responsible for high acuity vision. The area where the optic nerve enters the retina is called the optic disc; this area contains no photoreceptors
- The pigmented layer lies between the neural layer and the choroid. It supports the neural layer and is continuous throughout the entire eye
Sections of the eye
There are three fluid-filled areas within the eye: the anterior chamber, posterior chamber and vitreous body.
- The anterior and posterior chambers contain aqueous humour, which is constantly produced and drained from the eye. Impaired drainage of aqueous humour can result in glaucoma
- The vitreous body contains vitreous humour

The extraocular muscles
In total, there are seven extraocular muscles.
Six of these are responsible for the movement of the eye, with the seventh being responsible for the movement of the superior eyelid.
The muscles responsible for the movement of the eye may be divided into the four recti muscles and the two oblique muscles.
Table 1. An overview of the extraocular muscles responsible for eye movements.
|
Muscle |
Origin |
Insertion |
Action |
Innervation |
|
Superior rectus |
Common tendinous ring |
Superior aspect of sclera |
Elevates eye |
|
|
Inferior rectus |
Common tendinous ring |
Inferior aspect of sclera |
Depresses eye |
|
|
Medial rectus |
Common tendinous ring |
Medial aspect of sclera |
Adducts eye |
|
|
Lateral rectus |
Common tendinous ring |
Lateral aspect of sclera |
Abducts eye |
|
|
Superior oblique |
Body of sphenoid |
Sclera, posterior to superior rectus |
Depresses and abducts eye |
|
|
Inferior oblique |
Orbital floor |
Sclera, posterior to lateral rectus |
Elevates and abducts eye |
The final extraocular muscle is levator palpebrae superioris, which originates from the lesser wing of the sphenoid bone and inserts onto the superior tarsal plate of the superior eyelid. It elevates the superior eyelid and is innervated by the oculomotor nerve (CN III).

A useful way to remember the actions of the extraocular muscles is the acronym SO4 LR6 EE3:
- SO4: superior oblique is supplied by CN IV (trochlear nerve)
- LR6: lateral rectus is supplied by CN VI (abducens nerve)
- EE3: everything else (inferior oblique; levator palpebrae superioris; superior, inferior and medial recti) is supplied by CN III (oculomotor nerve)
Nerve palsies
Understanding the anatomy of the extraocular muscles is useful for understanding cranial nerve palsies.
In the event of a palsy, the muscles supplied by the affected nerve will not work.
With an oculomotor nerve (CN III) palsy, the two unaffected muscles are the superior oblique and lateral rectus. This results in a depressed and abducted eyeball, with partial ptosis (drooping of the superior eyelid) on the affected side.
In the event of a trochlear nerve (CN IV) palsy, the action of the superior oblique muscle is lost. Since the lateral and inferior recti muscles collectively perform the same action as the superior oblique muscle, there is often no obvious eye displacement. Patients may, however, complain of diplopia (double vision) and develop a head tilt away from the affected side.
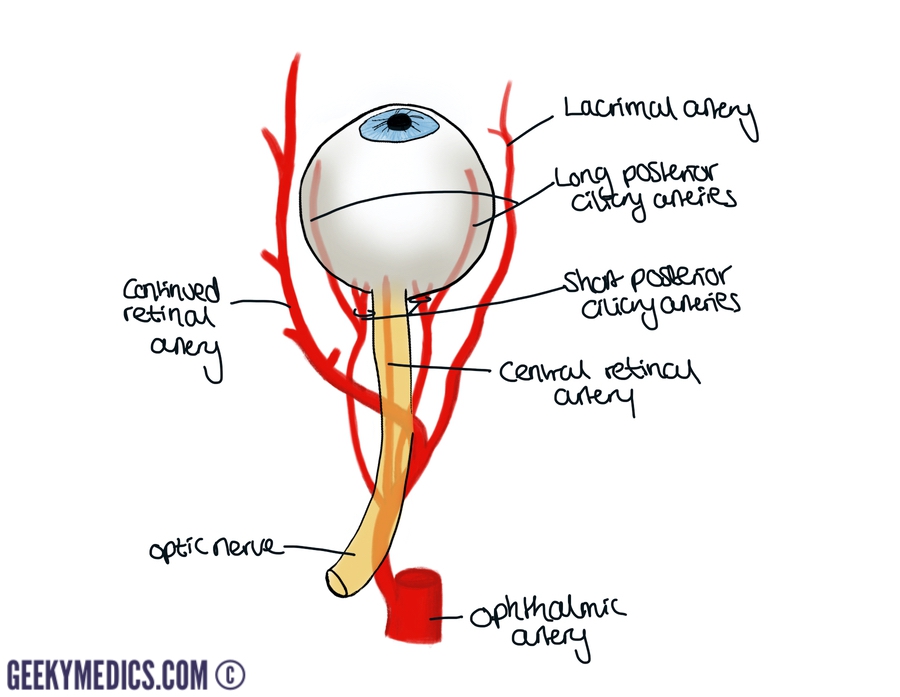
Arterial supply
The ophthalmic artery arises from the internal carotid artery. Initially, it gives rise to the central retinal artery, which pierces the optic nerve and runs within it to reach the retina at the optic disc. The branches of the central retinal artery are visible with an ophthalmoscope.
