

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Bone tumours describe lesions formed by abnormal tissue growing in bone. They can be divided into primary and secondary as well as benign and malignant. There are further grading systems that address the complexity of bone tumours.
Primary bone tumours refer to bone tumours originating from mesenchymal tissue. Secondary (metastatic) bone tumours refer to metastases originating from other tumours in the body that spread to the bone via the bloodstream.
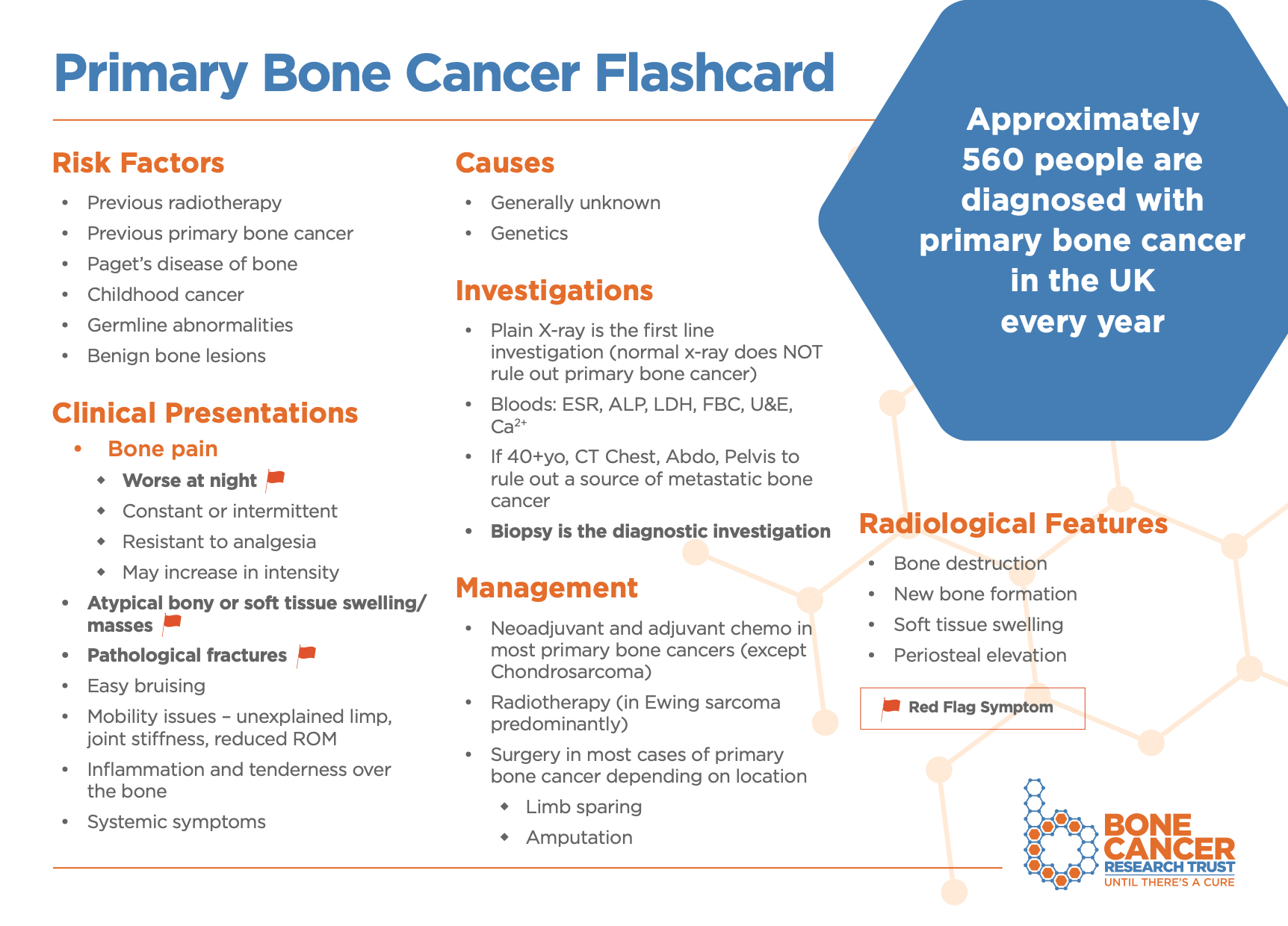
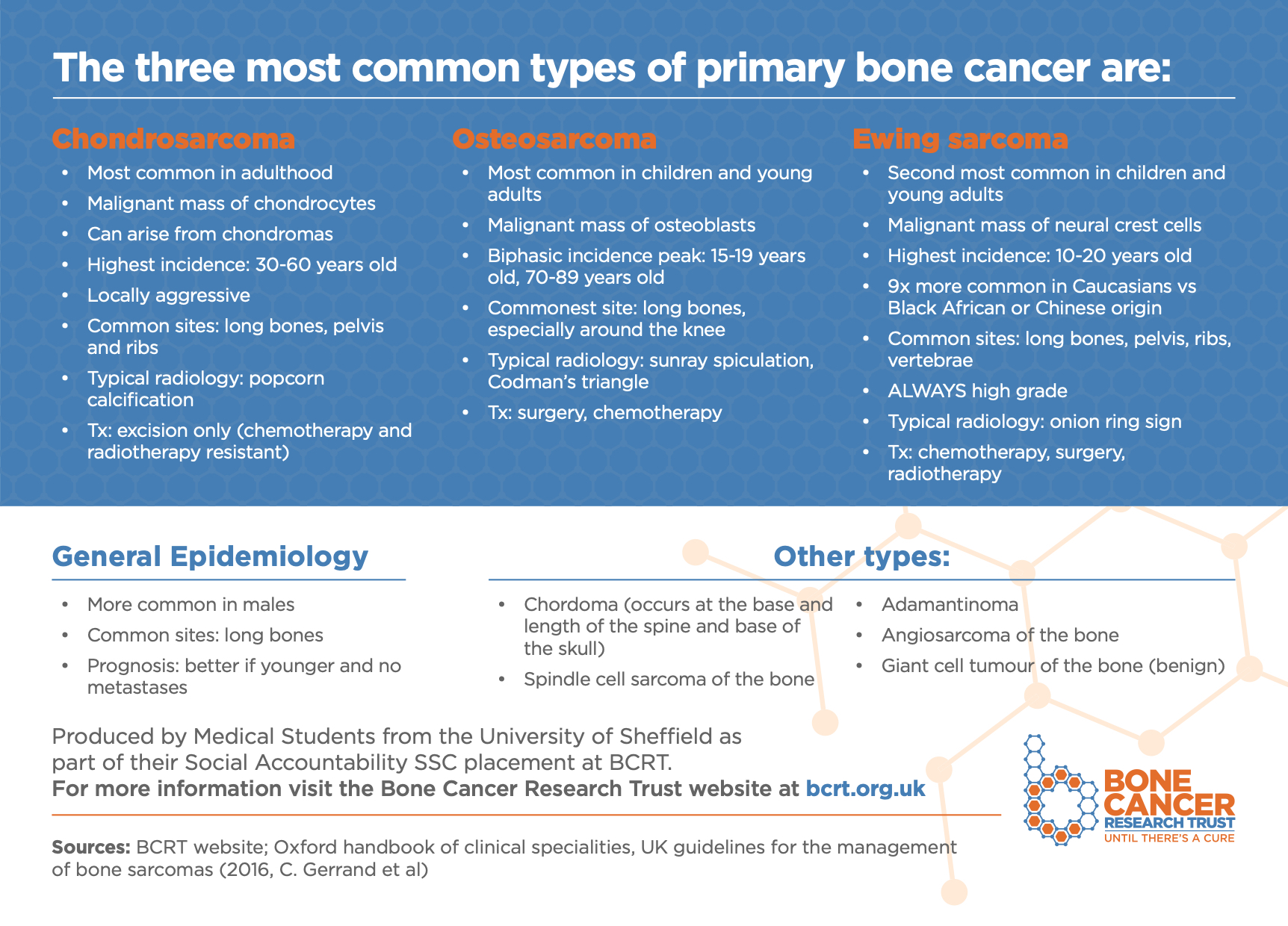
See the Bone Cancer Research Trust’s flashcard below which summarises the three most common types of primary bone cancer and download the PDF version here.
