
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Optic neuritis (ON) is an inflammatory optic neuropathy usually affecting one eye at a time and typically presents with acute or subacute visual loss. It frequently occurs in association with multiple sclerosis (MS).
Aetiology
Typical (demyelinating) ON is strongly associated with MS. It may initially occur as a clinically isolated syndrome without evidence of generalised demyelination, however, this eventually develops in a significant proportion of patients.
Other less common (atypical) causes of ON include:1
- Antibody-mediated: neuromyelitis optica spectrum disorders (NMOSD) and myelin oligodendrocyte glycoprotein antibody disease (MOGAD)
- Non-infectious: neurosarcoidosis and systemic autoimmune conditions such as systemic lupus erythematosus
- Infectious: syphilis, Lyme disease, cat-scratch disease, herpes zoster, sinus disease
- Post-infectious: following an acute infection or immunisation
Pathophysiology
As in MS, the primary mechanism is autoimmune. T-cells are directed against the central nervous system myelin antigens which destroy the myelin sheath.
Other significant contributing factors include a precipitating infectious agent (Epstein-Barr virus), genetic susceptibility and the environment (low vitamin D, low UV exposure, smoking and obesity).2
Risk factors
Risk factors for ON include:2,3,4
- Known diagnosis of MS: up to 70% of patients with MS will have at least one episode. Optic neuritis can be the presenting feature of MS in up to 20% of cases.
- Female sex: there is a female predominance by a ratio of 3:1
- Young age: most patients are aged 20-50 years
- Higher latitude: the incidence is higher for populations at higher or lower latitudes (the northern United States, northern and western Europe, southern Australia and New Zealand) compared with areas closer to the equator
Clinical features
History
Typical symptoms of demyelinating ON include:5,6,7
- Acute to subacute unilateral loss of vision: the visual acuity upon testing can vary from being normal (6/6) to rarely becoming ‘no perception of light’, i.e. inability to tell when a bright flashlight is being shone into the affected eye.
- Retrobulbar and peri-ocular pain: this is present in >90% of cases and is exacerbated by eye movements and may precede or occur with visual loss. The pain is believed to occur due to close proximity of rectus muscle insertions to the inflamed optic nerve sheath at the orbital apex.
- Photopsias (flashes) exacerbated by eye movements
- Visual field loss: any pattern of field loss may be seen including diffuse, altitudinal, central and sectoral losses.
- Reduced contrast sensitivity and colour vision.
The vision worsens over hours to days, but recovery starts within two weeks with or without treatment. The visual acuity may recover to near normal but permanent abnormalities of colour perception, contrast sensitivity and visual field may occur.
Clinical examination
All patients with suspected optic neuritis should undergo a comprehensive ophthalmic, cranial nerve and neurological examination.
The ophthalmic examination should include:4
- Visual acuity testing with a Snellen chart
- Colour vision assessment with an Ishihara test
- Testing for a relative afferent pupillary defect (RAPD): this will be positive for the affected eye unless there is pre-existing disease in the contralateral eye.
- Fundoscopy: swelling of the optic nerve may be visible in a third of patients and is typically mild. However, most patients have retrobulbar involvement therefore the optic nerve appears normal. Over time, the optic nerve will develop pallor.
- Testing extraocular muscle movements: expected to be normal in ON but may detect internuclear ophthalmoplegia (common in multiple sclerosis)
For more information on clinical examination findings, see the Geeky Medics guide to multiple sclerosis.
Differential diagnoses
Alternative diagnoses should be considered in patients with atypical features.6
Differential diagnoses for unilateral acute and chronic optic neuropathies are wide-ranging and include:1
- Atypical causes of ON (see aetiology section)
- Ischaemic: giant cell arteritis must be considered in a patient over the age of 50
- Hereditary: Leber’s hereditary optic neuropathy
- Compressive/infiltrative: secondary to an orbital infection, malignancy or inflammatory disease (e.g. sarcoidosis).
- Nutritional/toxic: B12/folate deficiency and alcohol
- Trauma/radiation
Investigations
Optic neuritis is a clinical diagnosis in patients with typical features of demyelinating ON.