The ophthalmic artery then branches into the short posterior ciliary arteries, which pierce the sclera and supply the choroid up to the equator of the eye. Long posterior ciliary arteries run a similar course but move further into the eye to supply the anterior aspect of the choroid in addition to the iris and ciliary bodies.
The ophthalmic artery also branches into the lacrimal artery, which supplies the lacrimal gland and the lateral portion of the eyelid.
The final part of the ophthalmic artery supplies the ethmoid bone and medial part of the eyelid.
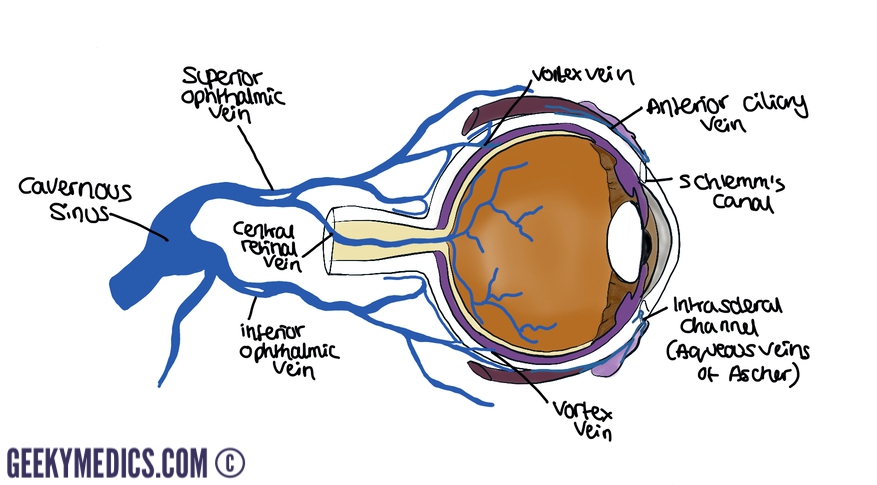
Venous drainage
The eyeball receives its venous drainage from the central retinal and vortex veins.
Individuals commonly have between 4 and 8 vortex veins. The superior vortex veins join to form the superior ophthalmic vein, which then receives the central retinal vein. The inferior vortex veins form the inferior ophthalmic vein.
