
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
This guide provides an overview of the recognition and immediate management of upper gastrointestinal bleeding (UGIB) using an ABCDE approach.
The ABCDE approach is used to systematically assess an acutely unwell patient. It involves working through the following steps:
- Airway
- Breathing
- Circulation
- Disability
- Exposure
Each stage of the ABCDE approach involves clinical assessment, investigations and interventions. Problems are addressed as they are identified, and the patient is re-assessed regularly to monitor their response to treatment.
This guide has been created to assist healthcare students in preparing for emergency simulation sessions as part of their training. It is not intended to be relied upon for patient care.
Clinical features of upper gastrointestinal bleeding
Typical clinical features of upper gastrointestinal bleeding include:
- Haematemesis: typically ‘coffee-ground’ in appearance due to the presence of partially digested blood
- Malaena: black, tarry stools caused by the presence of digested blood
- Abdominal pain: typically epigastric in location but can be diffuse
- Haematochezia: the passage of fresh red blood per rectum, although more common in lower gastrointestinal bleeding it can occur in the context of profuse upper gastrointestinal haemorrhage due to the rapid transit of blood through the gastrointestinal tract
- Haemodynamic instability: tachycardia, hypotension, syncope
Causes
Causes of upper gastrointestinal bleeding include:
- Peptic/duodenal ulcers: can be secondary to Heliobacter pylori or NSAIDs
- Oesophageal erosions
- Mallory-Weiss tear (usually a history of forceful retching preceding any bleeding)
- Oesophageal varices due to portal hypertension (e.g. advanced liver cirrhosis)
- Malignancy: bleeding tumour or erosion of gastrointestinal vessels
Patients may have clinical signs of the underlying condition causing gastrointestinal bleeding (e.g. ascites and jaundice in advanced liver cirrhosis).
Tips before you begin
General tips for applying an ABCDE approach in an emergency setting include:
- Treat problems as you discover them
- Re-assess regularly and after every intervention to monitor a patient’s response to treatment
- If the patient loses consciousness and there are no signs of life, put out a crash call and commence CPR
- Make use of the team around you by delegating tasks where appropriate
- All critically unwell patients should have continuous monitoring equipment attached
- Clearly communicate how often you would like the patient’s observations relayed to you by other staff members
- If you require senior input, call for help early using an appropriate SBAR handover
- Review results as they become available (e.g. laboratory investigations)
- Use local guidelines and algorithms to manage specific scenarios (e.g. acute asthma)
- Any medications or fluids must be prescribed at the time (you may be able to delegate this to another staff member)
- Your assessment and management should be documented clearly in the notes. However, this should not delay management. The A-E approach can also form the structure for documenting your assessment.
Initial steps
Acute scenarios typically begin with a brief handover, including the patient’s name, age, background and the reason the revie has been requested.
You may be asked to review a patient with UGIB due to tachycardia, hypotension, malaena and/or haematemesis.
Introduction
Introduce yourself to whoever has requested a review of the patient and listen carefully to their handover.
Interaction
Introduce yourself to the patient, including your name and role.
Ask how the patient is feeling, as this may provide useful information about their condition.
If the patient is unconscious or unresponsive, and there are no signs of life, start the basic life support (BLS) algorithm as per resuscitation guidelines.
Preparation
Ensure the patient’s notes, observation chart, and prescription chart are easily accessible.
Ask for another clinical member of staff to assist you if possible.
Airway
Clinical assessment
Can the patient talk?
Yes: if the patient can talk, their airway is patent, and you can move on to the assessment of breathing.
No:
- Look for signs of airway compromise: angioedema, cyanosis, see-saw breathing, use of accessory muscles
- Listen for abnormal airway noises: stridor, snoring, gurgling
- Open the mouth and inspect: look for anything obstructing the airway, such as blood, secretions or a foreign object
Interventions
Regardless of the underlying cause of airway obstruction, seek immediate expert support from an anaesthetist and the emergency medical team (often called the ‘crash team’). You can perform basic airway manoeuvres to help maintain the airway whilst awaiting senior input.
Head-tilt chin-lift manoeuvre
Open the patient’s airway using a head-tilt chin-lift manoeuvre:
- Place one hand on the patient’s forehead and the other under the chin
- Tilt the forehead back whilst lifting the chin forwards to extend the neck
- Inspect the airway for obvious obstruction. If an obstruction is visible within the airway, use a finger sweep or suction to try and remove it. Be careful not to push it further into the airway.