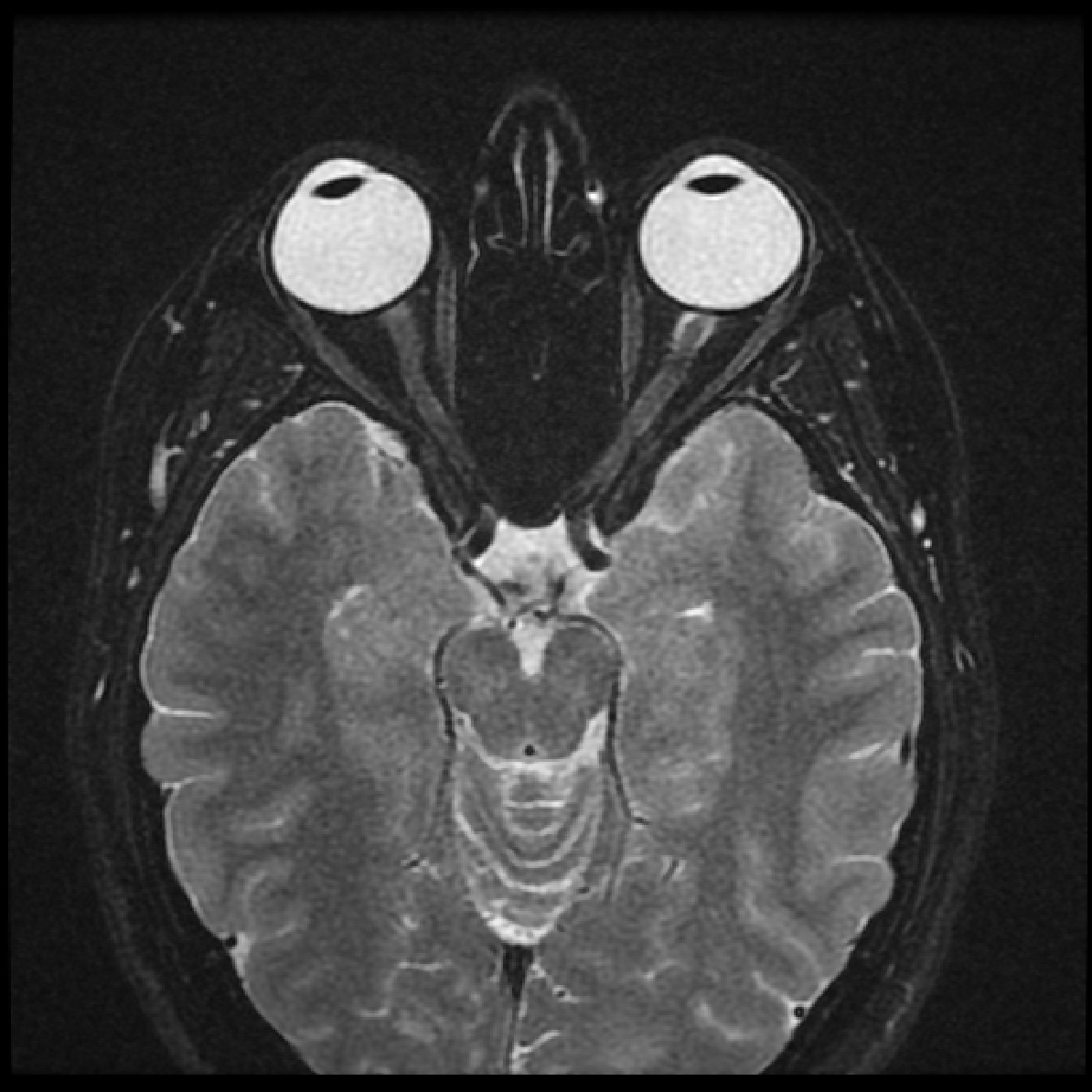
An MRI of the brain and orbits with gadolinium contrast will show enhancement of the optic nerve, confirming the diagnosis. MRI may also identify any white matter lesions suggestive of MS (Figure 1).
A lumbar puncture for CSF analysis may be useful to support the diagnosis of MS if the MRI is normal.
Patients with atypical features may require additional laboratory and radiological investigations depending on the clinical context to exclude other causes of optic neuropathy.
Management
Optic neuritis treatment trial (ONTT)6
The Optic Neuritis Treatment Trial (ONTT) was a landmark study which demonstrated an increased rate of visual recovery in typical ON patients treated with high-dose systemic (intravenous) steroids.
However, the final visual outcome at 6 months was similar to the placebo group. Oral prednisolone was found to be ineffective and increased the risk of recurrence of ON. The trial also found that intravenous methylprednisolone reduced the risk of developing MS in patients with typical ON for the first 2-years compared to placebo.
Medical management
Patients with typical ON should be started on high-dose corticosteroid therapy.
The typical regimen is intravenous methylprednisolone 1g daily for three days followed by an oral prednisolone taper (1mg/kg for 11 days).
