
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
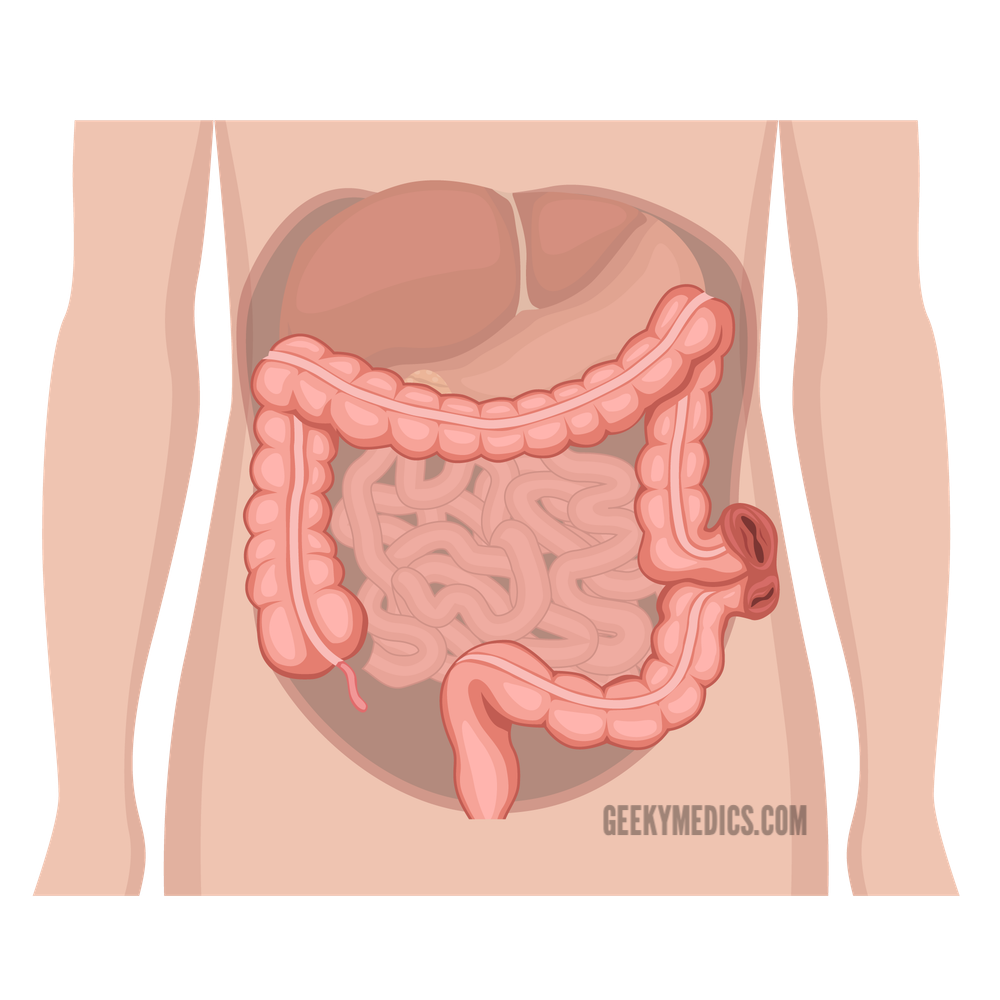
Introduction
A stoma is a surgically created opening in the body between the skin and a hollow viscus (stoma has the Greek meaning ‘mouth’). Abdominal stomas are mainly used to divert faeces or urine outside the body, which can then be collected in a bag on the skin.
There are three common stoma types:
- Colostomy
- Ileostomy
- Urostomy
Each stoma can be either permanent or temporary.
A stoma’s position, appearance and contents can indicate which type of stoma it is and provide clues as to the patient’s previous surgical history. For more information, see our OSCE guide to performing a stoma examination.
Colostomy
As the name suggests, colostomies are made using the large bowel (or colon).
One of the hallmarks of colostomies is that they are found in the left iliac fossa (LIF).
The contents of a colostomy bag should be solid or semisolid as the faeces have had time to travel through the colon, undergoing water absorption.
Colostomies are positioned flush to the skin (i.e. no spout) because the enzymes present in large bowel contents are less alkali and, therefore, less irritating to the skin.