Jaw thrust
If the patient is suspected of having suffered significant trauma with potential spinal involvement, perform a jaw-thrust rather than a head-tilt chin-lift manoeuvre:
- Identify the angle of the mandible
- Place two fingers under the angle of the mandible (on both sides) and anchor your thumbs on the patient’s cheeks
- Lift the mandible forwards
Other interventions
Airway adjuncts are helpful and, in some cases, essential to maintain a patient’s airway. They should be used in conjunction with the manoeuvres mentioned above.
An oropharyngeal airway is a curved plastic tube with a flange on one end that sits between the tongue and hard palate to relieve soft palate obstruction. It should only be inserted in unconscious patients as it may induce gagging and aspiration in semi-conscious patients.
A nasopharyngeal airway is a soft plastic tube with a bevel at one end and a flange at the other. NPAs are typically better tolerated in partly or fully conscious patients than oropharyngeal airways.
Re-assessment
Make sure to re-assess the patient after any intervention.
Breathing
Clinical assessment
Observations
Review the patient’s respiratory rate:
- A normal respiratory rate is between 12-20 breaths per minute
- Tachypnoea is often the first indication of shock due to hypovolaemia
Review the patient’s oxygen saturation (SpO2):
- A normal SpO2 range is 94-98% in healthy individuals and 88-92% in patients with COPD at high risk of CO2 retention
- Hypoxaemia may occur secondary to shock or aspiration pneumonia
Auscultation
Auscultate the chest to screen for evidence of other respiratory pathology (e.g. coarse crackles may be present if the patient has developed aspiration pneumonia or pulmonary oedema secondary to fluid resuscitation).
Investigations and procedures
Arterial blood gas
Take an ABG if indicated (e.g. low SpO2) to quantify the degree of hypoxia.
Chest X-ray
A chest X-ray may be indicated if abnormalities are noted on auscultation (e.g. reduced air entry, coarse crackles) to screen for evidence of aspiration pneumonia. A chest X-ray should not delay the emergency management of UGIB.
Interventions
Patient positioning
If the patient is conscious, sit them upright, which can help with oxygenation.
Oxygen
Administer oxygen to all critically unwell patients during your initial assessment. This typically involves using a non-rebreathe mask with an oxygen flow rate of 15L. You can then trial titrating oxygen levels downwards after your initial assessment. In COPD, target SpO2 levels accordingly (88-92%) and consider using a Venturi mask: 24% (4L) or 28% (4L)
Adequately oxygenating the patient is important. However, be aware of the risks of aspiration if the patient vomits whilst wearing an oxygen mask.
Re-assessment
Make sure to re-assess the patient after any intervention.
Circulation
Clinical assessment
Pulse
Tachycardia is an early sign of volume depletion in the context of UGIB. The patient’s pulse may feel thready secondary to hypovolaemia.
Blood pressure
Hypotension is a late sign and suggests significant blood loss has occurred (>1500ml).
Fluid balance assessment
Calculate the patient’s fluid balance:
- Calculate the patient’s current fluid balance using their fluid balance chart (e.g. oral fluids, intravenous fluids, urine output, drain output, stool output, vomiting) to inform resuscitation efforts
- Reduced urine output (oliguria) is typically defined as less than 0.5ml/kg/hour in an adult
- Urine output is maintained until significant blood loss has occurred (e.g. 1500-2000 mls)
Inspection
Inspect the patient from the end of the bed and note evidence of pallor indicative of anaemia.
Capillary refill time
Assess the patient’s capillary refill time (CRT):
- In the context of UGIB, the CRT may be prolonged (>2 seconds) both peripherally and centrally
- The patient’s peripheries may also feel cool secondary to hypovolaemia and peripheral vasoconstriction
Investigations and procedures
Intravenous cannulation
Insert two large-bore cannulae (14-16G) and take blood tests as discussed below.
Adequate intravenous access is essential in upper gastrointestinal bleeding as patients can rapidly deteriorate with haemodynamic instability, requiring large volumes of fluid and blood to be transfused.
