
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Pericarditis refers to inflammation of the pericardium, a fibrous sac surrounding the heart.
Pericarditis is more prevalent in men, predominantly in young adults. It is the most common disease of the pericardium seen in clinical practice. Pericarditis makes up 0.1% of all hospital admissions and 5% of emergency department admissions for chest pain.
Acute pericarditis has several potential causes, although in most cases it is idiopathic.1
Aetiology
Anatomy
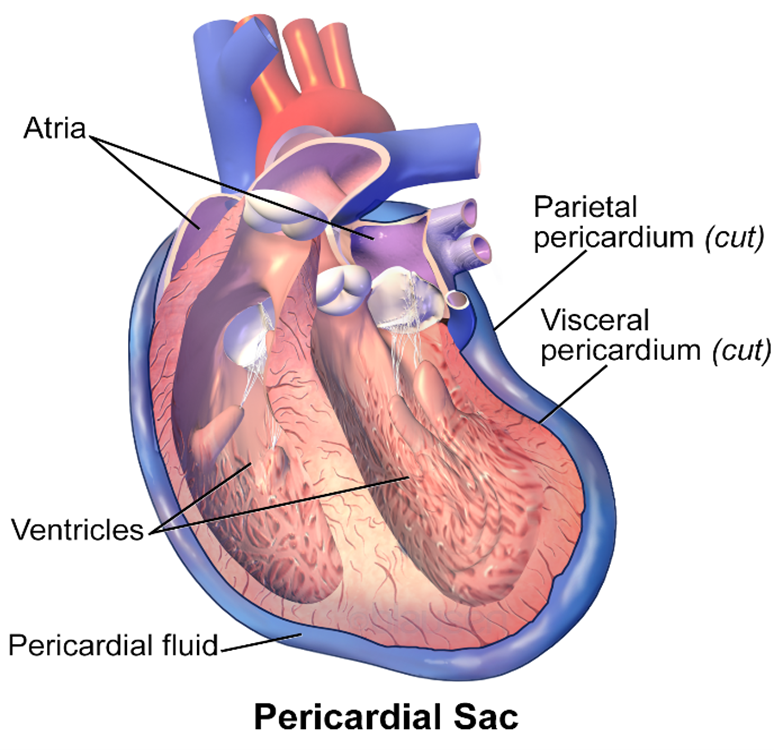
The pericardium is the outer lining of the heart and comprises of two parts, an outer fibrous pericardium and inner serous pericardium.2
The fibrous pericardium surrounds the heart with tough connective tissue but remains unattached to the heart itself.2
The serous pericardium consists of an outer parietal layer, which sticks to the inner surface of the fibrous pericardium, and an inner visceral layer that attaches to the heart and forms the heart’s outer epicardium layer.3
A small space exists between the parietal and visceral layers of the serous pericardium, called the pericardial cavity, where a small volume of fluid separates the heart from its surroundings, reducing friction and enabling a degree of freedom in heart movement and changes in shape.3
Causes of pericarditis
Most cases of pericarditis are idiopathic, and an underlying cause is not found.
However, potential underlying causes of pericarditis include:4
- Infections: viruses (e.g. coxsackievirus and HIV), bacteria (e.g. staphylococcus and Mycobacterium tuberculosis) and fungi (e.g. histoplasmosis)
- Acute myocardial infarction: pericarditis occurs 1-3 days after an infarction involving the full thickness of the ventricular wall (transmural). This is believed to be the result of the healing necrotic heart tissue interacting with the pericardium.
- Dressler’s syndrome: this form of pericarditis tends to occur weeks to months after myocardial infarction. It is an autoimmune response triggering systemic inflammation, affecting other serous membranes as well such as the pleura.