Oral methylprednisolone 500mg once a day for five days has been suggested as an alternative to intravenous steroids, but its use remains controversial.
The decision to treat may depend on several factors. Treatment is more likely to be offered to those with a diagnosis of MS, profound visual loss in a solitary eye, or in cases of severe pain.3 It is important to consider the significant side effects which can be associated with high-dose steroids, and counsel the patient appropriately.
Trials have shown that both interferon-beta and glatiramer acetate prolong the time to development of clinically definite MS in patients with ON and at least two white matter lesions on MRI.3,8
Complications
Patients with ON have favourable outcomes with >90% recovering vision to 6/12 or better within one year and this was sustained at 15 years of follow-up in the ONTT.9
However other abnormalities such as contrast sensitivity, relative afferent pupil defect and abnormalities of colour perception may persist.
The risk of recurrence in the affected or contralateral eye is about 30% at 5 years.10
An episode of ON does not imply a definite conversion to MS. Data from the ONTT shows that the overall 15-year risk of developing MS is 50%. The risk is 25% for patients with a normal MRI and up to 72% for those with one or more lesions on MRI.11
Key points
- Optic neuritis is an acute optic neuropathy that typically presents in a patient aged 20-50 with unilateral loss of vision over hours to days, with recovery starting within two weeks.
- The typical clinical signs elicited on examination are decreased visual acuity, decreased colour vision, relative afferent pupillary defect, and retrobulbar pain that is worse on eye movement.
- An episode of optic neuritis may occur in isolation or may be associated with demyelinating (multiple sclerosis being the most common association) or other inflammatory aetiologies.
- Diagnosis can be made on clinical grounds but radiological and laboratory investigations may be needed particularly to rule out other, non-MS causes.
- An acute episode may be treated with a short course of high-dose systemic corticosteroids.
- Most patients with typical optic neuritis recover to near normal vision.
- The risk of developing multiple sclerosis at 15 years following an episode of optic neuritis is about 50%.
Editor
Dr Chris Jefferies
References
- Kanski JJ, Bowling B. Clinical Ophthalmology: A Systematic Approach. Edinburgh, Elsevier/Saunders; 2015.
- Baecher-Allan C, Kaskow BJ, Weiner HL. Multiple Sclerosis: Mechanisms and Immunotherapy. Neuron. 2018;97(4):742–68.
- Pau D, al Zubidi N, Yalamanchili S, Plant GT, Lee AG. Optic neuritis. Eye. 2011;25(7):833–42.
- Denniston A, Murray P. Oxford Handbook of Ophthalmology. 4th ed. OUP Oxford; 2018.
- Keltner JL, Johnson CA, Cello KE, Dontchev M, Gal RL, Beck RW. Visual field profile of optic neuritis: A final follow-up report from the optic neuritis treatment trial from baseline through 15 years. Archives of Ophthalmology 2010;128(3):330–7.
- Beck RW, Cleary PA, Anderson MM, et al. A Randomized, Controlled Trial of Corticosteroids in the Treatment of Acute Optic Neuritis. New England Journal of Medicine [Internet] 1992;326(9):581–8. Available from: [LINK]
- The Optic Neuritis Study Group. The Clinical Profile of Optic Neuritis: Experience of the Optic Neuritis Treatment Trial. Archives of Ophthalmology [Internet] 1991;109(12):1673–8. Available from: [LINK]
- Comi G, Martinelli V, Rodegher M, et al. Effect of glatiramer acetate on conversion to clinically definite multiple sclerosis in patients with clinically isolated syndrome (PreCISe study): a randomised, double-blind, placebo-controlled trial. The Lancet [Internet] 2009;374(9700):1503–11. Available from: [LINK]
- The Optic Neuritis Study Group. Visual Function 15 Years after Optic Neuritis: A Final Follow-up Report from the Optic Neuritis Treatment Trial. Ophthalmology [Internet] 2008;115(6):1079-1082.e5. Available from: [LINK]
- The Optic Neuritis Study Group. Visual Function 5 Years After Optic Neuritis: Experience of the Optic Neuritis Treatment Trial. Archives of Ophthalmology [Internet] 1997;115(12):1545–52. Available from: [LINK]
- The Optic Neuritis Study Group. Multiple Sclerosis Risk After Optic Neuritis: Final Optic Neuritis Treatment Trial Follow-up. Archives of Neurology [Internet] 2008;65(6):727–32. Available from: [LINK]
Image references
- Figure 1. Dr Mohammad A. ElBeialy / Radiopaedia.org. From the case rID: 38584. License: [CC BY-NC-SA]