Epidemiology
Primary bone tumours account for less than 1% of total cases of cancer and are far less common than secondary bone tumours.1
Primary bone tumours have two to three peaks in their incidence: one between 0 and 20 years, another between 20 and 40 years and finally one after 50 years. Secondary bone tumours tend to occur in adults over the age of 40. There appear to be no differences across genders.
Bone tumours are often discovered in an incidental radiograph which accounts for difficulties encountered in calculating prevalence and incidence in epidemiological studies.
Currently, the risk factors and causes are largely unknown.
Aetiology
To understand how bone tumours arise and how they are classified, it’s important to understand the composition of bones.
Bones are made of organic and non-organic components. The non-organic component consists of calcium hydroxyapatite crystals. This gives bone its characteristic hardness. The organic component consists of an osteoid matrix (composed of ground substance and collagen fibres) and the following cells:2
- Osteogenic cells: bone stem cells located in the periosteum and endosteum. These cells differentiate into osteoblasts.
- Osteoblasts: lay bone matrix around themselves (“build bone”) until they become trapped and become osteocytes.
- Osteoclasts: derived from monocytes, their function is to resorb bone in response to hormonal signalling (“break down bone”).
- Osteocytes: these are mature osteoblasts that maintain the integrity of bone tissue.
There are other types of cells present, such as chondrocytes which produce cartilage (present at the ends of bones) and fibrocytes which are derived from haematopoietic cells present in the bone marrow.
From these types of cells, bone tumours can be classified based on their histology (Table 1).
Table 1. The classification of bone tumours according to histology.3
|
|
Benign |
Malignant |
|
Osteogenic (bone-forming) |
Osteoid osteoma Osteoma Osteoblastoma
|
Osteosarcoma:
|
|
Chondrogenic (cartilage forming) |
Chondroma Enchondroma Osteochondroma Chondroblastoma Chondromyxoid fibroma |
Chondrosarcoma:
Malignant chondroblastoma |
|
Giant-cell tumour |
Osteoclastoma Giant cell tumour Malignant giant cell tumour |
|
|
Marrow |
Ewing’s sarcoma Reticulosarcoma Lymphosarcoma Multiple myeloma |
|
|
Tumour-like lesions |
Simple bone cyst, aneurysmal bone cyst, fibrous dysplasia, myositis ossificans, brown tumour, intraosseous epidermoid cyst, giant cell granuloma |
|
|
Secondary (metastatic): breast, prostate, thyroid, renal, lung, bowel cancer. |
||
Location
Bone tumours have a predilection for certain parts of bones (table 2).
Table 2. The classification of bone tumours according to location.4
|
Long bones |
|
|
Epiphysis |
Giant cell tumour, chondroblastoma, clear cell chondrosarcoma, osteochondroma |
|
Metaphysis |
Conventional osteosarcoma, Ewing sarcoma, primary chondrosarcoma, osteochondroma, chondroma, osteoid osteoma, giant cell tumour |
|
Diaphysis |
Periosteal osteosarcoma, Ewing sarcoma, osteoid osteoma, primary chondrosarcomas, chondroma, multiple myeloma |
|
Flat bones |
Ewing sarcoma, secondary chondrosarcoma |
Structure and composition of bone
Where the tumour occurs in a bone reflects the structure (figure 1) and normal development of the bone (figure 2). Knowing the differences can aid diagnosis and management.
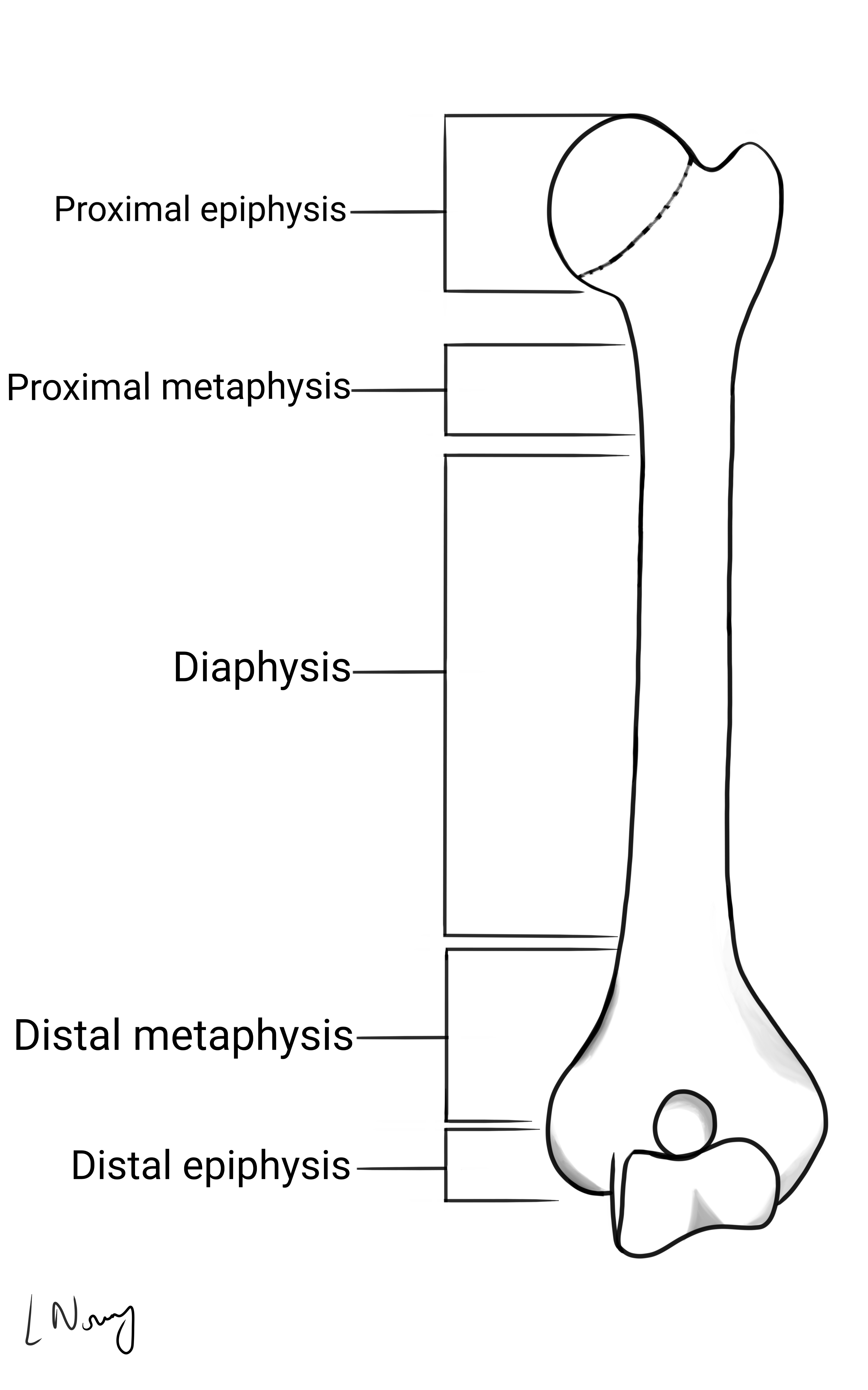

Metaphyseal lesions tend to be either secondary (metastatic) bone tumours due to an extensive blood supply or, multiple myeloma due to the presence of haematopoietic cells. 7,8,9
An epiphyseal lesion in a skeletally mature individual suggests a giant-cell tumour whereas an epiphyseal lesion in a skeletally immature individual points to chondroblastoma.4
Clinical features
History
Typical symptoms of bone tumours include:7,8
- Pain (progressive, activity-related, at rest or worse at night)
- Soft tissue or bony swellings
- Limp
- B symptoms: weight loss, fever and night sweats
Other important areas to cover in the history include:
- History of trauma (e.g. any fractures, minor injuries)
- Family history
- Previous medical and surgical history (e.g. previous malignancy, pre-existing bone diseases and previous radiotherapy treatments)
Bone tumours also have a peak incidence across different ages, so age is especially important in narrowing down the differential diagnoses (table 3).
