
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Down’s syndrome (DS), also known as trisomy 21, is the most common congenital chromosomal abnormality, occurring in about 1 in 800 to 1 in 1000 live births.1,2 The presence of additional genetic material from chromosome 21 results in characteristic phenotypic features and increased morbidity through its effect on multiple organ systems. The major cause of early mortality in Down’s syndrome is congenital heart disease.3,4 Despite this, many people with Down’s syndrome live happy and fulfilling lives, developing at their own pace and receiving coordinated care to manage comorbidities.
Aetiology
Trisomy 21 typically occurs via one of the following mechanisms:4,5
- Meiotic non-disjunction of the maternal chromosome 21 (95%)
- Robertsonian translocation of unbalanced chromosomal material, usually between chromosome 14 and chromosome 21 (4%)
- Mosaicism (1%)
Risk factors
Maternal age is the strongest risk factor for Down’s syndrome.23
Table 1. Risk of Down’s syndrome (live births) in relation to maternal age at delivery, prior to screening in pregnancy.4
|
Maternal age (years) |
Risk of Down’s syndrome |
|
All ages |
1 in 650 |
|
20 |
1 in 1530 |
|
30 |
1 in 900 |
|
35 |
1 in 385 |
|
37 |
1 in 240 |
|
40 |
1 in 110 |
|
45 |
1 in 37 |
Clinical features
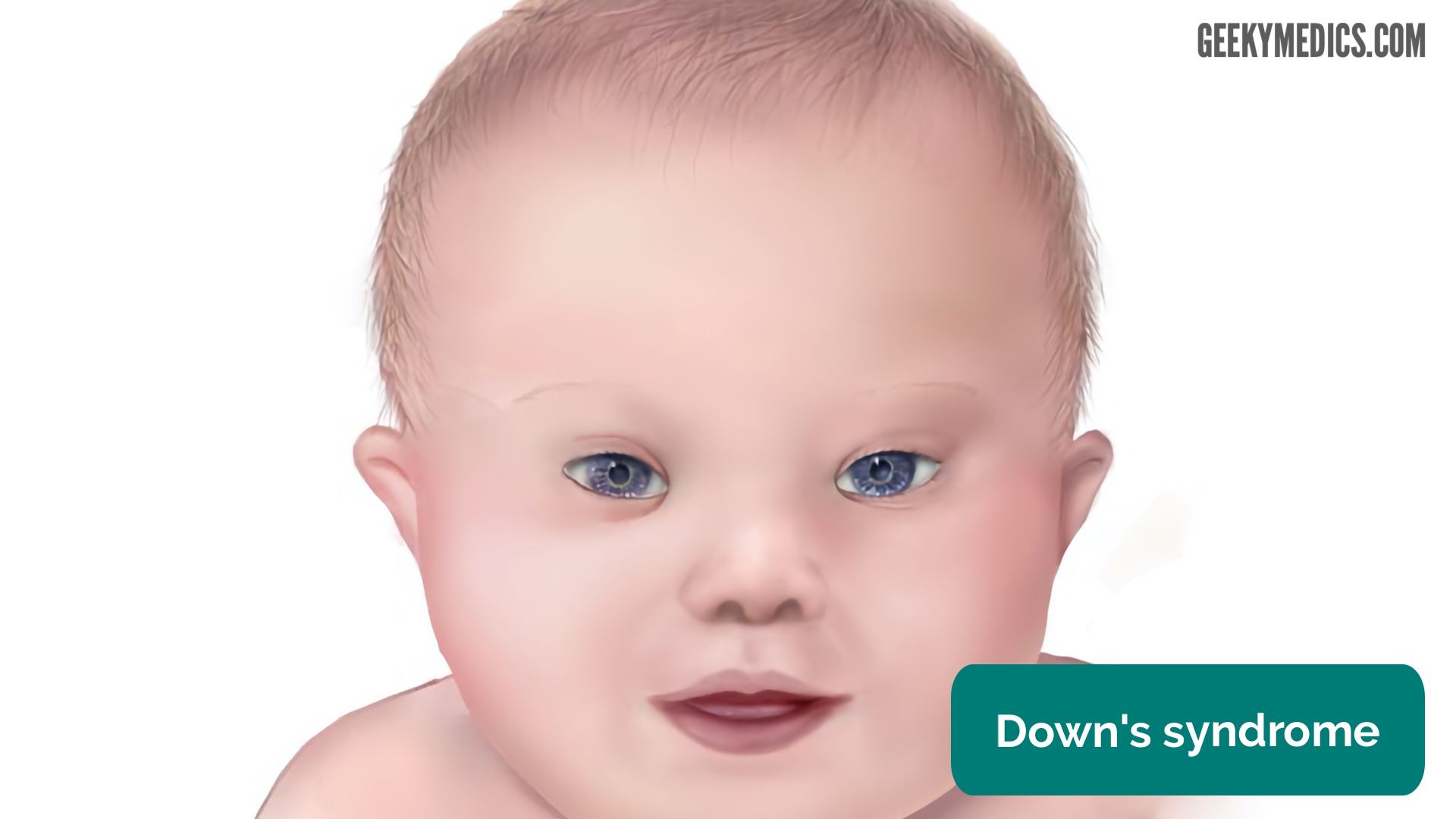
Dysmorphic features
Dysmorphic features which may be noted in neonates with Down’s syndrome are described below.2,7
General:
- Hypotonia: this may cause difficulties with feeding
- Hyperflexibility
Head:
- Oblique palpebral fissures
- Epicanthic folds
- Flat nasal bridge
- Brachycephaly (flat occiput)
- Dysplastic, low-set, small ears
- Open mouth with protruding or furrowed tongue
