
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Acoustic neuromas are rare tumours of the vestibulocochlear nerve, arising from the Schwann cells of the nerve sheath (also known as vestibular schwannomas).
Acoustic neuromas can develop at various locations along the vestibulocochlear nerve including within the internal auditory meatus and at the cerebellopontine angle. Tumours that develop within the internal auditory meatus cause symptoms (hearing loss and vestibular disturbance) earlier than those at the cerebellopontine angle.
Most acoustic neuromas are benign and slow-growing, however, because acoustic neuromas often occur at the cerebellopontine angle, compression of local structures can lead to life-threatening complications.1,2
Acoustic neuromas are usually unilateral and occur sporadically. The development of bilateral acoustic neuromas is a typical feature of the genetic condition neurofibromatosis type 2 (NF2).2
Aetiology
Pathophysiology
The cause of acoustic neuromas is unknown. However, there is growing evidence to suggest sporadic defects in tumour suppressor genes are involved in their development.
The typical clinical features of hearing loss and vestibular disturbance occur because of the compression of local neural structures or their nutrient blood supply. These local structures include the vestibular, trigeminal and facial nerves, as well as the cerebellum and brainstem.9
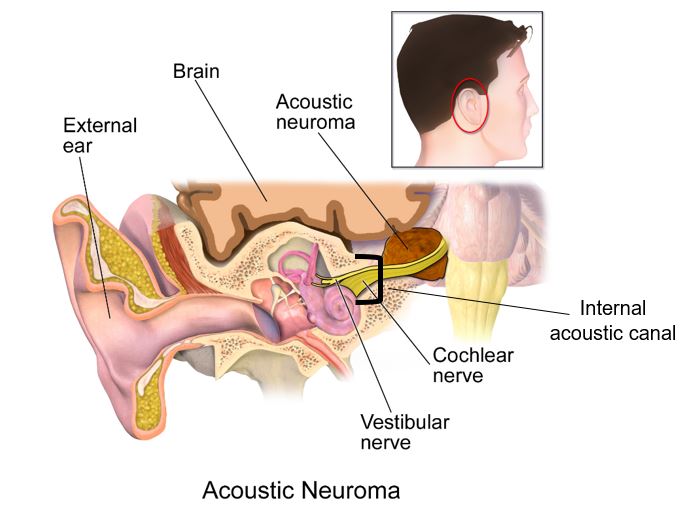
Figure 1. Illustration depicting the location of an acoustic neuroma.8
Risk factors
Risk factors for acoustic neuroma include:5
- High-dose ionising radiation to the head and neck
- Neurofibromatosis type 2 (NF2)
Clinical features
History
Typical symptoms of acoustic neuroma include:
- Unilateral sensorineural hearing loss (SNHL) and/or tinnitus: 90% of patients present with progressive SNHL, whereas only 5% present with sudden SNHL
- Dizziness and disequilibrium (vestibular dysfunction)
Other symptoms can include:2,9
- Facial pain and numbness: trigeminal (CN V) nerve compression
- Facial weakness: facial (CN VII) nerve compression
- Headaches, nausea and vomiting: raised intracranial pressure
Other important areas to cover in the history include:
- Past medical history or family history of similar tumours (if considering NF2)
Clinical examination
A thorough hearing and cranial nerve assessment should be performed if acoustic neuroma is suspected.
Typical findings of Rinne’s and Weber’s test are:
- Rinne’s test: air conduction > bone conduction bilaterally
- Weber’s test: sound lateralises to the unaffected ear indicating SNHL3
Differential diagnoses
Differential diagnoses to consider include:
- Meningioma (accounts for 5-10% of cerebellopontine angle tumours)
- Ectodermal inclusion tumours (includes epidermoid and dermoid tumours)
- Neuromas originating from other cranial nerves
- Extension of nearby lesions (e.g. brainstem or cerebellar glioma, pituitary adenoma, craniopharyngioma)
Investigations
All patients presenting with unexplained unilateral sensorineural hearing loss should be investigated for acoustic neuroma with an MRI head.1
Hearing assessment
Pure-tone audiometry should be performed to confirm the presence of SNHL.
Imaging
Magnetic resonance imaging (MRI) is the gold standard investigation for identifying acoustic neuroma.
Management
There is a range of management options for acoustic neuroma including active observation, microsurgery and radiosurgery.
The choice of management strategy depends on several factors including:
- Size of the tumour
- Patient factors (age and future quality of life)
- Involvement of local structures
Conservative treatment
Conservative treatment involves active surveillance with annual neuroimaging (MRI head) to monitor the growth of the tumour.
Patients who present with small tumours with no impairment to facial nerve function or hearing are sometimes managed with a ‘watch and wait’ approach due to the risks associated with interventional treatment.
Elderly patients with multiple medical co-morbidities are also often managed using this approach due to the increased risks associated with interventional treatment.2
Microsurgery
Microsurgery is the treatment of choice for most patients who receive active management.