Table 3. The epidemiology of different bone tumours.
|
Tumour |
Children |
Adults |
Elderly |
|
Simple bone cyst |
+ |
+ |
|
|
Ewing’s sarcoma |
+ |
+ |
|
|
Osteosarcoma |
+ |
+ |
|
|
Osteoid osteoma |
+ |
+ |
|
|
Chondromyxoid fibroma |
+ |
+ |
|
|
Aneurysmal bone cyst |
+ |
+ |
|
|
Chondrosarcoma (low grade) |
|
+ |
|
|
Chondroma |
|
+ |
|
|
Giant cell tumour |
|
+ |
|
|
Fibrosarcoma |
|
+ |
+ |
|
Secondary bone metastasis |
|
|
+ |
|
Multiple myeloma |
|
|
+ |
|
Chondrosarcoma (high grade) |
|
|
+ |
|
Osteosarcoma (Paget’s disease) |
|
|
+ |
Clinical examination
Where bone tumours are suspected, a thorough examination of the affected limb is necessary. See the Geeky Medics guides here for further information.
Typical clinical findings in bone tumours include:
- Neurovascular dysfunction: paraesthesia and reduced temperature in the affected limb (a large bone tumour can press on surrounding nerves and vessels)
- Swelling: may be painless or tender (note the size and consistency)
- Deformity
- Limp
- Local mechanical problems (painful movements or decreased range of joint motion)
- Signs of a fracture
- Systemic symptoms (e.g. unintentional weight loss and fatigue)
- Local lymphadenopathy
Some bone tumours are clinically silent and are only discovered in an incidental radiograph.
Differential diagnoses
There are many other conditions that present in a similar way to bone tumours: 7,8
- Tumour-like lesions: such as simple bone cyst and aneurysmal bone cyst.
- Osteomyelitis: lab investigations will show increased inflammatory markers. Biopsy of affected tissue sent for microbiological analysis will confirm the diagnosis.
- Stress fracture: typically, a young patient presenting with local pain near a joint. Radiographs will show the destruction of cortex but with overlying new bone formation.
- Healing fracture: radiographs show callus formation.
- Gouty tophi: patients will typically present with an inflamed joint, commonly in the lower limbs. Radiographs can show joint effusion and bone destruction. Blood tests will show an increased uric acid level.
- Eosinophilic granuloma: also known as Langerhans cell histiocytosis. Clinically resembles osteomyelitis. Biopsy reveals Langerhans cell proliferation and an increased number of inflammatory cells (e.g. eosinophils).
- Brown tumour: a result of hyperparathyroidism and histologically resembles giant cell tumour. Lab investigations will demonstrate elevated parathyroid hormone and/or blood calcium.
With all differential diagnoses, MRI is an important investigation in correctly diagnosing the lesion.
Investigations
History and radiological findings are often sufficient to obtain a diagnosis.
Conventional radiography
Conventional radiography plays a key role in the detection, diagnosis, staging and follow-up of bone tumours.9
Imaging must be interpreted in the context of clinical history and examination. Plain X-rays (in AP and lateral) of the bone in question are the most useful.
Interpreting radiographs
When interpreting radiographs, it’s useful to keep the following questions in mind: How does the tumour affect the bone and how does the bone react to the tumour?
Is it radiodense (sclerotic) or radiolucent (lytic/fibrous)?
What is the border and zone of transition around the lesion like?
- Are the borders clearly demarcated or ill-defined?
- Are the borders thicker (sclerotic)?
- Is the zone of transition small or large?
What is the condition of the cortex?
- Is it intact, eroded, broken or expanding?
Is there a periosteal reaction and if so, of what pattern?
Does the bone lesion extend into the surrounding soft tissues?
What is the matrix in the lesion like?
Are there skip lesions?
Benign vs malignant lesions
It is important to remember that benign lesions grow slowly while malignant lesions grow much faster. Bone formation is very slow and changes to the bone can indicate whether the lesion is likely to be benign or malignant. 9
Border: a benign lesion will have a clear and well-defined margin whereas a malignant lesion will have an ill-defined margin.
Zone of transition around the lesion: if the zone of transition is small it is more likely to be benign. If the zone is large it is more likely to be malignant.
Condition of the cortex: a destroyed cortex is a sign of malignancy (caused by tumours growing very fast and breaking through the cortex). If the cortex is intact but looks like it’s expanding, then this suggests an aggressive benign lesion (e.g. giant-cell tumour).
Pattern of periosteal reaction: the periosteum around bones react non-specifically to the presence of pus (in infections), blood (in trauma) and tumours. Periosteal reactions can be divided into benign and aggressive patterns (figure 3). With benign patterns, the bone has time to adapt and lay down bone and periosteum over the lesion, giving rise to a solid and even periosteum. Malignant bone tumours do not produce a benign periosteal reaction. Instead, they may have an aggressive periosteal reaction, where the periosteum didn’t have enough time to accommodate the fast-growing malignant lesion. In some cases, there may be no visible periosteal reaction.
Extension into the surrounding soft tissues signifies an aggressive, most likely malignant lesion.
Matrix: matrix signifies the substance inside the lesion of which there are two types: chondroid and osteoid matrix. These are produced by the chondrogenic and osteogenic tumours respectively. Each has their own distinctive appearance on radiographic images: chondroid matrix taking on a popcorn-like appearance and osteoid matrix taking on a cloud-like density.
Skip lesions: skip lesions are separate foci of tumour cells that develop within the same affected bone or across an adjacent joint. Bone tumours that can cause skip lesions include metastatic bone tumours, osteosarcoma and multiple myeloma.

Table 4. Distinguishing benign and malignant bone tumours.
| Benign | Malignant | |
| Border | Clear, well-defined | Ill-defined, not clear |
| Zone of transition | Small | Large |
| Cortex |
Intact Intact but expanding: aggressive benign |
Destroyed |
| Periosteal reaction | Benign | Aggressive |
| Extension into the soft tissue | No | Yes |
Although conventional radiography can be very useful in the diagnosis of bone tumours, a normal radiograph does not exclude bone tumours. 40-50% of bone must be destroyed before a distinct area of radiolucency can be revealed.11
Other radiological investigations
CT, MRI and radioisotope scans are only required in specific cases:
- CT (chest, abdomen and pelvis): to look for metastases or primary lesions.
- MRI: assesses the extent of bone tumour and any soft tissue extension. MRI is the gold standard.12
- Radionuclide bone scans: uses Technetium-99m as an active agent to detect and follow-up bone metastases. Malignant and secondary bone tumours have high metabolic activity, so they will take up the radionuclides and appear as black areas on the bone scan.
Laboratory investigations
Baseline blood tests (FBC, U&E, coagulation, CRP): aids differential diagnosis. Microcytic anaemia is present in patients with multiple myeloma. CRP and WBC can be raised in osteomyelitis.
Serum ESR: ESR may be raised in osteomyelitis, osteosarcoma, Ewing’s sarcoma, multiple myeloma and secondary bone tumours.
Serum LDH: increased in secondary bone tumours.
Bone profile blood test: evaluates the bone turnover process. ALP (a marker of osteoblast hyperactivity) is increased in bone tumours, especially osteosarcoma. Serum albumin levels are abnormal in multiple myeloma. Serum calcium may be increased in multiple myeloma and secondary bone tumours.
Other tests:
- Urinalysis: Bence-Jones protein is present in patients with multiple myeloma.
- Tests for tumour markers confirming the origin of metastasis (e.g. increased prostatic acid phosphatase levels in prostate carcinoma).
Biopsy
Patients must be referred to the bone sarcoma multidisciplinary team (MDT) before taking a biopsy, in order to aid diagnosis and treatment.11 There are only 5 bone tumour units in the UK – Stanmore, Birmingham, Oswestry, Oxford and Newcastle.
A biopsy is necessary for confirmation of diagnosis and planning of treatment. This is usually an ultrasound or CT guided core needle biopsy. A biopsy track is chosen that later can be excised at the definitive operation.
If bone is removed, the defect must be covered with bone wax or methylmethacrylate cement. Avoid using drains as they increase the risk of tumour contamination.