Blood tests
Request a full blood count (FBC), urea & electrolytes (U&E) and liver function tests (LFTs) for all acutely unwell patients. In the context of upper gastrointestinal haemorrhage, also request:
- Group and crossmatch: to confirm the patient’s blood group and request blood products
- Coagulation screen: to screen for coagulopathy and inform resuscitation efforts
Raised urea occurs in the context of UGIB due to the digestion and absorption of blood proteins.
The haemoglobin level is used to guide transfusion.
Interventions
Strict fluid balance
If not already in place, ask for a strict fluid balance to carefully monitor the patient’s fluid status to inform ongoing resuscitation efforts.
Aim for a urine output of greater than 30mls an hour.
Fluid resuscitation
Hypovolaemic patients require fluid resuscitation:
- Administer a 500ml bolus of Hartmann’s solution or 0.9% sodium chloride (warmed if available) over less than 15 mins.
- Administer 250ml boluses in patients at increased risk of fluid overload (e.g. heart failure).
After each fluid bolus, reassess for clinical evidence of fluid overload (e.g. auscultation of the lungs, assessment of JVP).
Repeat administration of fluid boluses up to four times (e.g. 2000ml or 1000ml in patients at increased risk of fluid overload), reassessing the patient each time.
If the patient is losing significant volumes of blood, fluid replacement alone is inadequate, and blood transfusion needs to be arranged (see below).
Seek senior input if the patient has a negative response (e.g. increased chest crackles) or isn’t responding adequately to repeated boluses (i.e. persistent hypotension).
See our fluid prescribing guide for more details on resuscitation fluids.
Blood transfusion
Patients with a significant haemorrhage who are in shock need a balanced transfusion of red cells, platelets and fresh frozen plasma.
This is usually arranged via a massive transfusion protocol which simplifies the ordering and administration of large amounts of blood products (usually at least six units of red cells).
Haemodynamically stable patients should receive red cell transfusion if Hb is <70 g/L with a target Hb of 70 – 100 g/L.
Reversal of anticoagulation
Patients on anticoagulation (warfarin or DOACs) should be discussed with a senior clinician to consider the reversal of anticoagulation. This may require haematology input.
Prothrombin complex concentrate can be used in patients taking warfarin and actively bleeding.
Terlipressin
Terlipressin causes vasoconstriction of the splenic artery, reducing blood pressure in the portal system. It is recommended for all patients with suspected variceal bleeding at presentation. It should be stopped once definitive haemostasis has been achieved.
This should be a consultant-led decision.
Prophylactic antibiotic therapy
Administer prophylactic antibiotics to patients with suspected or confirmed variceal bleeding. Follow local microbiology guidelines. Ciprofloxacin 1g once daily for seven days is a commonly used regime.
Proton pump inhibitors
Proton pump inhibitors (PPIs) reduce the amount of acid the stomach produces. They can also reduce re-bleeding rates in patients with non-variceal upper GI bleeding. However, due to a lack of evidence, NICE currently does not advise routine prescribing of intravenous PPIs before endoscopy.
Endoscopy
Endoscopy should be performed on all unstable patients with severe UGIB immediately after resuscitation. It should be performed within 24 hours of admission for all other patients with UGIB. This allows diagnostic confirmation and treatment of bleeding sites.
Patients should be discussed with the on-call endoscopist.
Re-assessment
Make sure to re-assess the patient after any intervention.
Disability
Clinical assessment
Consciousness
In the context of UGIB, a patient’s consciousness level may be reduced secondary to hypotension or hepatic encephalopathy.
Assess the patient’s level of consciousness using the ACVPU scale:
- Alert: the patient is fully alert
- Confusion: the patient has new onset confusion or worse confusion than usual
- Verbal: the patient makes some kind of response when you talk to them (e.g. words, grunt)
- Pain: the patient responds to a painful stimulus (e.g. supraorbital pressure)
- Unresponsive: the patient does not show evidence of any eye, voice or motor responses to pain
If a more detailed assessment of the patient’s level of consciousness is required, use the Glasgow Coma Scale (GCS).
Pupils
Assess the patient’s pupils:
- Inspect the size and symmetry of the patient’s pupils
- Assess direct and consensual pupillary responses
Drug chart review
Review the patient’s drug chart for medications which may cause neurological abnormalities (e.g. opioids, sedatives, anxiolytics).