- Cancer: primary tumours (e.g. mesotheliomas) or metastatic (e.g. from breast or lung cancers)
- Autoimmune: collagen or vascular disorders (e.g. rheumatoid arthritis, systemic lupus erythematosus)
- Drug-induced (e.g. hydralazine)
- Uraemic: from the accumulation of toxic metabolites and nitrogenous waste in the blood as seen with end-stage renal disease
Risk factors
Risk factors for pericarditis include:5
- Age: the average age of patients with acute pericarditis is 41-60 years and advanced age is a risk factor for bacterial pericarditis
- Sex: males have a higher risk for developing acute pericarditis
- Seasons: idiopathic pericarditis has been found to occur most often in the spring and fall
- Steroids: recurrent pericarditis occurs more often in patients being treated with steroids
Additional risk factors for bacterial pericarditis include:5
- Diabetes
- Extensive burn injuries
- Systemic infections
- Immunosuppression
- Heart surgery
- Chest trauma
- Pre-existing pericardial effusion
Clinical features
History
Typical symptoms of pericarditis include:4
- Chest pain (>90%): typically retrosternal but can be left-sided, radiating to the neck, shoulders and arms. Radiation to the trapezius ridge is a classic sign. It can be exacerbated by deep inspiration (pleuritic) and when lying down, typically relieved by sitting or leaning forwards.
- Dyspnoea
Other important areas to cover in the history include:4
- Systems review: can identify clues related to the causative diagnoses such as recent infective symptoms or a known autoimmune disorder
- Drug history (e.g. chemotherapy drugs)
- Travel history: may reveal recent travel to countries endemic for certain infectious diseases
Clinical examination
A thorough cardiovascular examination should be performed to look for features of pericardial effusion and cardiac tamponade.
Typical clinical findings in pericarditis include:4
- Pericardial rub: due to friction between the pericardial layers, typically loudest at the left lower sternal border, best heard with the patient leaning forward
- Evidence of pericardial effusion: usually not symptomatic unless large, may hear soft/distant heart sounds, tubular breath sounds in the left axilla/base due to bronchial compression, obscured apex beat
- Beck’s triad indicative of cardiac tamponade: hypotension, muffled heart sounds and a raised JVP
Cardiac tamponade
Patients with cardiac tamponade exhibit varying signs of decreased cardiac output and shock including hypotension, tachycardia, tachypnoea, cool peripheries, diaphoresis and peripheral cyanosis.
The y descent of the JVP is usually absent, as the heart volume becomes fixed and venous inflow can’t increase
Pulsus paradoxus may be present. This refers to an abnormally large drop in pulse pressure during inspiration (≥10mmHg in systolic pressure).
Differential diagnoses
It is important to differentiate acute pericarditis from other causes of chest pain such as acute coronary syndrome, pneumonia with pleurisy, pulmonary embolism, gastro-oesophageal reflux disease and costochondritis.
A detailed history is important to make this distinction as well as a thorough systems review. Investigations such as ECGs and chest X-rays are also important for the exclusion of other differential diagnoses.