Complications of bone biopsy
Bone biopsy is not a minor procedure and so risks must be fully explained to the patient before obtaining consent. Complications of bone biopsy include:
- Tumour contamination
- Haemorrhage
- Wound breakdown
- Infection
- Pathological fracture
In the case of benign tumours, excisional biopsy where the entire lesion is removed can be considered. However, in the case of malignant tumours, detailed imaging of the lesion must be obtained before carrying out the biopsy (as the biopsy might alter the appearance of the lesion on imaging).
Tissue samples must be sent for histological and microbiological analysis (necessary to exclude osteomyelitis).
Staging of bone tumours
There are currently two staging systems used for bone tumours: TNM and Enneking systems.4, 11, 13
The Enneking system
Based on histological grading, location of the tumour and metastases.
Grading is from G0 to G2:
- G0 – non-cancerous (benign)
- G1 – low-grade tumour
- G2 – high-grade tumour
Bone tumours are also divided into 3 stages: stage 1 is low grade, stage 2 is high grade and stage 3 denotes that the tumour has metastasised.
Stages 1 and 2 are further divided into A and B:
- A – the tumour is contained within the bone
- B – the tumour has broken through the bone wall
Table 5a. The Enneking staging system
| Benign | |||
| Latent: low biological activity; clear margin; often incidentally found; can heal spontaneously; low recurrence | |||
| Active: symptomatic; defined margins but can have partial bone destruction with cortical thinning; may present with pathological fracture; low recurrence | |||
| Aggressive: unclear margins; bone destruction/soft tissue extension; growth is not limited by surrounding natural barriers; low risk of metastases and high risk of recurrence |
Table 5b. The Enneking staging system
| Malignant | |||
| Stage | Grade | Site | Metastases |
| IA | G1 | T1 (intracompartmental) | M0 |
| IB | G1 | T2 (extracompartmental) | M0 |
| IIA | G2 | T1 | M0 |
| IIB | G2 | T2 | M0 |
| III | Any | Any | M1: Regional or distant metastases |
Management
NICE recommends that all patients with bone tumours must be promptly referred to a sarcoma multidisciplinary team (MDT) for an expert diagnosis; to establish a unique care plan with suitable support and rehabilitation services and for treatment to be arranged and provided by the specialist MDT.14,15
The principles of bone tumour management are:
- Early detection and treatment
- Prevent recurrence
- Minimise complications
- Avoid long term disability by preventing or fixing pathological fractures
- Prevent metastases
Surgical management
For benign lesions, treatment options include:
- Curettage
- Excisional biopsy
- Complete local excision.
For malignant lesions, histological diagnosis, the grade of malignancy and staging must first be confirmed through biopsy. Treatment options include:
- Limb sparing surgeries: local excision and wide excision.
- Radical surgeries: resection with prosthetic replacement and amputation with prosthetic replacement.8
Medical management
Medical management involves adjuvant therapy in the form of radiotherapy and chemotherapy:8, 11
- Pre-operative combination chemotherapy
- Local surgery
- Postoperative adjuvant chemotherapy
Molecular therapy can also be used, especially in the treatment of giant cell tumours. Denosumab, a human monoclonal antibody, targets cells in the tumour expressing RANK ligands thus blocking the maturation of osteoclasts and halting bone destruction.16, 17
Benign bone tumours
Osteoid osteoma
An osteoid osteoma is a small (<1cm) osteogenic benign tumour often seen in patients under the age of 30. It often occurs in long bones (e.g. femur, tibia) in the diaphysis or metaphysis of the affected bone. Patients typically experience pain at the tumour site, which is usually worse at night and relieved by nonsteroidal anti-inflammatories (a diagnostic hallmark due to increased levels of COX enzymes and PGs in the lesion).
Pathologically, the lesion is formed of osteoid matrix and freshly laid bone. Radiological features include a nidus with benign periosteal reaction (figures 4a and 4b). The tumour may spontaneously resolve but can also be managed with local excision.
Chondroma
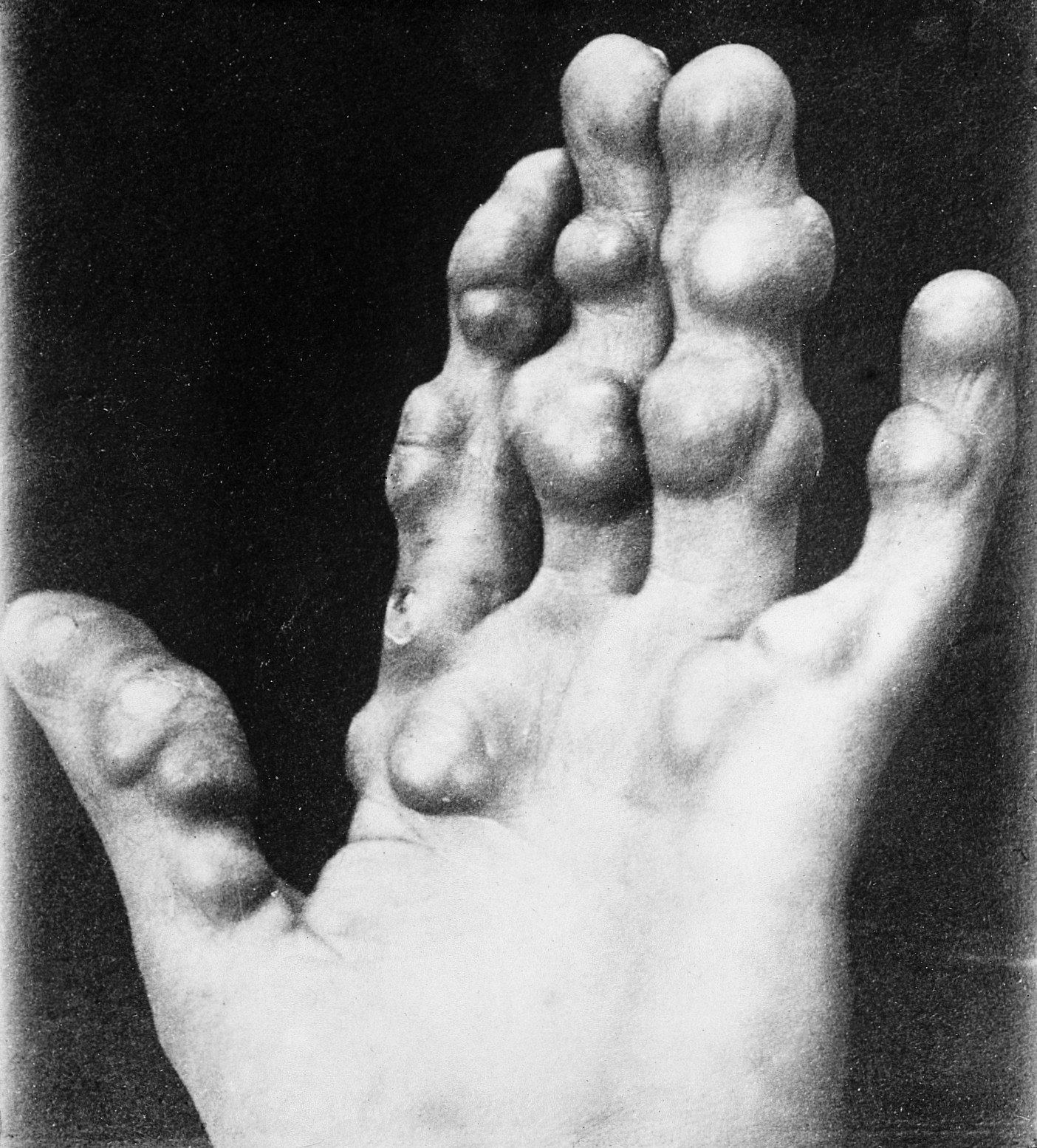
A chondroma is a chondrogenic benign tumour (varying sizes) that can be seen at any age, but usually in patients aged between 15 and 50. Chondromas commonly occur in bones of the hands and in the diaphysis or metaphysis of the bone, where they are termed enchondromas.
They are largely asymptomatic but causes obvious deformity. It can present as a single lesion or as multiple lesions, as part of dyschondroplasia and other disorders such as Ollier disease and Maffucci’s syndrome, leading to fractures and reduction of limb length.20
In conventional radiography, there is a central, expanded radiolucent area. It can be distinguished from a lytic lesion due to the presence of chondroid matrix appearing as flecks of calcification (figures 5a and 5b).