Also, look for medications which may worsen bleeding:
- Warfarin
- Direct acting antiocagualants (DOACs): apixaban, rivaroxaban etc.
- Antiplatelets
Investigations and procedures
Blood glucose and ketones
Measure the patient’s capillary blood glucose level to screen for causes of a reduced level of consciousness (e.g. hypoglycaemia or hyperglycaemia).
A blood glucose level may already be available from earlier investigations (e.g. ABG, venepuncture).
The normal reference range for fasting plasma glucose is 4.0 – 5.8 mmol/l.
Hypoglycaemia is defined as a plasma glucose of less than 3.0 mmol/l. In hospitalised patients, a blood glucose ≤4.0 mmol/L should be treated if the patient is symptomatic.
See our blood glucose measurement guide for more details.
Interventions
Maintain the airway
Alert a senior clinician immediately if you have concerns about a patient’s consciousness level.
A GCS of 8 or below, or a P or U on the ACVPU scale, warrants urgent expert help from an anaesthetist. In the meantime, you should re-assess and maintain the patient’s airway, as explained in the airway section of this guide.
Correct hypoglycaemia
Hypoglycaemia should always be considered in patients presenting with a reduced level of consciousness, regardless of whether they have diabetes. The management of hypoglycaemia involves the administration of glucose (e.g. oral or intravenous).
See our hypoglycaemia guide for more details.
Re-assessment
Make sure to re-assess the patient after any intervention.
Exposure
Exposing the patient during your assessment may be necessary. Remember to prioritise patient dignity and the conservation of body heat.
Clinical assessment
Inspection
Inspect the patient for stigmata of chronic liver disease and/or coagulopathy:
- Bruising
- Petechiae (e.g. thrombocytopenia)
- Spider naevi
- Caput medusae
- Ascites
- Evidence of trauma and bleeding from other sites
- Peripheral oedema
Palpation
Perform a brief abdominal examination, which may reveal:
- Ascites secondary to cirrhotic liver disease
- Abdominal tenderness (e.g. duodenal ulcer)
Temperature
Measure the patient’s temperature:
- If fever is present, consider co-existing infection
Rectal examination
Perform a rectal examination to assess for evidence of gastrointestinal bleeding (e.g. malaena).
Interventions
Catheterisation
Catheterise the patient to monitor urine output which can guide fluid resuscitation and the need for escalation.
Re-assessment
Make sure to re-assess the patient after any intervention.
Re-assessment and escalation
Re-assess the patient using the ABCDE approach to identify any changes in their clinical condition and assess the effectiveness of your previous interventions.
Any clinical deterioration should be recognised quickly and acted upon immediately.
Seek senior help if the patient shows no signs of improvement or if you have any concerns.
Escalation
Haemodynamically unstable patients with upper gastrointestinal bleeding will require urgent critical care input. The on-call endoscopist should be contacted to consider an urgent endoscopy.
Use an effective SBAR handover to communicate the key information to other medical staff.
Ongoing management
The UK upper gastrointestinal bleeding care bundle guides the management of a UGIB (Figure 1).