Other less common differentials include:
- Aortic dissection
- Intra-abdominal pathology
- Pneumothorax
Cardiac tamponade can be confused with conditions that cause shock, low blood pressure, raised JVP, including:6
- Decompensated heart failure
- Conditions causing pulmonary hypertension such as pulmonary embolism, chronic lung disease, coronary artery disease, liver cirrhosis
- Right ventricular myocardial infarction
Investigations
Bedside investigations
Relevant bedside investigations include:2
- Basic observations (vital signs): to check for signs of shock such as hypotension and tachycardia
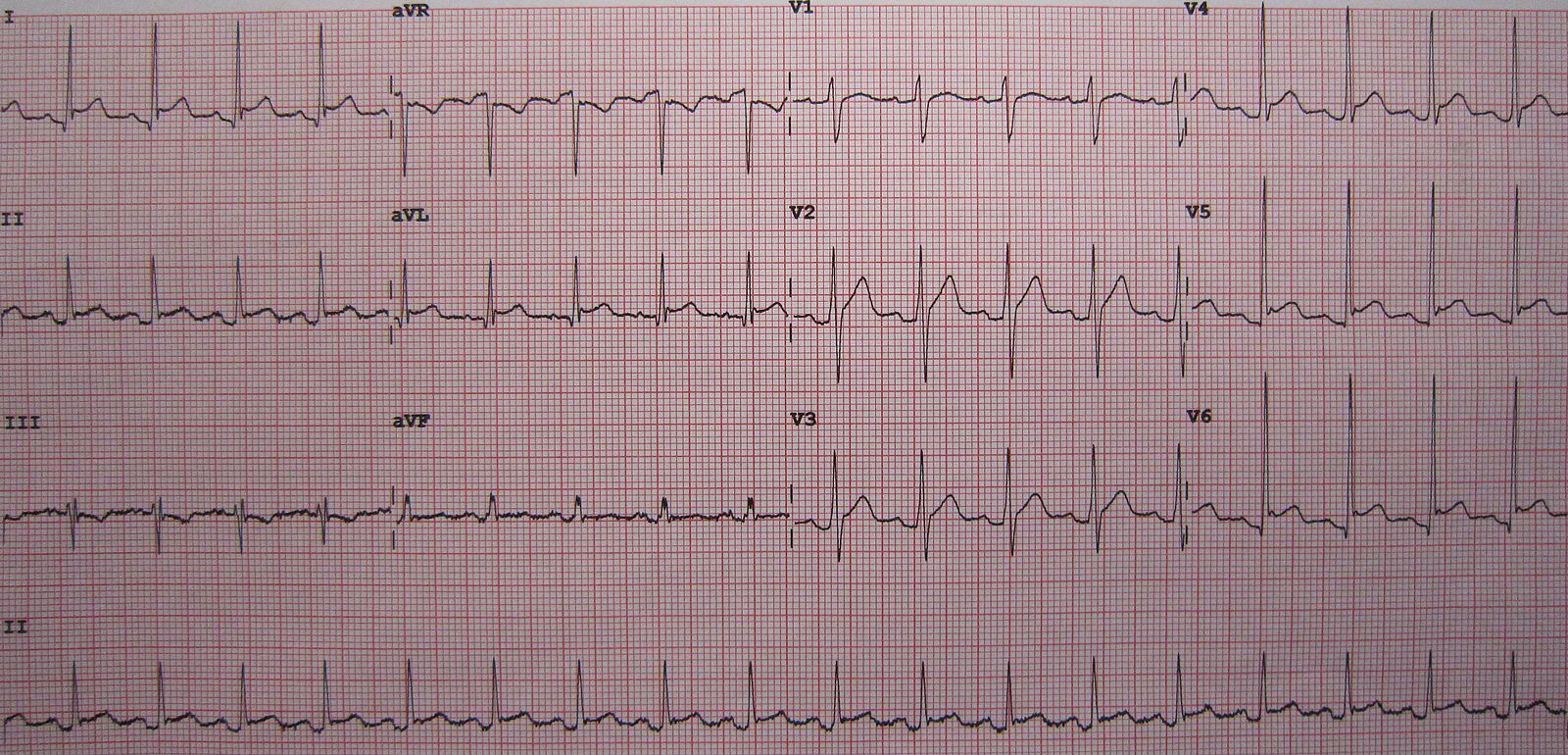
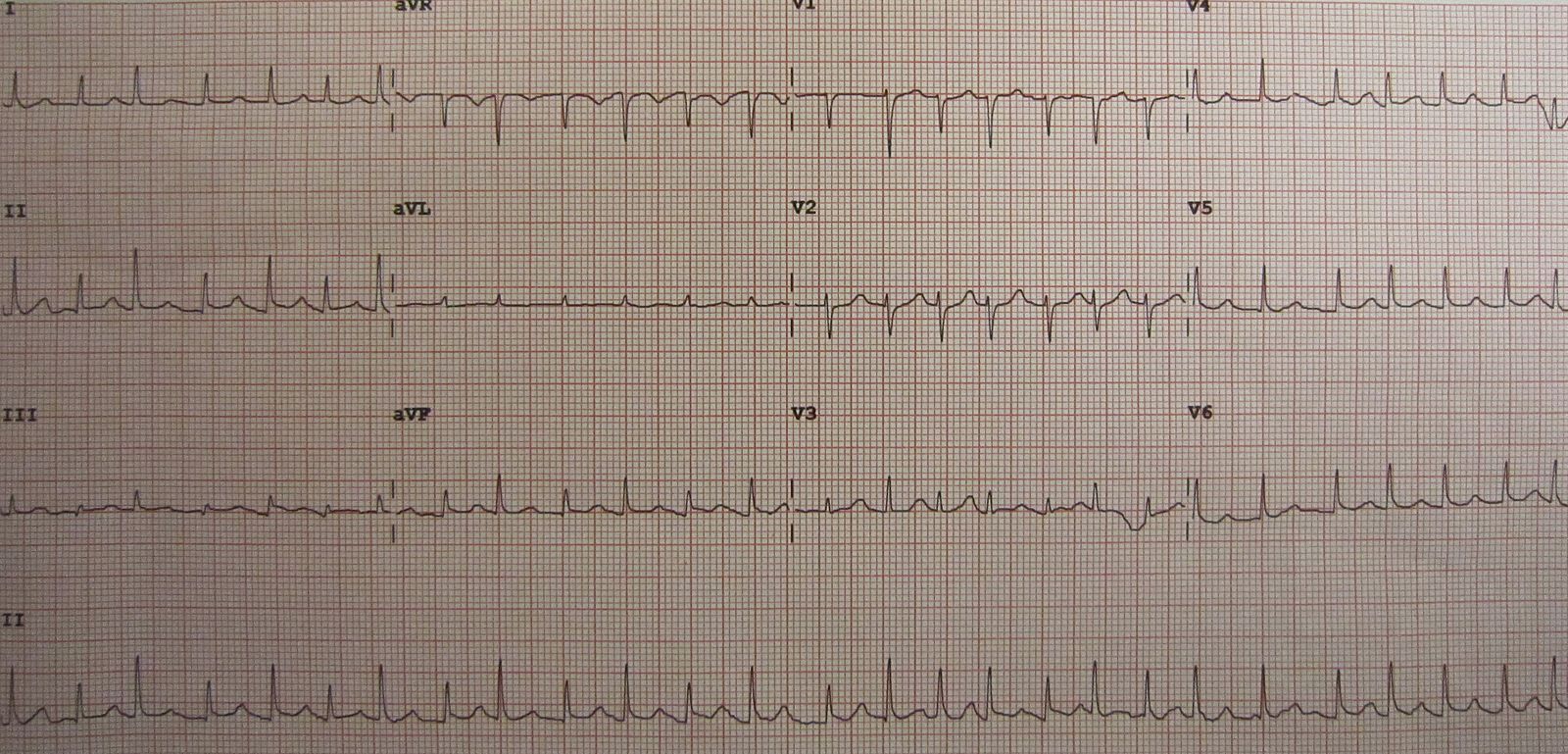
- 12-lead ECG: typical findings are widespread ‘concave/saddle shaped’ ST-elevation except in aVR and often V1, PR segment depression; low voltage QRS complexes/‘electrical alternans’ indicates significant pericardial effusion. These ECG changes reflect myocardial involvement as the pericardium is electrically inert.
Laboratory investigations
There is no single diagnostic laboratory test for acute pericarditis. However, blood tests can help exclude other causes or may give clues to the underlying aetiology or potential precipitating factors.