Treatment involves close follow up if asymptomatic. If it grows in size, becomes painful, or is at risk of causing a pathological fracture – the tumour should be removed by curettage and the defect filled with bone graft.
Chondromas, although benign, have a small risk of malignant change to chondrosarcoma.

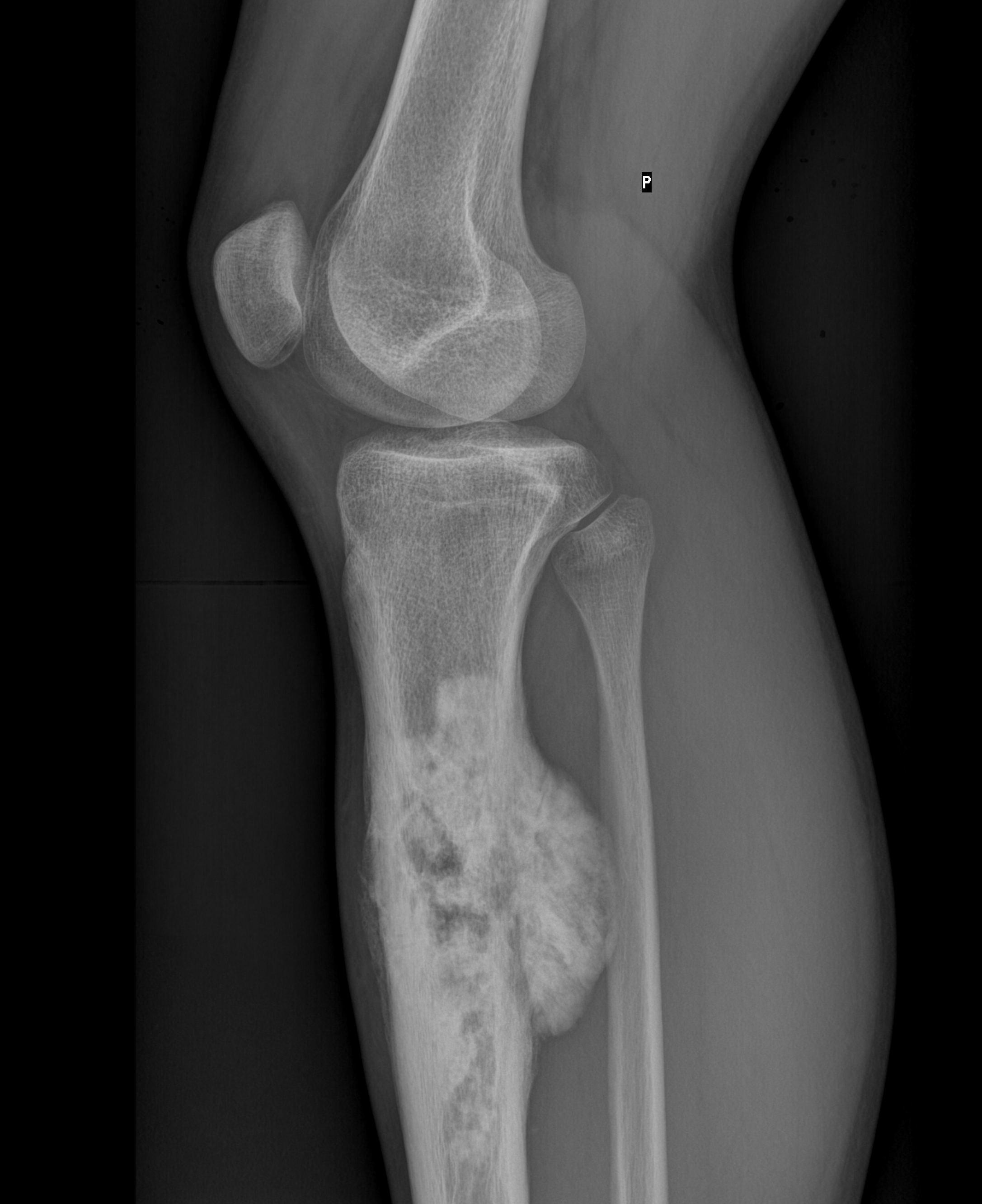
Osteochondroma
This chondrogenic tumour typically presents in young patients aged between 10 and 20. It develops from the epiphysis growing into the metaphysis of long bones, growing away from the joint. (figure 6).
Osteochondromas are suspected to be a developmental lesion as they develop at the ends of the bones at the epiphyseal plate and become a bony prominence by endochondral ossification. Osteochondromas are covered by a layer of hyaline cartilage, called a cartilage cap. The thickness of the cartilage cap is linked to malignant transformation.23
The genetic disorder multiple hereditary exostoses are characterised by multiple osteochondromas resulting in bone growth disruption.24
Tumour growth follows the patient’s growth and when the patient stops growing, the lesion stops growing too. If the lesion continues to grow, malignancy must be suspected.
These tumours are painless but can compress nearby neurovascular structures or tendons or ligaments.
Treatment involves local excision if the tumour is symptomatic.

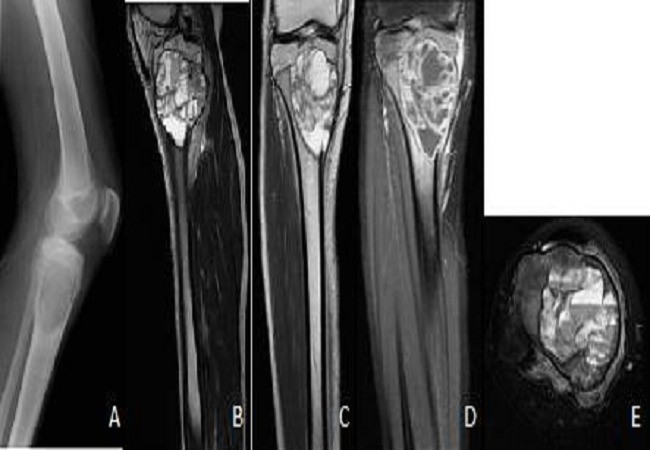
Giant cell tumour
Although benign, this is a locally aggressive, osteolytic bone tumour derived from osteoclasts. Giant cell tumours commonly affect adults aged between 20 to 40 and are usually located in the epiphysis and metaphysis (after the growth plate has fused) of long bones.
Patients complain of pain and swelling at the end of a long bone. In some cases, presenting with a pathological fracture.
On X-rays, the tumour almost always is located under the sealed growth plate (figure 7). A unique classification of GCT is the Campanacci grading system which is based on radiological features of the tumour (Table 6).26
CT and MRI are required for further analysis and to see if the joint surface has been compromised. A biopsy of the tumour is also needed to confirm the diagnosis and rule out malignancy.
Table 6. Campanacci grading system.
|
Grade |
Description |
|
1 |
Well circumscribed lesion. Thin but intact cortex. No aggressive features (e.g. periosteal reaction). |
|
2 |
The lesion has well-defined borders, but a radio-opaque rim is absent. |
|
3 |
Indistinct borders with cortical bone destruction and soft tissue extension. |
If the tumour is slow-growing with benign histology, treatment will involve curettage and adjuvant therapy (e.g. burring, liquid nitrogen, phenol, polymethyl methacrylate bone cement etc).4 This is then followed by packing with bone graft.
However, if the tumour is aggressive with a high risk of local recurrence, local excision and replacement with bone grafting or prosthesis is recommended.