- High arched palate
Neck:
- Short neck with excessive skin at the nape of the neck
Hands:
- Transverse palmar crease (Simian crease)
- Short and incurved little finger
Feet:
- Large gap between the first and second toes (“sandal toe deformity”)
Congenital heart defects
Approximately 50% of neonates with DS will have associated congenital heart disease.
The most common forms of congenital heart disease are: 2-4,7,10
- Complete atrioventricular septal defect (37%)
- Ventricular septal defect (31%)
- Atrial septal defect (15%)
Neurological disease
Developmental delay and intellectual disability
Developmental milestones are frequently delayed in Down’s syndrome.
Intellectual disability is an almost universal feature of Down’s syndrome which can vary significantly in severity.
Autism, attention deficit hyperactivity disorder (ADHD) and aggressive behaviour are also more prevalent in Down’s syndrome.20
Alzheimer’s disease
Alzheimer’s disease develops in up to 75% of DS patients by the sixth decade of life.8,9,20.
Respiratory disease
Asthma and obstructive sleep apnoea are more common in Down’s syndrome.1
Gastrointestinal disease
Gastrointestinal tract anomalies requiring surgery occur in about 12% of patients with Down’s syndrome.1 The most characteristic anomaly is duodenal atresia caused by a failure of the intestine to recanalize during development.7,11 Other structural gastrointestinal anomalies may include imperforate anus and/or tracheo-oesophageal fistula.
Down’s syndrome is also associated with an increased risk of Hirschsprung disease.7
Endocrine disease
Endocrine diseases most commonly associated with Down’s syndrome include hypothyroidism and type 1 diabetes mellitus.