Relevant laboratory investigations include:1
- Full blood count: raised white blood cell count is a common finding
- Inflammatory markers: a raised CRP/ESR is a common finding
- Troponin: may be elevated if there is co-existent myocarditis
- Urea and electrolytes: for renal dysfunction
- Liver function tests: for liver dysfunction
Additional testing would be done if suspecting a specific cause, for example measuring anti-nuclear antibody in a young woman if there is suspicion of systemic lupus erythematosus.
Imaging
Relevant imaging investigations include:1
- Chest X-ray: often normal in acute pericarditis, a raised cardiothoracic ratio is typically associated with a pericardial effusion of over 300mls and there may be a globular appearance to the cardiac silhouette (Figure 4).
- Transthoracic echocardiography: performed to check for any evidence of effusion. If there is an effusion, it is important to look for any signs of haemodynamic compromise as it the haemodynamic effects of the effusion rather than the size of the effusion which predicts if the patient may need the effusion draining and decisions on whether they need to stay in as an inpatient or if they can be managed as an outpatient.
- Cardiac CT or MRI: may be performed in atypical presentations to look for pericardial thickening and inflammation. An MRI may be performed in suspected myopericarditis as these patients have poorer long-term outcomes and require additional drug treatment including ACE inhibitors or beta-blockers as well as follow up.

Management
After confirming the diagnosis, assessing for an underlying cause, and looking for evidence of pericardial effusion, treatment is usually directed at alleviation of symptoms as acute idiopathic pericarditis is typically self-limiting in 70-90% of patients.
If an underlying cause of pericarditis is found, management should involve treating the underlying condition.
General lifestyle advice for all patients includes restricting physical activity until symptoms have resolved and, for athletes, it is recommended to return to sports after three months, only after symptoms have fully resolved and investigation findings have normalised. As with all presentations, safety netting for symptoms of deterioration is important.
Symptomatic management
Non-steroidal anti-inflammatories such as ibuprofen are first-line for symptomatic treatment. The choice of drug is based on the patient’s history (e.g allergies, contra-indications or co-morbidities). For example, aspirin would be favoured if it is already needed for antiplatelet treatment and patient preferences. Gastroprotection with a proton pump inhibitor should be given as well.
Colchicine is recommended as an adjunct for three months. It has been shown to improve the response to medical therapy and reduce recurrences by approximately 50% during follow-up.
Corticosteroids are second-line, for example, if there is a contraindication to or failure of NSAID and colchicine therapy. Low doses are recommended to prevent complications and colchicine is given concurrently.
Predictors of poor prognosis
Major risk factors identified suggestive of a poor prognosis include:1
- Fever >38oC
- Subacute onset
- Large pericardial effusion
- Cardiac tamponade
- Failure of response to NSAIDs after a week of therapy
Complications
Pericardial effusion & cardiac tamponade
Any disease leading to pericarditis can cause pericardial effusion, its formation is a response to inflammation, infection or neoplastic conditions involving the pericardium (exudate). Pericardial fluid can also accumulate due to reduced reabsorption because of a rise in systemic venous pressure from heart failure or pulmonary hypertension (transudate).1
As an effusion accumulates, pericardial pressure builds up and impedes right heart filling, leading to underfilling of the left heart. It reaches a critical point when the effusion decreases the diastolic volume of the heart chambers, leading to reduced cardiac output. This compromise of ventricular filling leading to haemodynamic compromise is termed cardiac tamponade, a life-threatening emergency.5
Treatment involves draining the pericardial fluid typically by pericardiocentesis using echo/fluoroscopic guidance. The pericardial fluid can be sent off for analysis for diagnostic purposes.4
Recurrent or chronic pericarditis
Approximately 15-30% of patients develop a recurrence of symptoms. This can be termed ‘incessant’ with symptoms lasting for more than 4-6 weeks or ‘chronic’, lasting for more than 3 months. This rate of recurrence may rise to 50% in patients not given colchicine, especially if treated with steroids.1
Novel treatment options now exist for refractory recurrent pericarditis, including immunosuppressants (such as azathioprine), intravenous immunoglobulins and IL-1 antagonists (such as anakinra).1
A potential alternative to giving further medical treatment is pericardiectomy (surgically removing part or all of the pericardium).1
Constrictive pericarditis
This can be considered the final stage of the inflammation involving the pericardium. The risk of progression is particularly linked to the aetiology with the risk being highest in bacterial pericarditis. The most prevalent cause reported in developed countries is idiopathic, viral, post-cardiac surgery or post-radiation.1
Inflammation in the pericardium can result in fibrosis and calcification, with adhesions of the parietal and visceral pericardium. This scarring tends to be symmetric and if the pericardium becomes inelastic to a point where it hinders diastolic filling of the cardiac chambers, this is termed constrictive pericarditis. These represent chronic changes, therefore it enables to body to compensate and is therefore not imminently life-threatening like cardiac tamponade.5
For the majority of patients, the definitive treatment for chronic constrictive pericarditis is surgical pericardiectomy (resection of the pericardium).2
Key points
- The pericardium is the outer lining of the heart, consisting of an outer fibrous pericardium and inner serous pericardium.