End colostomy
In an end colostomy, the end of the colon is brought to the abdominal wall and used to create a stoma.

Permanent vs temporary
Permanent end-colostomies are often performed after abdominoperineal resection of low rectal or anal cancers leading to the removal of the entire rectum.
Temporary end-colostomies are sometimes performed to allow the distal bowel to rest in acute diverticulitis, obstruction or bowel leak. In a two-stage Hartmann’s procedure, the rectum and bowel are re-anastomosed later once acute inflammation has settled.
Loop colostomy
Loop colostomies are performed to protect distal anastomoses after recent surgery. They can also be performed to decompress distal bowel obstruction.
A loop of bowel will be brought to the skin’s surface and half-opened. This allows the faecal matter to drain into the stoma bag without reaching the distal anastomoses.
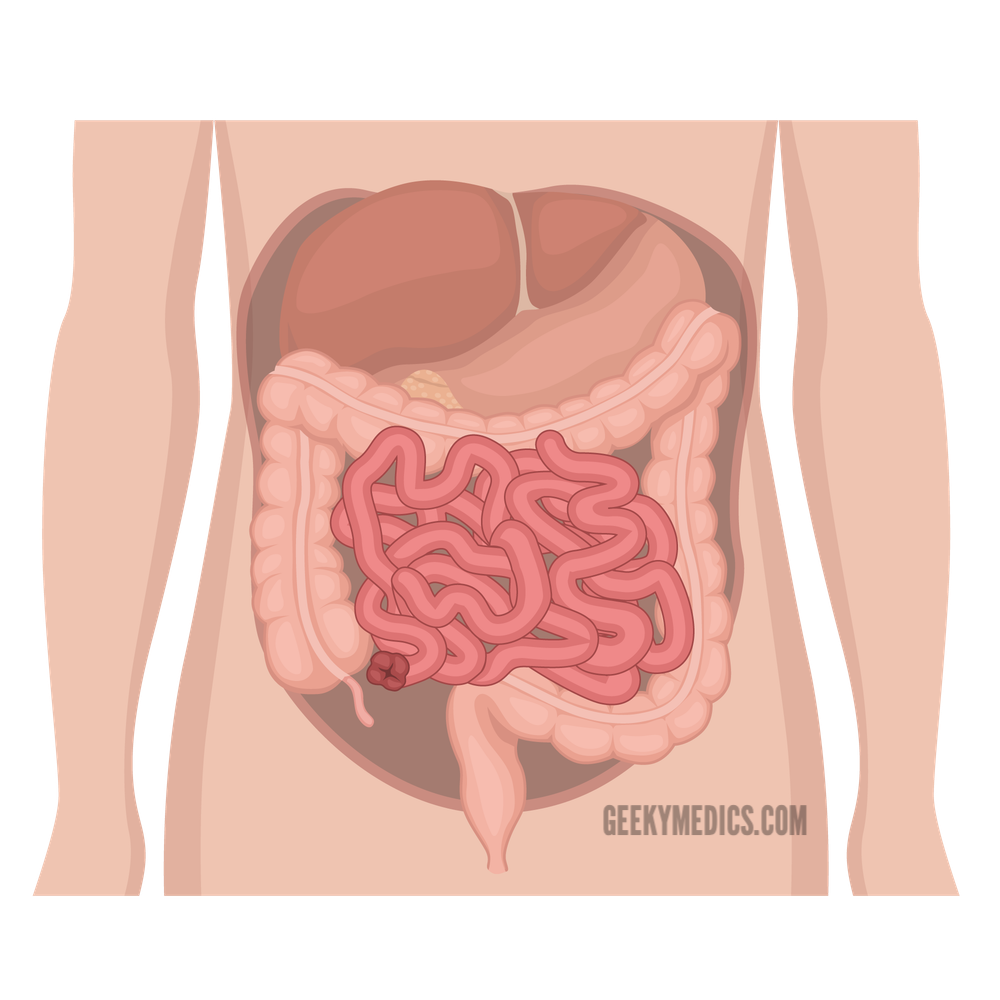
Ileostomy
Ileostomies are created using small bowel and are typically located in the right iliac fossa (RIF).
Less water is absorbed in the small bowel, so the contents of the stoma bag tend to have a liquid or mushy consistency.
