

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
This guide demonstrates how to perform a subcuticular suture, including step-by-step images of the key stages involved. This guide focuses on a buried continuous dermal suture which is typically used to approximate the most superficial skin edges.
You might also be interested in the following guides:
Equipment
Needle holder (a.k.a. Driver)
Needle holders should be held with your dominant hand.
Put your thumb through one handle and place your ring finger through the other handle. Some people prefer avoiding this as they feel you have greater dexterity and range of movement (this is referred to as “palming”).
 Needle holder closed
Needle holder closed




Toothed forceps (a.k.a. Pickups)
Hold the forceps with your non-dominant hand in the same way you would hold a pen.
Be gentle when using toothed forceps to manipulate skin, do not grip it too tightly or you may damage the wound’s edges.
- Hold the forceps with your non-dominant hand in the same way you would hold a pen



Scissors
Scissors are used for cutting sutures.
Position your index finger at the base of the blades to make your movements more precise.
Rest the blades on your index finger of your non-dominant hand to increase accuracy when cutting.
- Use the scissors to cut sutures



Suture
The suture of choice in this scenario tends to be Monocryl as it is a smooth absorbable monofilament that has reasonable strength and doesn’t cause much irritation to the skin. Monocryl loses 50% of its tensile strength at approximately 3 weeks and completely absorbs within 8 weeks. Care must be taken, if knots are not tied deep under the skin they can erode through the wound whilst healing.
Prolene or nylon can also be used as these are smooth and cause minimal skin irritation. These monofilaments are non-absorbable and therefore have to be removed, which is viewed as an advantage by some. Be sure not to leave too long a length of suture within the skin or it may snap when attempting to remove it, leaving non-absorbable suture within the skin.
Vicryl Rapide is a braided absorbable suture which loses 50% of its tensile strength at 7 days and is completely absorbed at 21 days. Braided sutures are thought to induce a more significant inflammatory response from the skin.
Basic principles of wound management
All wounds should have local anaesthetic infiltration before the intervention. Take care in cosmetically sensitive areas such as the lip as this may distort the normal anatomy.
Following this, they should be thoroughly washed and the wound bed should be examined for internal damage. Patients should be up to date with their tetanus immunisation and contaminated wounds warrant a course of an antibiotic such as co-amoxiclav or a suitable alternative if allergic.
X-rays should be performed if there is suspicion of a fracture or foreign body.
Wound edges should be debrided if the wound is contaminated. If there is no damage deep to the skin, then primary closure can be performed.
Use intuition, some patients have much thicker skin than others and will require a larger suture to facilitate wound closure.
| BODY AREA | SIZE | MATERIAL | REMOVAL TIME |
| Face/Lip | 6-0 | Monofilament, non-absorbable | 3-5 days |
| Scalp | 3-0, 4-0 | Monofilament, non-absorbable | 7-10 days |
| Chest/Abdomen/Back | 3-0, 4-0 | Monofilament – may be absorbable or non-absorbable | 10-14 days |
| Limbs | 3-0 to 5-0 | Monofilament – may be absorbable or non-absorbable | 10-14 days |
| Hands | 4-0 or 5-0 | Monofilament – usually non-absorbable | 10-14 days |
| Nailbed | 6-0 | Braided, rapidly absorbable | Absorbable |
Setup for subcuticular sutures
This is a sterile procedure, and therefore the wound and surrounding skin must be prepared with antiseptic solution before placing a drape around the sterile field. You must wash your hands and wear sterile gloves, taking care not to ‘de-sterilise’ during the procedure. Although you may not need a surgical gown, you must don gloves taking care not to touch the external surface.
Wash the wound and debride the skin edges if ragged or dirty and if you are certain there is no deep tissue damage you may proceed to close the skin.
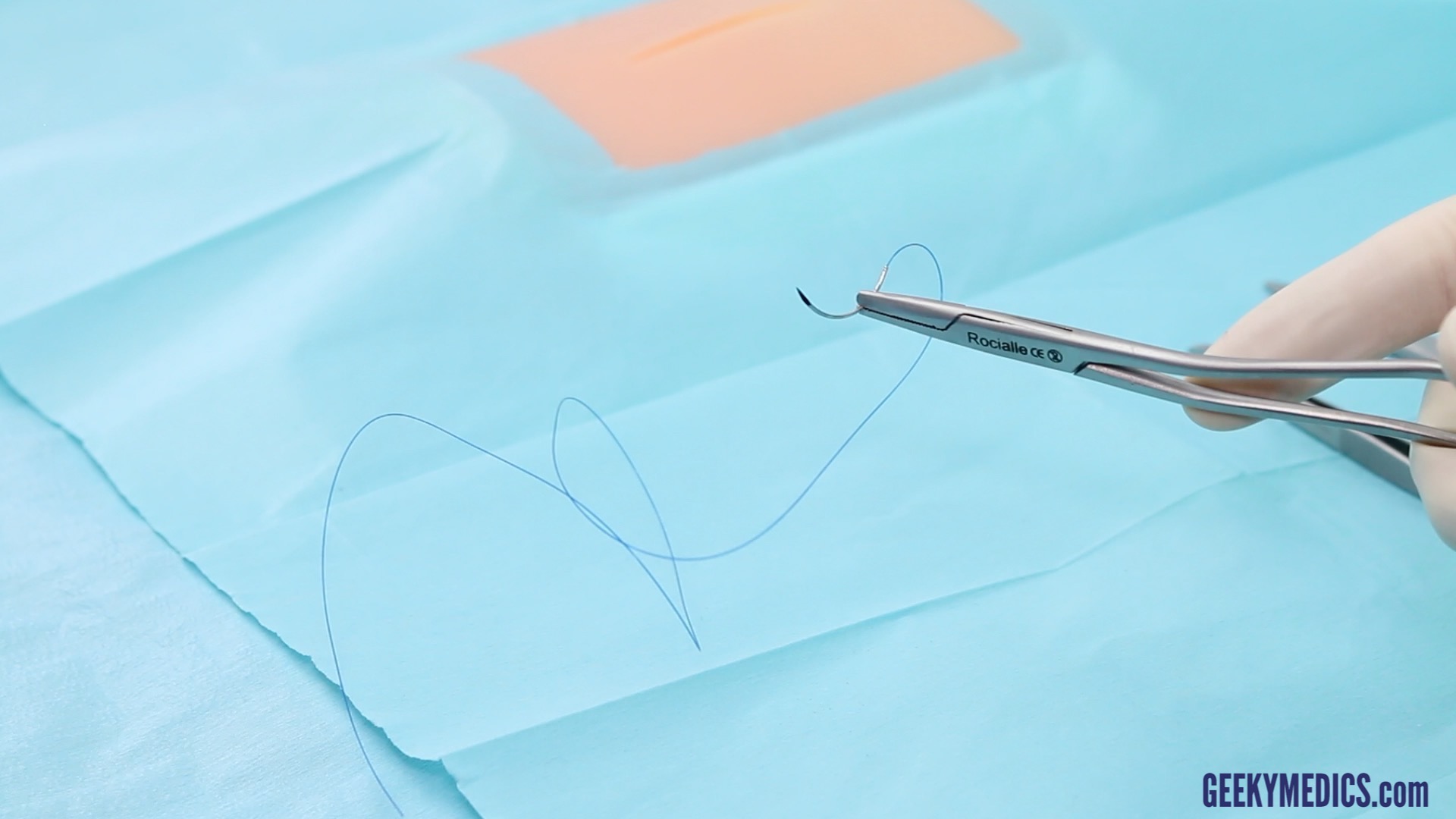
Load your needle holder by placing the needle in the tip of the holder, two-thirds of the distance from the tip to the thread.
- Load the needle between the apex of its curvature and two-thirds from the needle tip

