

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Pyloric stenosis describes a thickening of the pyloric muscle. This results in the narrowing of the opening between the stomach and the small intestine, which can cause complete obstruction of the gastric outlet.
The incidence of pyloric stenosis varies between countries and is between 1-3 per 1000 live births.
Aetiology
In pyloric stenosis, there is hypertrophy of the circular and longitudinal muscle layers in the pylorus. This hypertrophy narrows the lumen of the gastric outlet. The length of the pylorus increases also increases. Over time, the lumen will become obstructed, resulting in the postprandial projectile vomiting classically associated with the condition.
The cause of pyloric stenosis is unclear. However, there is evidence to support a neurogenic cause and a link with the neuronal nitric oxide synthase gene.
Risk factors
There are no strongly associated risk factors of pyloric stenosis. However, it is more common in males, firstborns and those with a family history of the condition.
Clinical features
History
The most typical presentation of pyloric stenosis is non-bilious vomiting, which occurs between 2-6 weeks of age. Parents often describe this as projectile vomiting.
This prolonged vomiting can result in weight loss or failure to thrive, constipation, lethargy and haematemesis caused by oesophagitis.
For more information, see the Geeky Medics guide to paediatric history taking.
Clinical examination
Typical clinical findings of pyloric stenosis on examination include:
- Dehydration
- Thin but hungry
- Visible gastric peristalsis
- Palpable pyloric mass in the epigastrium (often difficult to identify)
Differential diagnoses
The main differential diagnoses for vomiting in this age group are:
- Gastroesophageal reflux disease (GORD)
- Malrotation
These two differentials often cause non-projectile vomiting. GORD causes non-bilious vomiting, whereas malrotation causes bilious vomiting.
Investigations
Bedside investigations
Relevant bedside investigations include:
- Test feed with dextrose water: this causes the pylorus to contract, making an epigastric mass more obvious on examination. This may also result in projectile vomiting. If the pylorus was palpable from this test feed, no further imaging is required, and the diagnosis can be confirmed. If the test is inconclusive, an ultrasound will be required.
Laboratory investigations
Relevant laboratory investigations include:
- Blood gas: this will show hypochloraemic hypokalaemic metabolic alkalosis caused by the loss of fluid, hydrogen and chloride through excessive vomiting
- U&Es: this is vital to monitor electrolytes, which will likely be deranged from dehydration
Imaging
Relevant imaging investigations include:
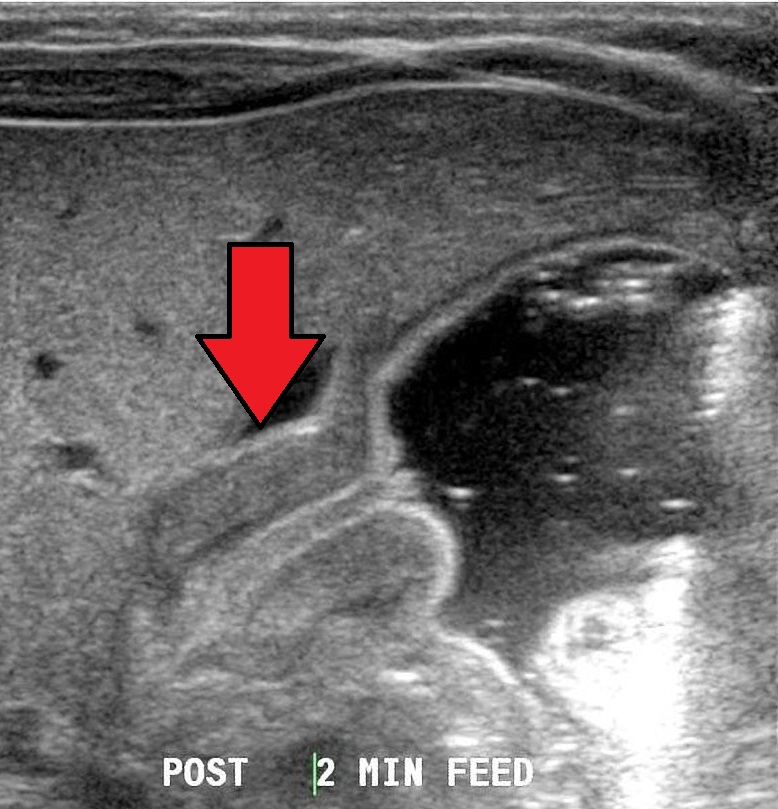
- Abdominal ultrasound: to meet the requirements for diagnosing pyloric stenosis on ultrasound, the pyloric muscle must be over 4mm in thickness, the pyloric muscle length must be over 18mm, and there must be an obstruction preventing the passage of fluid beyond the pylorus, despite gastric peristalsis.
Other investigations
If the previous investigations have been inconclusive, contrast studies can be undertaken, demonstrating a ‘string sign‘ due to the thin long pylorus. This study can also be useful in identifying malrotation.
Diagnosis
There are no set criteria for diagnosing pyloric stenosis. The diagnosis is made by the presence of a pyloric mass on examination or abdominal ultrasound (see ultrasound criteria above).
Management
Patients with pyloric stenosis require both medical and surgical management.
Medical management
Medical management includes:
- Nasogastric tube insertion: this decompresses the stomach and allows accurate recording & replacement of gastric losses
- Preoperative rehydration and correction of electrolyte abnormalities: this should consist of initial fluid boluses of 0.9% sodium chloride, IV maintenance fluids to keep the patient nil by mouth with added potassium per serum levels, and IV replacement fluids to replace NG tube losses
Surgical management
The definitive treatment for pyloric stenosis is Ramstedt’s pyloromyotomy, which involves longitudinally incising the muscle fibres of the hypertrophic pyloric muscle. This defect is left open, allowing the pyloric mucosa to bulge through the incision and providing a wider passage between the pylorus and the duodenum.

Complications
Complications of pyloric stenosis (pre-operatively) include:
- Electrolyte abnormalities
- Dehydration
Surgical complications include perforation, haemorrhage and post-operative infection. The prognosis of pyloric stenosis is good, with most patients experiencing no long-term complications following surgical repair.
Key points
- Pyloric stenosis describes a thickening of the pyloric muscle, which can result in gastric obstruction
- Patients usually present with a history of projectile non-bilious vomiting at 2-6 weeks old
- Blood gases classically show a hypochloraemic, hypokalaemic metabolic alkalosis
- The diagnosis can be made from clinical examination or ultrasound
- Medical management includes fluid resuscitation and electrolyte correction
- The definitive management is Ramstedt’s pyloromyotomy
Reviewer
Paediatric registrar
Editor
Dr Chris Jefferies
References
Text references
- Harper, S.J. and Saeb-Parsy, K., 2013. Essential Surgery E-Book: Problems, Diagnosis and Management. Elsevier Health Sciences.
- John M. Hutson, et al. Jones’ Clinical Paediatric Surgery: Diagnosis and Management. 2008. John Wiley & Sons
- Garfield K, Sergent SR. Pyloric Stenosis. [Updated 2022 May 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. Available from: [LINK]
Image references
- Figure 1. Dr Laughlin Dawes. Pyloric stenosis as seen on ultrasound in a 6 week old. License: [CC BY-SA]
- Figure 2. Kiu77. PyloricStenosisHorizontal. License: [CC BY-SA]
