

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Melanoma is a type of malignant cancer that arises from the melanocyte layer of the skin, normally situated in the basal layer of the epidermis.
Melanoma is the fifth most common cancer in the UK, with increasing incidence. It accounts for more cancer deaths than all other skin cancers combined.2
Aetiology
Melanoma occurs when melanocytic stem cells undergo a genetic transformation and proliferate uncontrollably.
Melanocytes produce melanin, a protein that helps protect against harmful ultraviolet (UV) radiation exposure. Melanocytes are found in equal numbers in different skin tones. However, darker skin produces more melanin. Therefore, damage caused by UV exposure is more likely in white skin compared to dark-brown or black skin.1
The growth of melanoma can be described as follows:
- In situ: the tumour is confined to the epidermis
- Invasive: the tumour has spread into the dermis
- Metastatic: the tumour has spread to other tissues
When melanocytes grow in a non-cancerous way, they result in moles (benign melanocytic naevi) and freckles (lentigines and phelides).1,3
Subtypes of melanoma
There are four common subtypes of melanoma (Table 1).
Table 1. Common subtypes of melanoma.1,3
| Subtype of melanoma | Description |
|
Superficial spreading melanoma  |
|
|
Nodular melanoma  |
|
|
Lentigo maligna melanoma  |
|
|
Acral lentiginous melanoma  |
|
Risk factors
Factors which increase the risk of melanoma include:2
- History of skin cancer, melanoma, or atypical naevi
- Family history of melanoma
- Pale skin (Fitzpatrick skin type I and II)
- Red or light-coloured hair
- High freckle density
- Light coloured eyes
- History of sunburn
- Sun exposure or tanning bed exposure
- Large amounts of moles
- Increasing age
- Immunosuppression
- Outdoor occupation
- Genetic syndromes with skin cancer predisposition (for example, xeroderma pigmentosum)
Clinical features
The first sign of melanoma is often a change in a previous mole, freckle or a new lesion arising in a normal patch of skin. Patients commonly present with a change in shape, size or colour (including the loss of pigmentation) of a lesion. However, melanomas can have no pigment (amelanotic melanoma), appearing as a pink or red lesion.4,5
Important areas to cover in the history of a pigmented lesion include:
- Location of the lesion on the body
- Date of onset of the lesion and duration