- Acute pericarditis is the term given to inflammation of the pericardium. Most cases are idiopathic.
- Typical symptoms include central or left-sided chest pain, typically pleuritic in nature and relieved by leaning forwards.
- Clinical examination is often normal, however, a pericardial rub may be heard on auscultation.
- Signs of complications may be detected on clinical examination such as hypotension, muffled heart sounds and a raised JVP suggesting cardiac tamponade.
- Important investigations include 12-lead ECG, chest x-ray and echocardiography.
- Initial management is focused on confirming the diagnosis and looking for an underlying aetiology if clinical findings are suggestive of one.
- Idiopathic pericarditis is typically self-limiting therefore treatment is focused on alleviating symptoms.
- First-line treatment is an NSAID with colchicine given as an adjunct for three months.
- Complications include pericardial effusion and cardiac tamponade, recurrent symptoms and constrictive pericarditis.
Reviewer
Dr Kuldeepa Veeratterapillay
Cardiology Registrar
Editor
Dr Chris Jefferies
References
- Yehuda Adler, Philippe Charron, Massimo Imazio, Luigi Badano, Gonzalo Barón-Esquivias, Jan Bogaert, Antonio Brucato, Pascal Gueret, Karin Klingel, Christos Lionis, Bernhard Maisch, Bongani Mayosi, Alain Pavie, Arsen D Ristić, Manel Sabaté Tenas, Petar Seferovic, Karl Swedberg, Witold Tomkowski, ESC Scientific Document Group, 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC). Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS), European Heart Journal, Volume 36, Issue 42, 7 November 2015, Pages 2921–2964
- Susan Standring. Gray’s Anatomy. 42nd Elsevier. Published in 2020.
- Amar Vaswani, Hwan Juet Khaw, Scott Dougherty, Vipin Zamwar, Chim Lang. Cardiology in a heartbeat. Scion Publishng Limited. Published in 2016.
- Parveen J. Kumar, Michael L. Clark, Adam Feather, David Randall, Mona Waterhouse. Kumar and Clark’s Clinical Medicine. Tenth Edition. Elsevier. Published in 2020.
- Hessen et al. Elsevier Point of Care. Clinical overview. [Updated 2021 Jul 20].
- Douglas P. Zipes, Peter Libby, Robert O. Bonow, Douglas L. Mann, Gordon F. Tomaselli, Eugene Braunwald. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine, Eleventh Edition. Published in 2018.
Images
- Figure 1. Blausen Medical Communications Inc. (2013). License: [CC BY 3.0]
- Figure 2. James Heilman, MD (2011). License: [CC BY-SA 3.0]
- Figure 3. James Heilman, MD (2011). License: [CC BY-SA 3.0]
- Figure 4. Hellerhoff (2010). License: [CC BY-SA 3.0]