In a systematic review, microsurgery was found to provide the best outcomes in terms of tumour control compared to other management strategies.16
There are several ways of surgically excising the tumour, including retrosigmoid, translabyrinthine and middle fossa approaches. The choice of surgical approach depends on the location and size of the tumour.11
Risks of microsurgery include:12,13
- Cerebrospinal fluid leak
- Cerebellar injury
- Meningitis
- Hearing loss and/or facial paralysis
- Death (mortality risk approximately 1%)
Stereotactic radiosurgery
Stereotactic radiosurgery is typically used for small tumours that are less than 3 centimetres in diameter.
The treatment involves using high energy gamma rays to deliver a single dose of radiation to the tumour (known as a ‘gamma knife’ surgery).
This approach is sometimes also used for moderate-sized tumours and partially resected tumours, with the aim of stopping or slowing the growth of the tumour.
As well as being a much less invasive approach, stereotactic radiosurgery has a comparatively better hearing preservation rate compared to microsurgery.1
Risks associated with stereotactic radiosurgery include:14,15
- Radiation necrosis of the brain
- Malignant change of the neuroma to glioblastoma multiforme
Complications
Complications of acoustic neuroma include:
- Hearing loss
- Facial paralysis
- Hydrocephalus (rare)
- Compression of the cerebellar peduncles, cerebellum, brainstem and cranial nerves IX-XI.
Key points
- An acoustic neuroma is a rare, benign, slow-growing tumour originating from the Schwann cells of the vestibulocochlear nerve.
- Acoustic neuromas are usually unilateral, however, in rare cases, bilateral acoustic neuromas can develop, typically in individuals with NF2.
- Unexplained unilateral sensorineural hearing loss (SNHL) requires urgent investigation with MRI head to rule out acoustic neuroma.
- Common clinical features associated with an acoustic neuroma include unilateral SNHL, tinnitus and vestibular disturbance.
- Conservative treatment involves regular active surveillance using neuroimaging.
- Microsurgery is the most common active treatment, whereas stereotactic radiosurgery is typically used for smaller and/or partially resected tumours.
- Complications of an acoustic neuroma can include hearing loss, facial paralysis, hydrocephalus and compression of the cerebellum and brainstem.
Reviewer
Ms Shadaba Ahmed
ENT Consultant
References
- Patient. Acoustic Neuromas. Published in 2014. Available from: [LINK]
- GP Notebook. Acoustic neuroma. Available from: [LINK]
- Andrew Baldwin, Nina Hjelde, Charlotte Goumalatsou and Gil Myers. Oxford Handbook of Clinical Specialties 10th Ear, Nose and Throat. Published in 2016. Available from: [LINK]
- Joshua Greene, Mohammed A. Al-Dhahir. Acoustic neuroma (Vestibular Schwannoma). Published in 2020. Available from: [LINK]
- Schneider AB, Ron E, Lubin J, Stovall M, Shore-Freedman E, Tolentino J, Colling BJ. Acoustic neuromas following childhood radiation treatment for benign conditions of the head and neck. Published in 2008. Available from: [LINK]
- Faramarz Memari, Fatemah Hassannia, Seyed Hamid Reza Abtahi. Surgical Outcomes of Cerebellopontine angle Tumours in 50 cases. Published in 2015. Available from: [LINK]
- American Journal of Neuroradiology. Dumbbell Schwannomas of the Internal Auditory Canal. Published in 2001. Available from: [LINK]
- Wikimedia commons. Acoustic neuroma (modified by Arunachalam Soma). License: [CC BY-SA] Available from: [LINK]
- British Association of Otorhinolaryngologists – Head and Neck Surgeons. Acoustic Neuroma (Vestibular Schwannoma). Published in 2002. Available from: [LINK]
- Myrseth E, Pedersen PH, Moller P, Lund-Johansen M. Treatment of vestibular schwannoma. Why, when and how? Published in 2007. Available from: [LINK]
- Ramnarine Devindra, Whitfield Peter. Management of patients with vestibular schwannoma. Published in 2005.
- Douglas SA, Yeung P, Daudia A, Gatehouse S, O’Donoghue GM. Spatial hearing disability after acoustic neuroma removal. Published in 2007. Available from: [LINK]
- Action on Hearing Loss. Acoustic neuroma (vestibular schwannoma). Published in 2017. Available from: [LINK]
- American Journal of Otolaryngology. Radiation necrosis of the brain after radiosurgery for vestibular schwannoma. Published in 2007. Available from: [LINK]
- Neuro-oncology. Glioblastoma multiforme after stereotactic radiotherapy for acoustic neuroma: Case report and review of the literature. Published in 2007. Available from: [LINK]
- Neurological Research. Conservative management, gamma-knife radiosurgery, and microsurgery for acoustic neurinomas: A systematic review of outcome and risk of three therapeutic options. Published in 2003. Available from: [LINK]