- Size of the lesion
- Changes in size, shape, and colour of the lesion
- Any bleeding and/or ulceration
- Risk factors
For more information, see the Geeky Medics guide to dermatological history taking.
ABCDE criteria
The ABCDE criteria are used to describe features that most melanomas have:1,5
- A: asymmetrical shape
- B: border irregularity, including poorly defined margins
- C: colour change and variation
- D: diameter of the mole (most melanomas are >6mm)
- E: evolving (such as changing in size, shape or colour)
For more information, see the Geeky Medics OSCE guide to examining a pigmented skin lesion.
Differential diagnoses
Differential diagnoses for a pigmented lesion include:3
- Benign naevus (mole)
- Lentigines
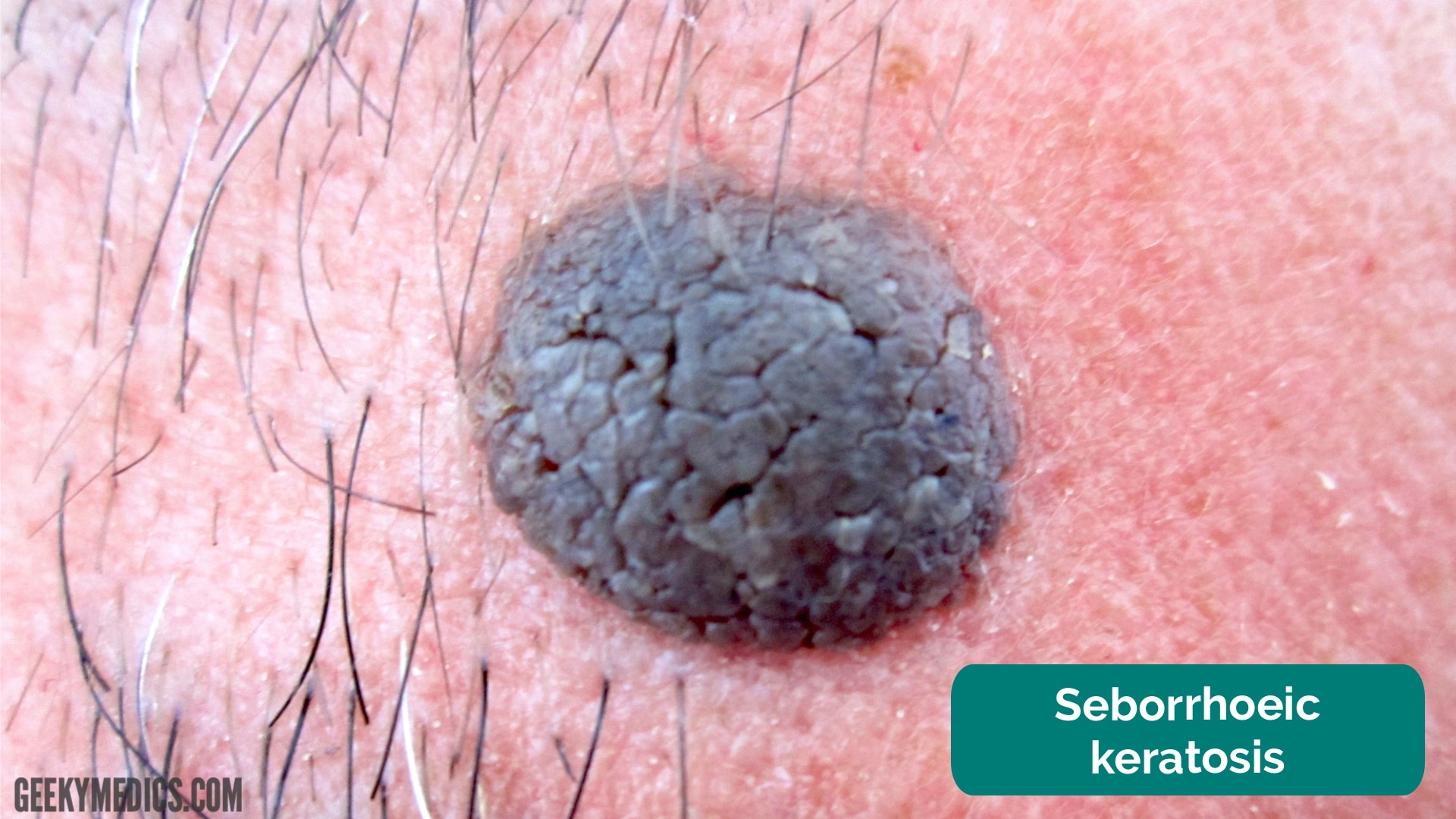
- Seborrhoeic keratoses
- Dermatofibroma
- Pigmented basal cell carcinoma (BCC)
Seborrhoeic keratoses
A common and benign class of lesion that can score highly on the ABCDE criteria are seborrhoeic keratoses (also called seborrhoeic warts).
Investigations
Melanoma is first inspected visually with the aid of a dermatoscope. Suspicious lesions are excised for histology with a lateral margin of 2-3 mm. The diagnosis is confirmed based on a full-thickness excisional skin biopsy.
Dermoscopy findings
The dermoscopic features of melanoma are highly variable and are assessed by trained physicians. In the early stages, melanoma may appear with organised features. However, as time progresses, features become more disorganised.
Due to their melanocytic origin, melanomas have the following features on dermoscopy:6
- Atypical network (white or pigmentated)
- Aggregated black or brown dots and globules
- Features specific to the site of the melanoma (e.g. parallel pattern on palms and soles)
Investigations for metastasis
In patients with advanced melanoma (stage IIb+), investigations should be considered to assess for metastasis in other sites of the body. Staging may be conducted with a whole-body and brain contrast-enhanced computed tomography (CT) scan. Staging with brain magnetic resonance imaging (MRI) may be considered in special circumstances.3,8
Management
All suspected melanomas should be referred urgently to a specialist. In the UK, an urgent referral means that you should see a specialist within 2 weeks.5
The management of melanoma depends on histological staging. Once a histological tissue sample is obtained, melanoma can be staged accordingly.