Haematological disease
Down’s syndrome is associated with an increased risk of developing several different haematological disorders including:1,7,14,15
- Immunodeficiency
- Transient myeloproliferative disorder
- Polycythaemia
- Acute megakaryoblastic leukaemia
- Acute lymphoblastic leukaemia
Other clinical features
Other clinical features associated with Down’s syndrome include (but are not limited to):
- Short stature and obesity
- Ophthalmological disorders including cataracts, refractive disorders, nystagmus, strabismus and glaucoma
- Orthopaedic disorders such as atlanto-axial instability, hyperflexibility, hip dislocation and foot deformities
- Recurrent acute otitis media 1
- Benign skin disorders such as hyperkeratosis and seborrhoeic dermatitis
- Urological abnormalities such as hypospadias and cryptorchism
- Juvenile idiopathic arthritis
Differential diagnosis
Differential diagnosis of Down’s syndrome includes, but is not limited to: 5,24
- Congenital hypothyroidism
- 49 XXXXY chromosome and high-order X chromosome disorders
- Zellweger syndrome (or other peroxisomal disorders)
- Aymé-Gripp syndrome
Investigations
Prenatal investigations
Screening for Down’s syndrome
Pre-natal screening is currently the most common means through which Down’s syndrome is identified and eventually diagnosed. Screening tests along with other data such as maternal age, weight, family origin and gestation are combined in software to calculate the probability of a fetus having Down’s syndrome. The screening test is considered positive if the risk of a fetus having Down’s syndrome is greater than 1 in 150. If the screening test returns a positive result, women are offered diagnostic testing.
Down’s syndrome screening most commonly involves:
- Serum screening: assessment of a range of biomarkers in the serum between 10-14 weeks + 1 day of gestation.
- Nuchal translucency scanning: ultrasound is used to assess the translucency of the nuchal pad at the nape of the fetal neck between 11 weeks + 2 days and 14 weeks + 1 day gestation. Increased nuchal translucency is associated with Down’s syndrome.
Serum screening and nuchal translucency scanning are typically used in combination (known as ‘the combined test‘).
The standard serum screen measures the following biomarkers:
- Beta-hCG: raised in Down’s syndrome
- PAPPA-A: decreased in Down’s syndrome
If a woman engages with antenatal care later in pregnancy when nuchal translucency scanning is less reliable, a different set of biomarkers are assessed (known as ‘the quadruple test‘):
- Beta-hCG: raised in Down’s syndrome
- AFP: low in Down’s syndrome
- Inhibin A: raised in Down’s syndrome
- Unconjugated estriol (uE3): low in Down’s syndrome
The quadruple test is less reliable than the combined test.
Non-invasive prenatal testing (NIPT)
During pregnancy, the placenta sheds cell-free DNA (cfDNA) into the mother’s bloodstream. As a result, the mother’s blood contains a mixture of placental and maternal cfDNA. By evaluating the cfDNA in the blood and combining this with the mother’s background chance of a trisomy (mother’s age or the combined test results), a likelihood ratio is obtained to predict whether or not the baby is more likely to have a chromosomal condition such as Down’s, Edward’s or Patau’s syndrome. It is possible from around 10 weeks gestation and has a sensitivity of around 99%.17-20
This test is not currently part of the routine screening pathway.
Confirming the diagnosis of Down’s syndrome
Karyotype analysis of fetal cells via chorionic villus sampling (9–12 weeks gestation) or amniocentesis (15–19 weeks gestation) is the gold standard for diagnosing Down’s syndrome, with equal detection rates of around 99%. There is a higher risk of pregnancy loss with chorionic villus sampling compared to amniocentesis.19
Post-natal investigations
Given the association of Down’s syndrome with a wide range of pathologies, it is essential that comprehensive screening is performed in the post-natal period to allow early identification and management of these complications.
Some examples of post-natal investigations include:
- Echocardiography: to screen for congenital cardiovascular abnormalities
- Red reflex testing: to screen for congenital cataracts
- TFTs: to screen for congenital thyroid disease
- FBC: to screen for myeloproliferative disorders and polycythaemia
- Hearing assessment: to screen for congenital hearing issues
- Radiographic swallowing assessment: performed if feeding difficulties are present to screen for gastrointestinal abnormalities (e.g. duodenal atresia)
Management
Management of Down’s syndrome requires a tailored multidisciplinary approach to screen, diagnose and treat complications. Patients with Down’s syndrome often require ongoing regular review from relevant specialists.