Malignant bone tumours
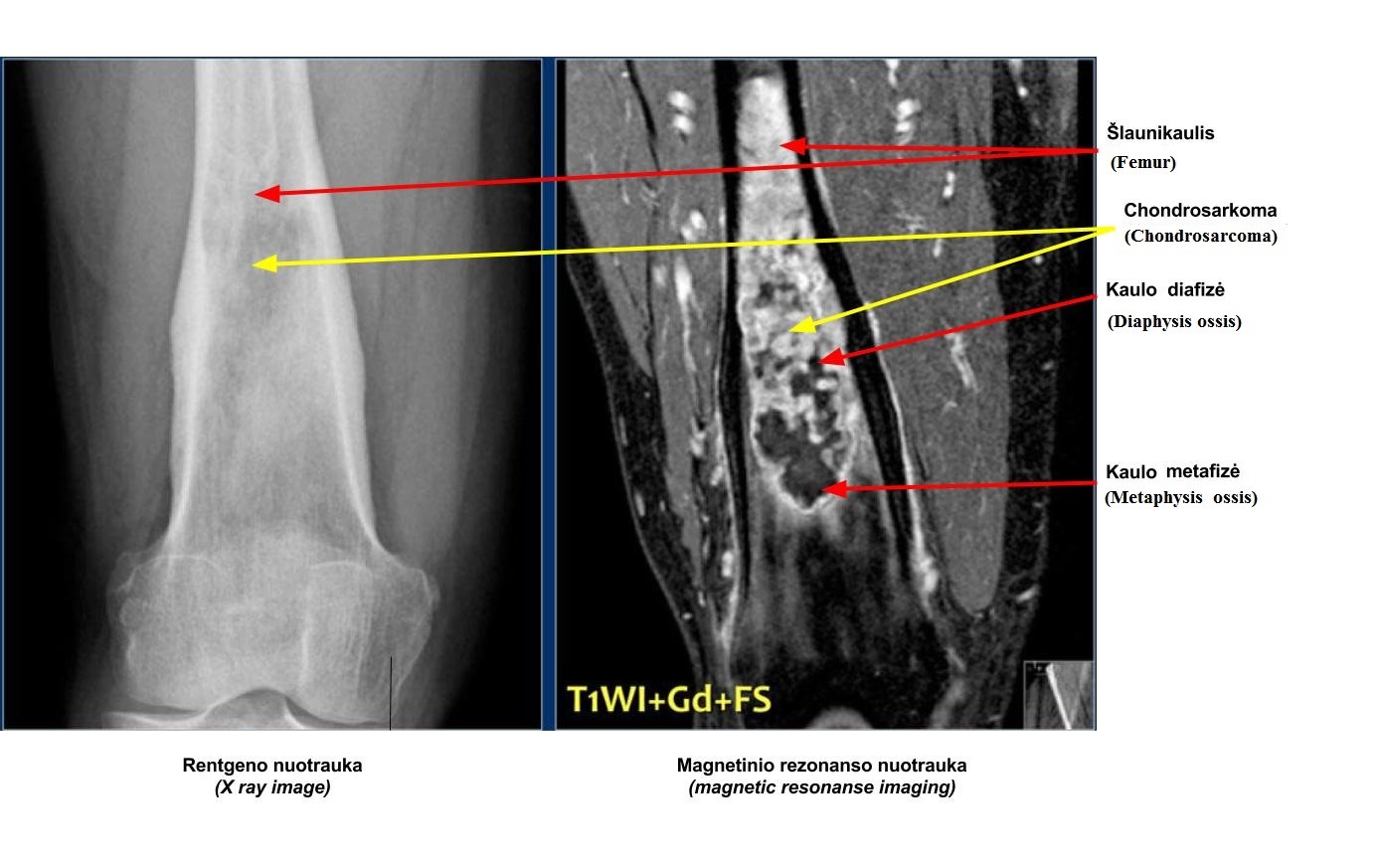
Chondrosarcoma
Chondrosarcoma commonly occurs in patients aged 30 to 60, with men being more affected. There are two types: primary chondrosarcoma and secondary chondrosarcoma.
Primary chondrosarcomas typically develop in the centre of metaphysis and diaphysis of long bones such as the femur, tibia or humerus. Secondary chondrosarcomas usually develop in the peripherally of flat bones (e.g. scapula and sacrum). They can arise from pre-existing osteochondromas that have transformed to chondrosarcomas over time.
Patients complain of a progressive, dull, aching pain and a gradually enlarging lump in the affected area.
On X-rays, chondrosarcomas appear as a radiolucent area with central flecks of calcification, a characteristic of chondroid matrix (figure 8). CT and MRI are needed to assess the soft-tissue extension of the tumour before performing a biopsy.
Chondrosarcomas are not responsive to chemotherapy or radiotherapy, so surgery is the only option. Resection with wide surgical margins followed by prosthetic replacement is required. Amputation sometimes may be necessary.
Osteosarcoma
This malignant tumour commonly affects young patients aged between 10 and 25 but also can occur in older adults over 60 as a complication of Paget’s disease, pre-existing bone lesions or radiation exposure.
Osteosarcoma often occurs at sites of rapid bone growth, in the metaphysis or diaphysis of the distal femur, proximal tibia and proximal humerus.
Patients complain of progressive pain and pain at night. Clinical examination may reveal soft tissue or bony swelling.
The radiological features of osteosarcoma are unique: the radiolucency of the tumour alternates between areas of lysis and areas of increased bone density.
The margins are poorly defined and there’s an aggressive periosteal reaction, in particular a sunburst pattern or Codman’s triangle. The tumour often breaks through the cortex and there’s usually soft tissue extension (figure 9).
If the suspicion for osteosarcoma is high, a biopsy is necessary to exclude other diagnoses. Once the diagnosis is confirmed, an MRI of the whole bone including above and below the adjacent joint is needed to check for skip lesions and to stage the tumour. Whole-body MRI and CT chest to check for distant metastases are also required.
Treatment consists of pre-operative chemotherapy followed by wide resection or amputation. Chemotherapy is continued postoperatively for 6 months to a year. If metastases are present, these can be assessed individually, but can often include resection.
Ewing’s sarcoma
Ewing’s sarcoma is a bone tumour of childhood, commonly affecting patients between 5 and 20 years. The cell origin of the sarcoma is unknown but the current theory points to mesenchymal stem cells with the chromosomal translocation t(11;22)(q24;q12) resulting in the EWSR1-FLI1 fusion protein.30, 31
Tumours commonly arise in the diaphysis or metaphysis (less common) of tibia, fibula, clavicle or humerus. Patients present with throbbing pain and swelling. They may be generally unwell with pyrexia, fatigue and weight loss.
Plain X-ray imaging reveals an area of bone destruction chiefly in the mid-diaphysis. An aggressive periosteal reaction in a distinctive onion-peel pattern is characteristic of Ewing’s sarcoma (figure 10). Skip lesions can also be present in the same bone at presentation.
CT and MRI of the bone, as well as whole-body MRI, are needed to assess the extent of the sarcoma, soft tissue extension and detect metastases. A biopsy is also necessary to confirm the diagnosis.
Prognosis is poor as the sarcoma can metastasise early. However, pre-operative chemotherapy/radiotherapy followed by wide excision and further chemotherapy for up to 1 year can produce good results.

Multiple myeloma
Multiple myeloma is a tumour of haematological origin, specifically transformed malignant B-cells. Consequent effects on bone are due to plasma cell proliferation and invasion with induced osteoclastic activity leading to widespread osteoporosis and lytic lesions all over the skeleton.
Multiple myeloma commonly arises in bones with active residual red marrow (e.g. shoulders, ribs, hips, or spine). Patients are typically aged between 45 and 70 years and present with weakness, back pain, bone pain, thirst and polyuria (due to hypercalcaemia). Patients may also present with pathological fractures or spinal cord compression (e.g. cauda equina syndrome) if a vertebral body is involved.
The radiological features of multiple myeloma include widespread osteoporosis and punched-out holes in the axial and appendicular skeleton (figures 11a to 11d). Crushed vertebral bodies are sometimes demonstrated.
For patients under 65 years of age, treatment involves cycles of induction chemotherapy followed by autologous/allogeneic stem cell transplantation.33 For patients over 65 years or with serious comorbidities, chemotherapy alone is given. Prophylactic/treatment of pathological fractures is also offered. Spinal fractures can cause spinal cord compression and require immediate stabilisation.




Metastatic bone disease/secondary bone tumours
Secondary bone tumours commonly affect adults aged over 50 years. Common primary lesions include malignancies affecting the breast, prostate, kidney, lung, thyroid, bladder and bowel. In some cases, no primary lesion is ever found (known as a CUP – cancer of unknown primary). Nowadays, as detection and treatment of primary bone lesions improve, an increase in pathological fractures secondary to metastases is being observed.