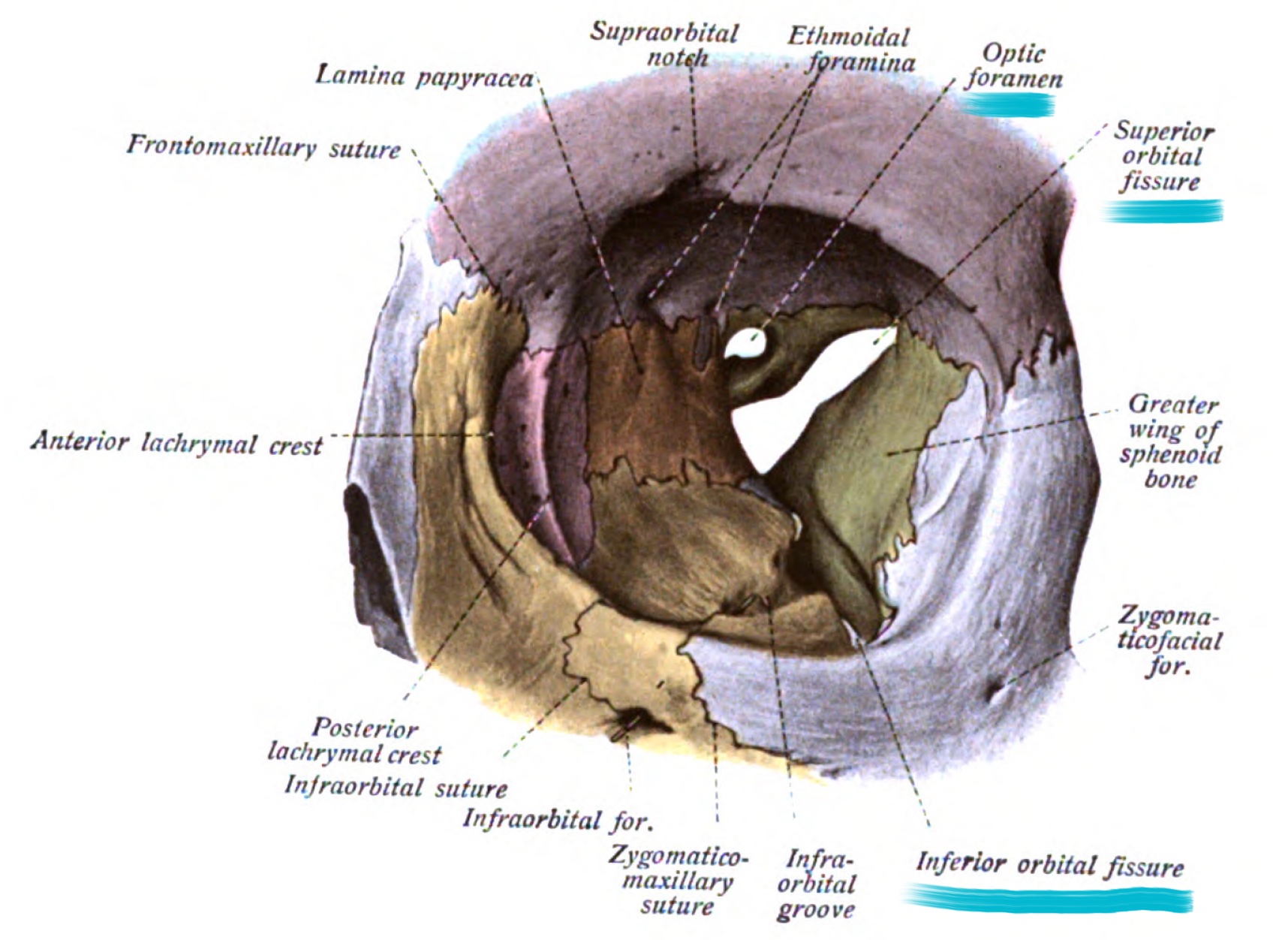
Pathways into the orbit
The three main pathways into the orbit are the optic canal, superior orbital fissure and inferior orbital fissure.
Optic canal
The optic canal transmits the ophthalmic artery and the optic nerve (CN II).
Superior orbital fissure
The common tendinous ring crosses the superior orbital fissure. Structures passing through the superior orbital fissure within this ring include the oculomotor nerve (CN III), abducens nerve (CN VI) and the nasociliary nerve, which is a branch of the ophthalmic nerve.
Structures passing through the superior orbital fissure that are not contained within the tendinous ring include the superior ophthalmic vein, trochlear nerve (CN IV), two branches of the ophthalmic nerve (CN V1), lacrimal nerve and frontal nerves.
Inferior orbital fissure
The inferior orbital fissure transmits the inferior ophthalmic vein and the zygomatic nerve, which is a branch of the maxillary nerve (CN V2).