Genetic counselling
If a newborn is diagnosed with Down’s syndrome, parents should be referred for genetic counselling to discuss the risk of further children having Down’s syndrome.
Key points
- Down’s syndrome is caused by the presence of additional genetic material from chromosome 21.
- Clinical features of Down’s syndrome are wide-ranging including dysmorphic features, cognitive impairment and a multitude of other medical conditions.
- The biggest risk factor for Down’s syndrome is maternal age.
- Prenatal screening provides a method for assessing the risk of Down’s syndrome through the assessment of serum biomarkers and nuchal translucency.
- Prenatal diagnosis of Down’s syndrome can be achieved through chorionic villus sampling or amniocentesis.
- Post-natal screening investigations are essential to allow early identification of Down’s syndrome complications.
- Management of Down’s syndrome requires a tailored multidisciplinary approach to screen, diagnose and treat complications.
References
- Center for Disease Control. Data and statistics on Down syndrome. Reviewed December 5, 2019. Available from: [LINK]
- The University of Chicago Pediatrics Clerkship. Trisomy 21 (Down). 2013. Available from: [LINK]
- O’Learly, L et al. Early death and causes of death of people with Down syndrome: A systematic review. Published September 2018. Available from: [LINK]
- Illustrated textbook of pediatrics with STUDENT CONSULT online. Genetics. Published in 2015. Available from: [LINK]
- Orphanet. Down syndrome. Reviewed in September 2019. Available from: [LINK]
- Halliday, Jacquelyn V et al. Patient education: Should I have a screening test for Down syndrome during pregnancy? (Beyond the Basics). Reviewed in February 2020. Available from: [LINK]
- Kathryn K. Ostermaier. UpToDate.com. Down syndrome: Clinical features and diagnosis. Reviewed January 2020. Available from: [LINK]
- Alzheimer’s society. Down Syndrome and Alzheimer’s Disease. Available from: [LINK]
- Hill, DA et al. Mortality and cancer incidence among individuals with Down syndrome. March, 2003. Available from: [LINK]
- Freeman, SB et al. Population-based study of congenital heart defects in Down syndrome. Published in 1998. Available from: [LINK]
- Orphanet. Duodenal atresia. February 2009. Available from: [LINK]
- Celiac Disease Foundation. What is celiac disease? Available from: [LINK]
- Gillespie, Kath et al. The Down Syndrome Medical Interest Group. Down Syndrome Association: Health series. PDF. Reviewed in 2018. Available from: [LINK]
- Manivannan et al. Down Syndrome with Different Hematological Manifestations: A Short Series of 3 Cases with Review of Literature. March 2013. Available from: [LINK]
- Rabin, Karen and James A. Whitlock. Malignancy in Children with Trisomy 21. February 2009. Available from: [LINK]
- Lacy, Jordan et al. Atlantoaxial instability. January 2020. Available from: [LINK]
- Palomaki GE et al. A summary analysis of Down syndrome markers in the late first trimester. Published in 2007. Available from: [LINK]
- Alldred SK et al. Cochrane Database System Review. Second trimester serum tests for Down’s Syndrome screening. Published in 2012. Available from: [LINK]
- Hall, Justin and Azra Premji. Essential Med Notes 2015 Obstetrics. Page OB6. PDF. Published 2015.
- Bunt, Christopher W. Role of the Family Physician in the Care of Children with Down Syndrome. AAFP. December 15, 2014. Available from: [LINK]
- NHS. What is Down Syndrome? Reviewed in October 2019. Available from: [LINK]
- Benn, Peter. Advances in prenatal screening for Down syndrome: II first trimester testing, integrated testing, and future directions. 2002. Available from: [LINK]
- Stanford Children’s Health. Risks of Pregnancy Over Age 30. 2020. Available from: [LINK]
- Gratias Tom Mundakel. Down Syndrome Questions & Answers: Differential diagnosis. April 30, 2018. Available from: [LINK]