Bony metastases tend to be located in bones that have a rich blood supply (e.g. vertebrae, ribs, pelvis, proximal humerus and proximal femur).
The typical clinical presentation is pain. If the spine is involved, the patient may also present with neurological symptoms consistent with compression of local nerve roots and/or spinal cord.
Patients may also present with pathological fractures due to tumour-induced osteolysis. Symptoms of hypercalcaemia (a useful adage: bones, stones, groans and moans) may also be present.
The radiological features of secondary bone tumours vary. In some cases, there are areas of bone destruction. In others, sclerosis (a marked thickening of the bone) can be seen (figures 12a and 12b).
If plain X-rays are negative, but history and clinic examination highly suggest a secondary bone tumour, a radionuclide bone scan should be carried out.
Initial treatment involves identifying and correcting hypercalcaemia. Combined surgery and radiotherapy of a single secondary bone tumour with its primary parent lesion can be curative. Certain primary lesions can be treated with hormone therapy (e.g. breast and prostate cancer metastases).
Prophylactic fixation or internal fixation of pathological fractures can be considered.
However, if the patient is terminally ill or there are other secondary tumours for which prognosis is poor, palliative care in the form of radiotherapy to control growth/reduce pain, analgesics and corticosteroids to reduce pain/swelling are recommended.


Tumour-like lesions
These are bone lesions that grossly resemble bone tumours however are non-neoplastic.
Simple bone cyst
Simple bone cysts (also known as unicameral bone cysts) commonly affect children and adolescents. They occur in the diaphysis of long bones (e.g. proximal humerus or femur).
The cyst may be expanded equally in all directions. The contents of the cyst are clear and they are largely asymptomatic however they can occasionally cause pathological fractures.
Plain X-ray shows a confined area of radiolucency with a thin sclerotic zone. The cortex above the cyst is thin and there may be a broken piece of cortical bone floating in the cyst (fallen leaf/fragment sign) which is pathognomonic for SBC (figure 13).
Some cysts are asymptomatic and small enough to spontaneously heal after the patient reaches skeletal maturity. However, in large cysts, decompression is important and will involve curettage and grafting. Other interventions include percutaneous aspiration of the cyst or a corticosteroid injection. Presently, there is no single preferred treatment, and management is customised to each patient. Pathological fractures are treated according to its characteristics.

Aneurysmal bone cyst (ABC)
N.B. ‘Aneurysmal’ refers to bone expansion, there is no relation to vascular aneurysms.
This type of bone cyst also commonly occurs in children and young adults. The cyst contains blood and is restricted by a thin cortex and the periosteum. As such, on X-ray images, the affected area looks very expanded with a ‘blown-out’ appearance.
Unlike a simple bone cyst, aneurysmal bone cysts are not located in the centre of the bone. CT and MRI may show fluid levels (a characteristic feature) and demonstrate the extent of cortical destruction (figure 14).
Changes that resemble ABC can occur in aggressive malignant bone tumours (e.g. telangiectatic osteosarcoma). Moreover, ABC changes can develop as a consequence of other distinct primary bone tumours which can alter management. Such cases must be referred for management at a specialist centre with a sarcoma MDT for biopsy to obtain a correct diagnosis.41 42
Management involves curettage and bone grafting. Sometimes the graft is reabsorbed and the cyst reoccurs, so further operations are required.
Complications
Complications of untreated bone tumours include:
- Pain
- Peripheral nerve and vessel compression
- Pathological fractures
- Malignant transformation of a previously benign tumour
- Metastasis
- Hypercalcaemia
- Cachexia
- Uncertainty of diagnosis
- Further tumour growth
Complications of surgical management include:
- Pain
- Loss of function
- Blood clots
- Prosthesis failure
- Tumour contamination
- Bleeding
- Infection
- Tumour recurrence
- Neurovascular damage
- Scarring/swelling/stiffness
- Wound issues including delayed wound healing
- Further surgery: due to patient growth, implant failure, aesthetics, wound breakdown and recurrence
Complications of medical management include:
- Impaired wound healing (where radiation is used)
- Increased risk of infection (when combined with surgery)
- Radiation-induced malignancy
- Bone marrow suppression
- Inflammation and ulceration of mucosal surfaces
- Compromised function of other organs
- Gastrointestinal symptoms (nausea, vomiting, constipation, diarrhoea)
- Hearing loss
Prognosis
Benign bone tumours have a good prognosis, owing to their slow growth rate and low risk of malignant transformation.
Conversely, malignant bone tumours can be aggressive and by the time the patient presents with clinical symptoms suggestive of a primary malignant bone tumour, they may already have metastases. Such patients have a poor prognosis.
Secondary bone tumours also carry a poor prognosis, especially where there is more than one metastasis.
Follow-up
Even after treatment, bone tumours can reoccur locally or develop metastatic changes. Furthermore, surgical reconstruction can fail or result in a decrease in function. Follow-up consists of a physical examination of the tumour site, an assessment of function and complications of surgical reconstruction, local imaging and chest X-ray/CT. As complications and local recurrences can arise more than a decade after the initial diagnosis, there currently is no widely accepted duration of follow-up.11, 44
Key points
- Bone tumours involve neoplastic tissue growing in bone.
- Primary bone tumours refer to bone tumours originating from mesenchymal cells in bone.
- Secondary (metastatic) bone tumours refer to metastases originating from other tumours in the body that spread to the bone.
- Common symptoms include pain, swelling, deformity and limp.
- Common clinical findings include painful movements or decreased range of movement; loss of/abnormal sensation and unintentional weight loss and/or fatigue.
- Conventional radiography plays an important role in the detection, diagnosis, staging and follow-up of bone tumours.
- Other differential diagnoses to consider include osteomyelitis, stress fracture, healing fracture, gouty tophi and tumour-like lesions.
- Patients with suspected bone tumours should be referred to a bone sarcoma multidisciplinary team (MDT).
- There are two staging systems for bone tumours: TNM and Enneking systems.
- Medical management involves radiotherapy and/or chemotherapy.
- Surgical management involves surgical removal of tumour and stabilisation of pathological fractures.
- Complications include pathological fractures, metastasis and malignant transformation.
Reviewers
Mr Metin Tolga Buldu, BSc(Hons), MBChB, MRCS
Orthopaedic Registrar
Royal National Orthopaedic Hospital
Mr Jonathan R Perera, BSc (Hons), MBBS, MRCS, Dip Tr&Orth, FRCS Tr&Orth
Senior Sarcoma & Joint Reconstruction Fellow
Royal National Orthopaedic Hospital
Editor
Dr Chris Jefferies
References
- Office for National Statistics. Cancer registration statistics, England: 2017. Published in 2019. Available from: [LINK].
- Mescher, A. L. Junqueira’s Basic Histology Text & Atlas 15th ed. Published in 2018.
- World Health Organization. WHO Classification of Tumours, 4th Ed. Volume 3: Soft Tissue and Bone Tumours. Published in 2014.
- Azar, Beaty and Canale. Campbell’s Operative Orthopaedics 13th ed. Published in 2017.
- Leyla Noury. Structure of a long bone.
- Leyla Noury. Normal bone development.
- Hamblen and Simpson. Adams’s Outline of Orthopaedics 14th ed. Published in 2010.
- Solomon, Warwick and Nayagam. Apley and Solomon’s Concise System of Orthopaedics and Trauma 4th ed. Published in 2014.
- Davies, Pettersson, Ostensen et al. The WHO Manual of Diagnostic Imaging. Published in 2002.
- Leyla Noury. Common patterns of periosteal reaction.
- Gerrand et al., UK Guidelines for the Management of Bone Sarcomas, Published in 2016. Available from: [LINK]
- McLatchie, Borley, Chikwe. Oxford Handbook of Clinical Surgery 4th ed. Published in 2013.