Because the enzymes in small bowel contents can irritate the skin, the bowel has a spout sticking out from the abdominal wall. This allows faeces to drain without touching the skin.
End ileostomy
In an end ileostomy, the end of the small bowel is brought to the abdominal wall and used to create a stoma.
Temporary vs permanent
Permanent ileostomies are typically created after a panproctocolectomy for conditions such as ulcerative colitis or familial adenomatous polyposis.
A temporary end-ileostomy is typically created during emergency bowel resection where it is considered unsafe to form an anastomosis with the remaining bowel at that time (e.g. diseased bowel, intra-abdominal sepsis or bleeding).
Loop ileostomy
Temporary loop ileostomies are created the same way as temporary loop colostomies, with two openings visible.
They are used to protect distal anastomoses or decompress distal bowel obstruction.
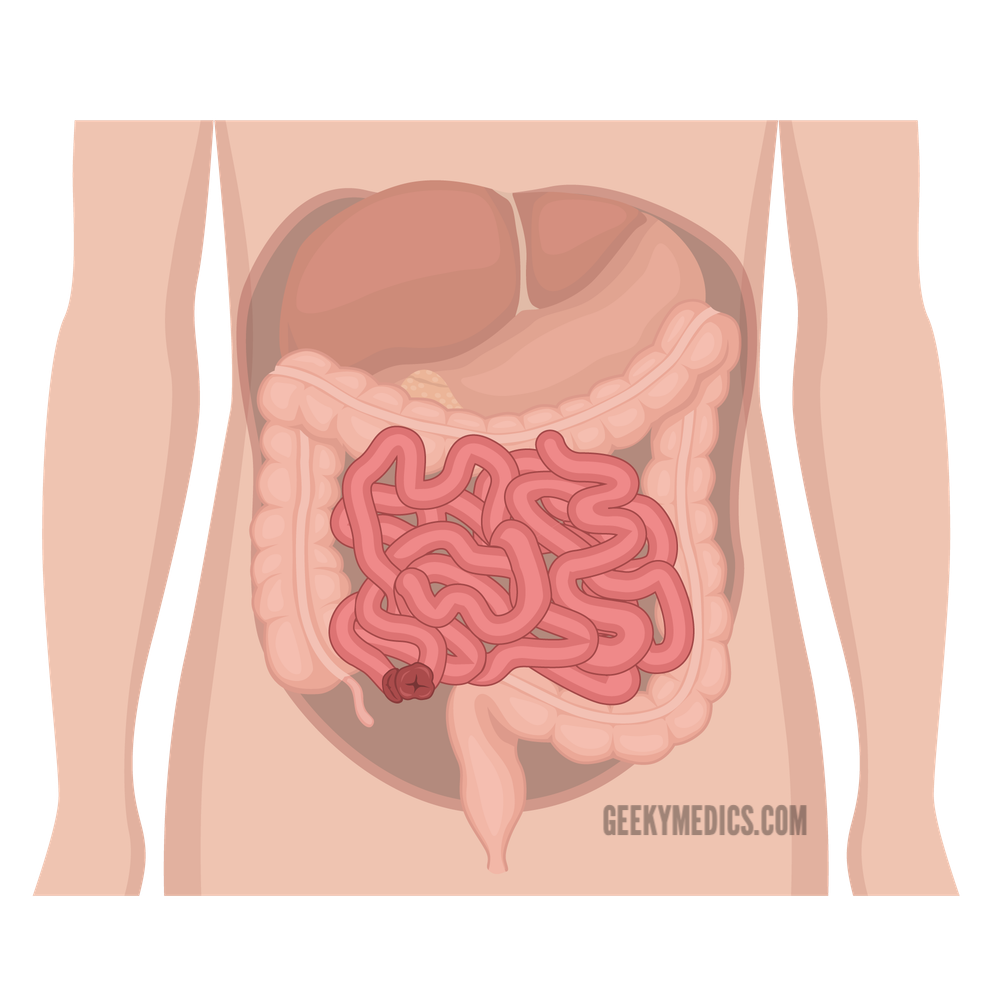
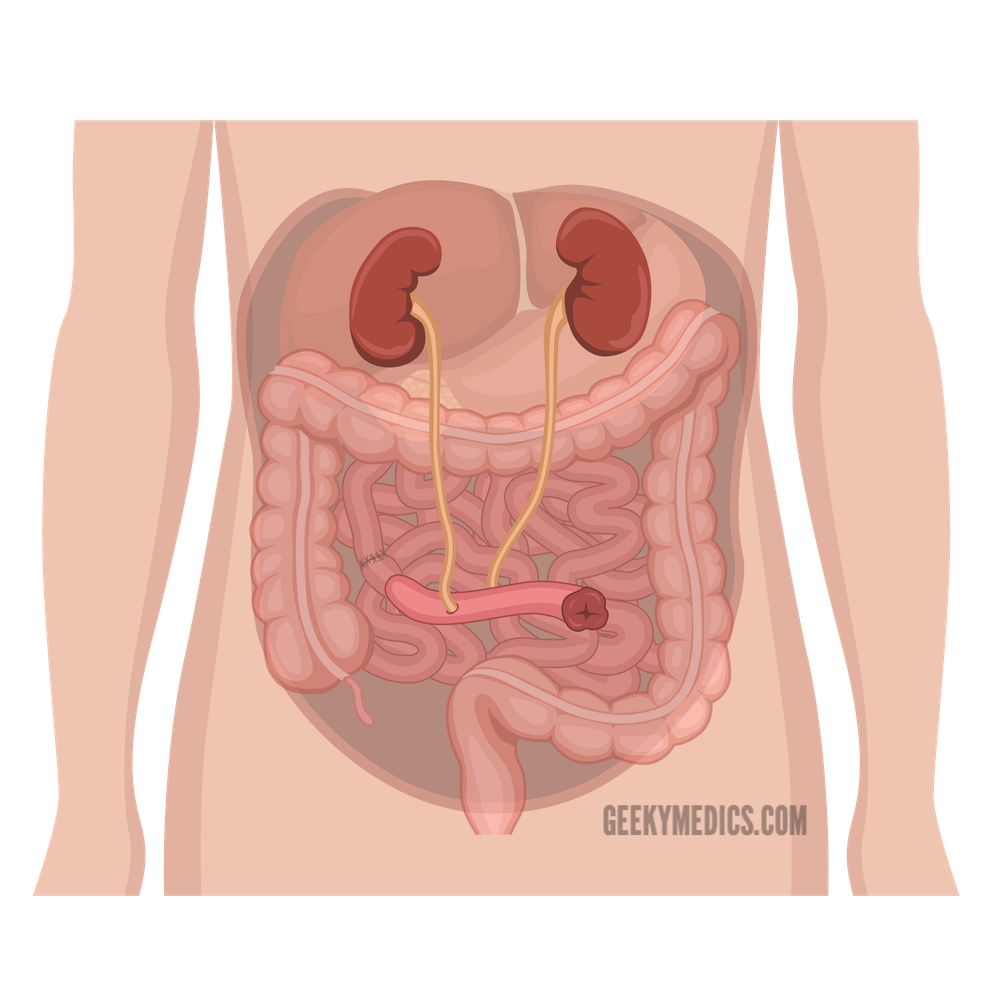
Urostomies
Urostomies after created after a cystectomy (bladder removal) and are typically located in the right iliac fossa (RIF).
An ileal conduit is used to route the urine out of the abdomen into the bag. This involves a piece of ileum being resected then attached to the skin with a spout protruding.
The ureters are then attached to the other end of the bowel.
The urine then drains via the piece of ileum into the stoma bag.
Summary
Table 1. A summary of the different types of stoma.
| Site | Lumens | Spout | Effluent | Anatomy | Indications | |
| End colostomy | Left iliac fossa | 1 lumen | Absent (flush with skin) | Solid or semisolid faeces | Sigmoid/descending colon |
|
| Loop colostomy | Left iliac fossa | 2 lumens close together | Absent (flush with skin) | Solid or semisolid faeces | Sigmoid/descending colon |
|
| End ileostomy | Right iliac fossa | 1 lumen | Present | Mushy or liquid small bowel content | Usually distal/terminal ileum |
|
| Loop ileostomy | Right iliac fossa | 2 lumens close together | Present | Mushy or liquid small bowel content | Usually terminal ileum |
|
| Urostomy | Right iliac fossa | 1 lumen | Present | Urine | Ureters draining via ileal conduit |
|