Table 2. The staging of melanoma.1
| Stage | Description |
| Stage 0 | ‘In situ’ melanoma |
| Stage 1 | Melanoma < 2 mm in thickness |
| Stage 2 | Melanoma > 2 mm in thickness, or > 1 mm in thickness with ulceration |
| Stage 3 | Melanoma spread to involve local lymph nodes |
| Stage 4 | Metastases to distant sites |
This is also known as the Breslow thickness, which measures the thickness of invasive melanoma in millimetres from the granular cell layer to the deepest tumour cell.1
Surgical management
The main management of melanoma is wide local excision. If the margins of the excised melanoma are inadequate, re-excision is performed.3,7
NICE guidelines recommend the following excision margins of tissue around the melanoma:
- Stage 0 melanoma (melanoma in situ): at least 0.5 cm
- Stage 1 melanoma: at least 1 cm
- Stage 2 melanoma: at least 2 cm
Sentinel lymph node biopsy
A sentinel lymph node biopsy is a procedure to test for the spread of cancer. It is generally indicated for melanoma with a Breslow thickness greater than 0.8 mm. It is often completed at the same time as surgical excision.8
The presence of metastatic disease in the sentinel lymph node mandates additional surgery to remove the remaining nodes, which is known as a lymph node dissection or completion lymphadenectomy.8
Medical management
Targeted therapy such as dabrafenib and vemurafenib may be used in patients with BRAF V600 mutation-positivity.
Immunotherapy such as nivolumab plus ipilimumab may be given to patients with stage IV or unresectable stage III melanoma if suitable.
Chemotherapy or the best supportive care may be considered for advanced melanoma not responsive to treatment.3,8
Complications
Melanoma has the greatest potential for metastasis causing local tissue invasion and destruction as compared with other skin malignancies.
Melanoma diagnosed at an advanced stage can cause serious morbidity and may be fatal despite treatment.3,8
The prognosis of melanoma is determined by the stage of the skin cancer, taking into consideration the Breslow thickness, spread to local lymphatics, and the level of ulceration.
The five-year survival for stage 1A melanoma (less than 1 mm thickness; no ulceration; mitoses less than 1 mm-2) is about 95%. In comparison, the five-year survival for stage 4 melanoma (spread to distant lymph nodes or other parts of the body) is 7-19%.3
Key points
- Malignant melanoma is a cancerous neoplasm of the pigment-forming cells called melanocytes.
- The rates of malignant melanoma are increasing, likely related to ultraviolet light exposure.
- All suspicious pigmented lesions should undergo excisional biopsy for histology.
- Management is dependent on the staging of melanoma. Surgical excision is the definitive treatment, with re-excision if needed.
Reviewer
Professor Nicola Ralph
Consultant Dermatologist
Editor
Dr Chris Jefferies
References
- Dermnet NZ. Melanoma. Published in October 2022. Available from: [LINK]
- The National Institute for Health and Care Excellence. Melanoma. Available from: [LINK]
- Patient Professional. Malignant Melanoma of the Skin. Published in August 2022. Available from: [LINK]
- British Association of Dermatologists. Melanoma Stage 2. Published in February 2019. Available from: [LINK]
- Cancer Research UK. Melanoma Skin Cancer. Published in March 2020. Available from: [LINK]
- Dermnet NZ. Dermoscopy of melanoma. Published in 2008. Available from: [LINK]
- British Association of Dermatologists. Dermatology – A handbook for medical students and junior doctors. Published in November 2020. Available from: [LINK]
- The National Institute for Health and Care Excellence. Melanoma: assessment and management. Published in July 2015. Available from: [LINK]
Image references
- Figure 1. DermNet NZ. Superficial spreading melanoma dermoscopy. Licence: [CC BY-SA]
- Figure 2. DermNet NZ. Nodular melanoma. Licence: [CC BY-NC-ND]
- Figure 3. DermNet NZ. Lentigo Maligna. Licence: [CC BY-NC-ND]
- Figure 4. DermNet NZ. Acral lentiginous melanoma. Licence: [CC BY-NC-ND]
- Figure 5: Делфина. Adapted by Geeky Medics. Seborrhoeic keratosis. Licence: [CC BY-SA]