- Cancer Research UK. Bone Cancer – Enneking staging system. Last reviewed in 2017. Available from: [LINK]
- National Institute for Health and Care Excellence. Improving outcomes for people with sarcoma. Last reviewed in 2014. Available from: [LINK]
- National Institute for Health and Care Excellence. Quality standard [QS78]. Published in 2015. Available from: [LINK]
- Xu et al. Denosumab and giant cell tumour of bone—a review and future management considerations. Published in 2013. Available from: [LINK]
- Thomas et al. Denosumab in patients with giant-cell tumour of bone: an open-label, phase 2 study. Published in 2010. Available from: [LINK]
- James Heilman, MD. Osteoma. License: [CC-BY-4.0]. Available from: [LINK]
- Osteoid osteoma in LT. X-ray and MRI demonstrating sclerosis and a nidus. License: [CC-BY-3.0]. Available from: [LINK]
- Amary et al. Ollier disease and Maffucci syndrome are caused by somatic mosaic mutations of IDH1 and IDH2. Published in 2011. Available from: [LINK]
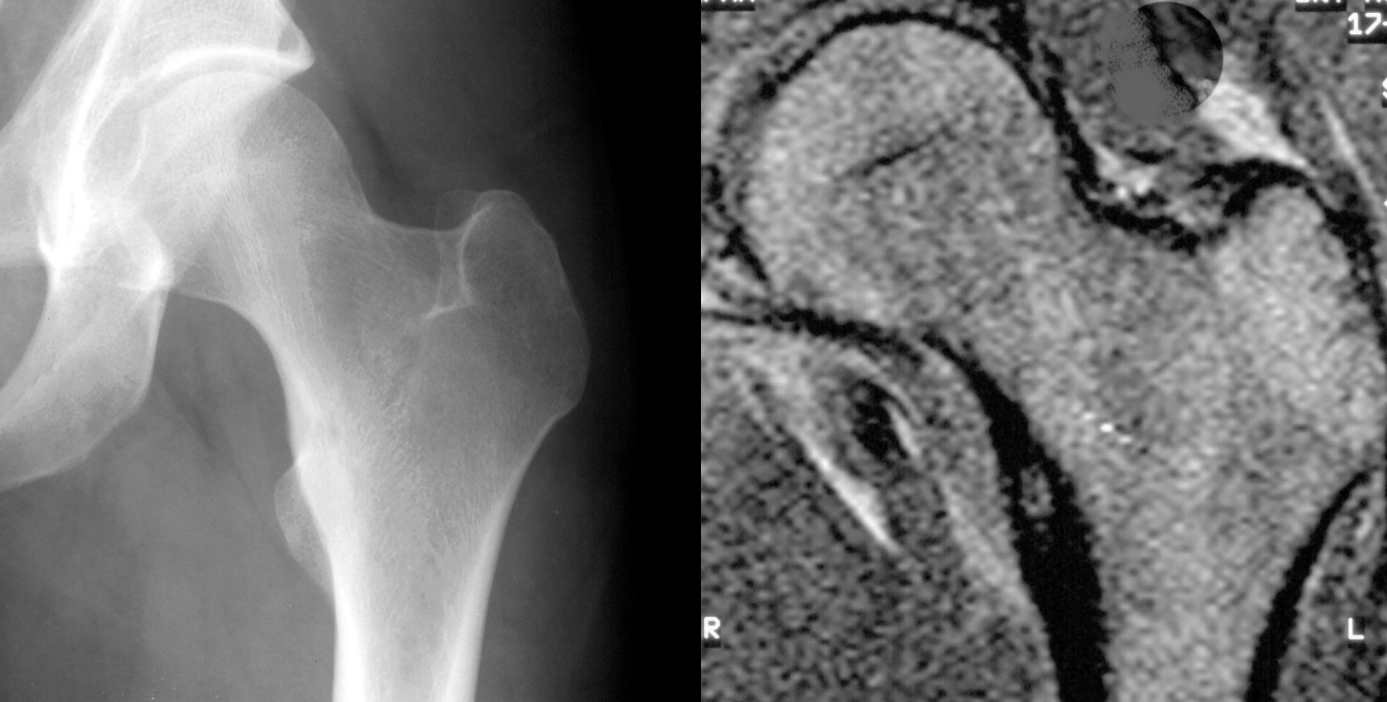
- Ruiz Santiago et al. Imaging of Hip Pain: From Radiography to Cross-Sectional Imaging Techniques. Synovial chondroma in hip. License: [CC-BY-4.0]. Available from: [LINK]
- Wellcome Collection gallery. Multiple Chondromata of fingers. License: [CC-BY-4.0]. Available from: [LINK]
- Bernard et al. Improved Differentiation of Benign Osteochondromas from Secondary Chondrosarcomas with Standardized Measurement of Cartilage Cap at CT and MR Imaging. Published in 2010. Available from: [LINK]
- Beltrami et al. Hereditary Multiple Exostoses: a review of clinical appearance and metabolic review. Published in 2016. Available from: [LINK]
- Michael R Carmont. Accelerated para-articular osteochondroma formation within the knee: a case report. Lateral radiograph of the knee demonstrating ossification in the peritendinous tissues in a patient with osteochondroma. License: [CC-BY-2.0]. Available from: [LINK]
- Campanacci et al. Giant-cell tumour of bone. Published in 1987. Available from: [LINK]
- James Heilman, MD. Giant cell bone tumor in the head of the 4th metacarpal of the left hand. License: [CC-BY-4.0]. Available from: [LINK]
- Henk Jan van der Woude ir Robin Smithuis (patobulino JustinasJa). Chondrosarcoma of the femur. License: [CC-BY-3.0]. Available from: [LINK]
- Yousef Samir. Osteosarkóm píštaly. License: [CC-BY-4.0]. Available from: [LINK]
- Toshifumi Ozaki. Diagnosis and treatment of Ewing sarcoma of the bone: a review article. Published in 2015. Available from: [LINK]
- Elzi et al. The role of FLI-1-EWS, a fusion gene reciprocal to EWS-FLI-1, in Ewing sarcoma. Published in 2015. Available from: [LINK]
- Michael Richardson, M.D. X-ray (lateral view) of an Ewing’s sarcoma (marked by white arrow) in the tibia of a child. License: [CC-BY-3.0]. Available from: [LINK]
- Robert A. Kyle and S. Vincent Rajkumar. Treatment of Multiple Myeloma: A Comprehensive Review. Published in 2009. Available from: [LINK]
- Mikael Häggström. X-ray of the left femur of a 59 year old man with elevated myeloma protein. It shows yet no signs of multiple myeloma. License: [CC-BY-1.0]. Available from: [LINK]
- Mikael Häggström. X-ray of the left femur of a 62 year old man with elevated myeloma protein. It shows typical lytic lesions of multiple myeloma. License: [CC-BY-1.0]. Available from: [LINK]
- Mikael Häggström. X-ray of the left humerus of a 59 year old man with elevated myeloma protein. It shows subtle lytic lesions of multiple myeloma. License: [CC-BY-1.0]. Available from: [LINK]
- Mikael Häggström. Description: X-ray of the left humerus of a 62 year old man with elevated myeloma protein. It shows typical lytic lesions of multiple myeloma. License: [CC-BY-1.0]. Available from: [LINK]
- James Heilman, MD. Sclerotic breast cancer metastasizes in the pelvis. License: [CC-BY-3.0]. Available from: [LINK]
- H. Liao, S. H. Lin, T. T. Wu. A 70-year-old male having advanced prostate cancer presenting with hypercalcemia and diffuse osteoblastic bone metastases: a case report. Abdominal radiograph showing osteoblastic changes of spine, pelvic and femoral bones (arrows). License: [CC-BY-2.0]. Available from: [LINK]
- Suat Çelik et al. Unicameral (simple) and aneurysmal bone cysts: the effect of insufficient curettage on recurrence. Radiography view of the simple bone cyst of the proximal humeral in 13-year-old boy. License: [CC-BY-2.0]. Available from: [LINK]
- Liu et al. Telangiectatic osteosarcoma: a review of literature. Published in 2013. Available from: [LINK]
- Park et al. Current management of aneurysmal bone cysts. Published in 2016. Available from: [LINK]
- Meryem Boubbou et al. Aneurysmal bone cyst primary – about eight pediatric cases: radiological aspects and review of the literature. License: [CC-BY-2.0]. Available from: [LINK]
- ESMO/European Sarcoma Network Working Group. Bone sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Published in 2014. Available from: [LINK]