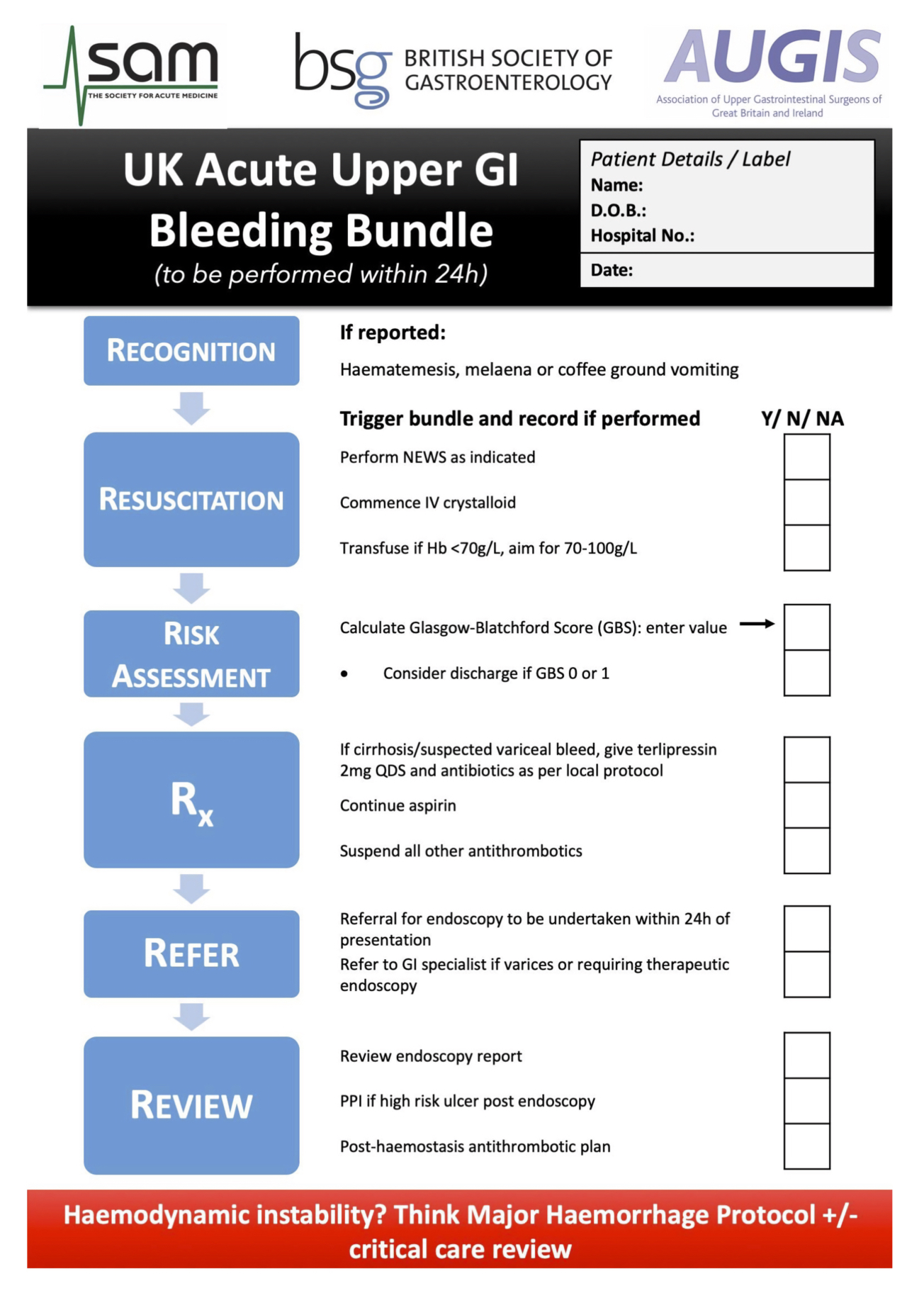
Glasgow-Blatchford score
The Glasgow-Blatchford score (GBS) is calculated before endoscopy and is based on simple clinical and laboratory parameters. Its principal use is to identify low-risk patients who do not require any intervention (blood transfusion, endoscopic therapy, surgery).
Approximately 20% of patients presenting with upper gastrointestinal haemorrhage have a Glasgow-Blatchford score of 0. Such patients can usually be managed as an outpatient, as the mortality in this group is nil.
Rockall score
The Rockall scoring system is used for risk stratification (mortality and risk of rebleeding). Rockall scores can be calculated both before and after endoscopy, but the post-endoscopy Rockall score provides a more accurate risk assessment.
Next steps
Take a history
Revisit history taking to explore relevant medical history, focusing on identifying the cause of upper gastrointestinal bleeding.
See our history taking guides for more details.
Review
Review the patient’s notes, charts and recent investigation results.
Review the patient’s current medications and check any regular medications are prescribed appropriately.
Document
Clearly document your ABCDE assessment, including history, examination, observations, investigations, interventions, and the patient’s response.
See our documentation guides for more details.
Discuss
Discuss the patient’s clinical condition with a senior clinician using an SBAR handover.
Questions which may need to be considered include:
- Are any further assessments or interventions required?
- Does the patient need a referral to HDU/ICU?
- Does the patient need reviewing by a specialist?
- Should any changes be made to the current management of their underlying condition(s)?
The next team of clinicians on shift should be informed of any acutely unwell patient.
References
- NICE. Acute Upper Gastrointestinal Bleeding Management. Updated 2016. Available from: [LINK].
-