Performing a subcuticular suture
This technique generally follows dermal suturing to complete a layered closure. It is often performed with an absorbable suture, however, non-absorbable material can be used and removed once the wound has reached an adequate strength. The technique can be thought of as a buried continuous suture.
Procedure
1. The suture is started at one apex of the wound. It can either be started with a buried dermal knot or a free length of suture out of the skin which can later be trimmed (if absorbable) or removed (if non-absorbable).
- At the apex of the wound, pass your need from deep to superficial to begin your buried knot








2. It is easier to suture from ‘far to near’ or from your dominant side towards your non-dominant side (right to left assuming right-handedness).
3. Starting from the chosen apex, take a bite deep to the epidermis that should curve parallel to the skin surface and exit in the same plane approximately 5-10mm along the wound, taking care to stay at the same level. It is useful to evert the skin edge with the toothed forceps to help. Ensuring that your suture is not too superficial will also aid wound eversion.
4. Remove the needle and pull the stitch through.
5. Perform a mirror image on the opposing side keeping the bites the same depth and length. If one side of your wound is longer than the other, bigger bites must be taken on the longer side of the wound to compensate for excess skin at the apex of the wound (called a ‘dog ear’).
6. Continue this down the length of the wound, pulling the suture taut as you oppose the skin edges.
- Pass your needle from deep to superficial, so that the tip exits at the very apex of the wound within the dermis











7. Once the distal apex is approached a knot needs to be secured (if not leaving the ends free).
8. Two deeper opposing bites are taken and then a knot can be instrument tied using a loop of suture or, more commonly, an ‘Aberdeen knot’.
9. To do this bring the needle out at the apex of the wound, pull this through with your non-dominant hand leaving behind a loop big enough for the thumb and index finger of your dominant hand. With the loop under tension (created by your thumb and index finger) reach through with your middle finger and grasp the free end of the suture. Keeping hold of the needle in the non-dominant hand, pull the loop down to form a knot. Repeat this 2-3 times and on the final knot bring the needle through the loop to secure the knot. If you create too many loops the knot will increase in size and is more likely to erode through the skin.
10. Once a secure knot is formed in the apex, pass the needle back deep through the wound emerging adjacent to the wound, this will bury the knot.
- To bury the final knot, you first pass the needle from superficial to deep at the apex of the wound



















Wound care and safe disposal of sharps
Once you have completed suturing, you must ensure that you account for and dispose of your sharps immediately in a sharps bin.
The wound should be washed and dried, then dressed appropriately. Dressings depend on the site of the body and professional preference, below are some examples:
- Face: Cover with steristrips and Micropore tape or provide chloramphenicol 1% ointment.
- Limb: Cover with a non-adhesive dressing such as Jelonet, Mepetel, or Silflex then gauze, Velband and crepe. A small wound may be covered with an OpSite or a Mepore waterproof dressing.
- Torso: Cover with non-adhesive then Opsite or Mepore. If large you may consider gauze and Mefix.
Follow up
All wounds should be reviewed in 5-7 days and sutures removed (if non-absorbable) as per the table above.
Authors
Mr Colin Brewster
Plastic Surgery Registrar
Mr Iain Anderson
Plastic Surgery Registrar