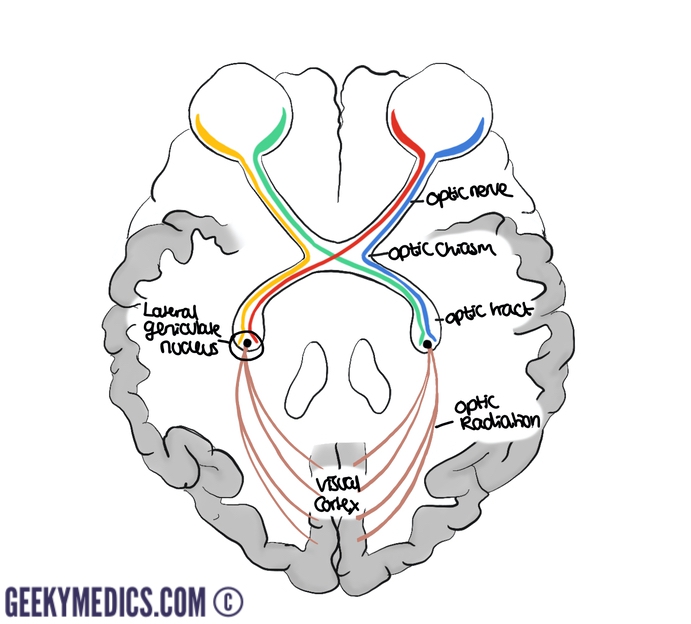
Optic nerve
Once leaving the orbit via the optic canal, the optic nerves enter the middle cranial fossa. Here, the two optic nerves unite to form the optic chiasm.
Within the chiasm, fibres from the medial side of each retina cross over to form right and left optic tracts.
The optic tracts then pass to the lateral geniculate nuclei where they synapse. Secondary neurones subsequently pass from the lateral geniculate nucleus to the visual cortex via optic radiations.
This complicated arrangement enables responses to threatening stimuli to be executed as quickly as possible.
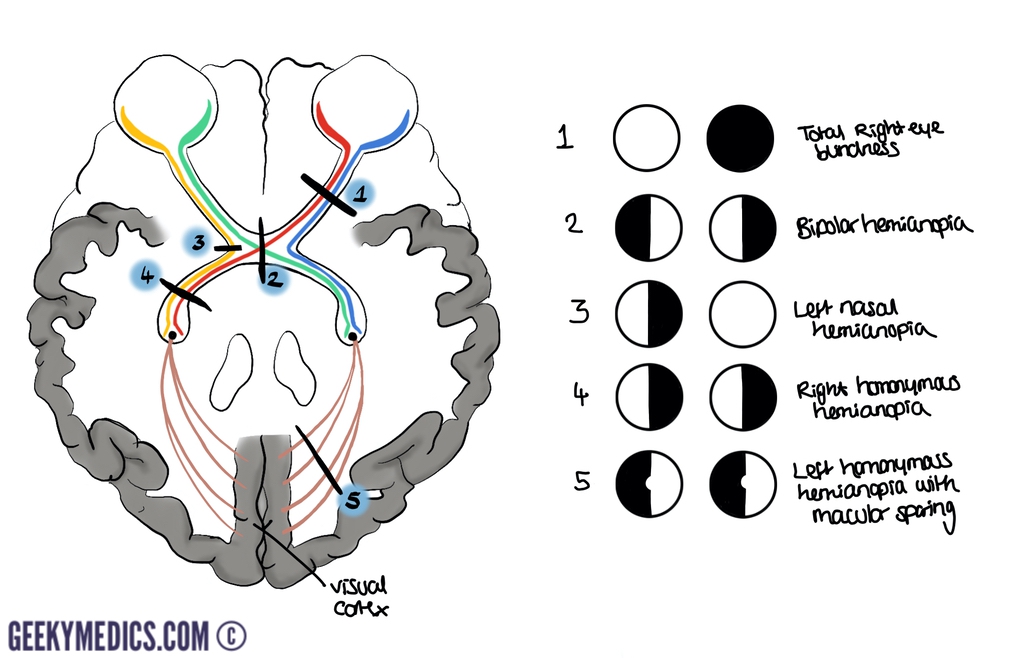
Visual field defects
Understanding the anatomy of the optic nerve is important for understanding how lesions in different locations will affect vision, as illustrated below. When a lesion lies within the optic radiations, the maculae remain unaffected.
Illustrator
Aisha Ali
Medical student and illustrator
References
- OpenStax College. Bony Orbit. License: [CC BY 3.0]
- By Rhcastilhos. And Jmarchn. License: [CC BY-SA 3.0]
