

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
There are three major groups of back muscles:
- Superficial: attached to the shoulder girdle
- Intermediate: attached to the posterior thorax
- Deep: attached to the vertebral column
The first two groups (superficial and intermediate) are referred to as the extrinsic back muscles. The deep group is the intrinsic muscle group. This article will focus on the superficial group.
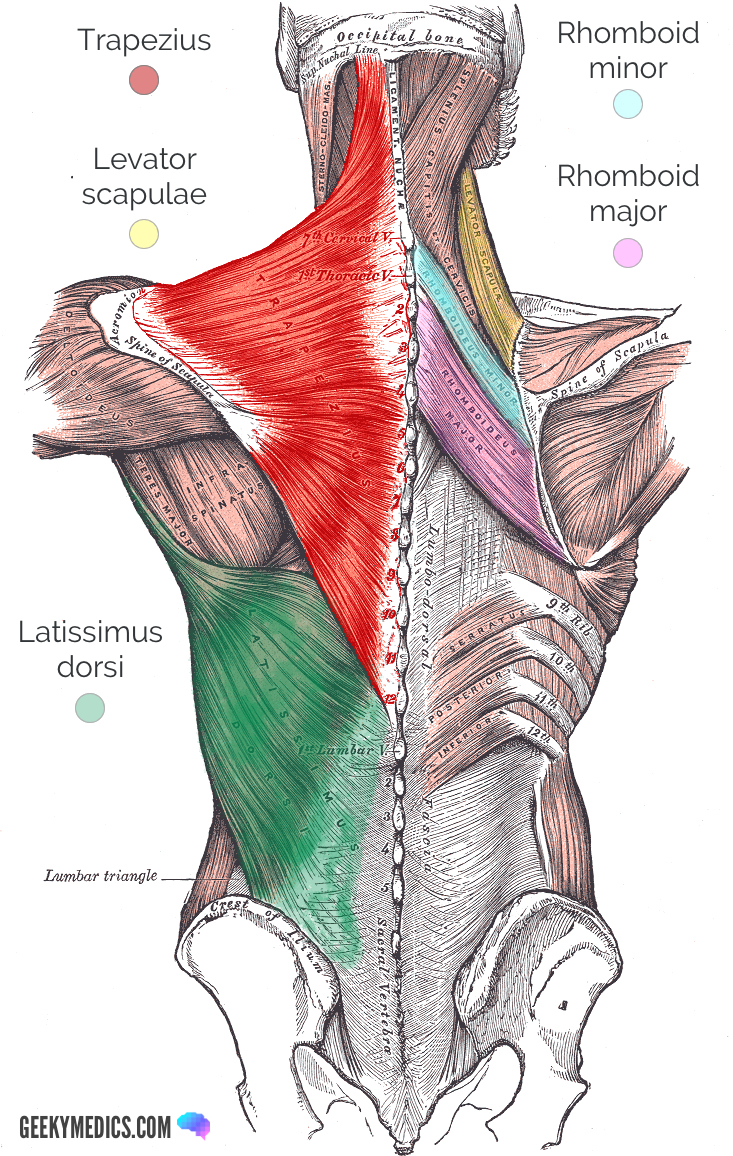
The superficial back muscles are covered by skin, subcutaneous connective tissue and a layer of fat. The muscles of this group include:
- Trapezius
- Latissimus dorsi
- Levator scapulae
- Rhomboid major and rhomboid minor
Trapezius
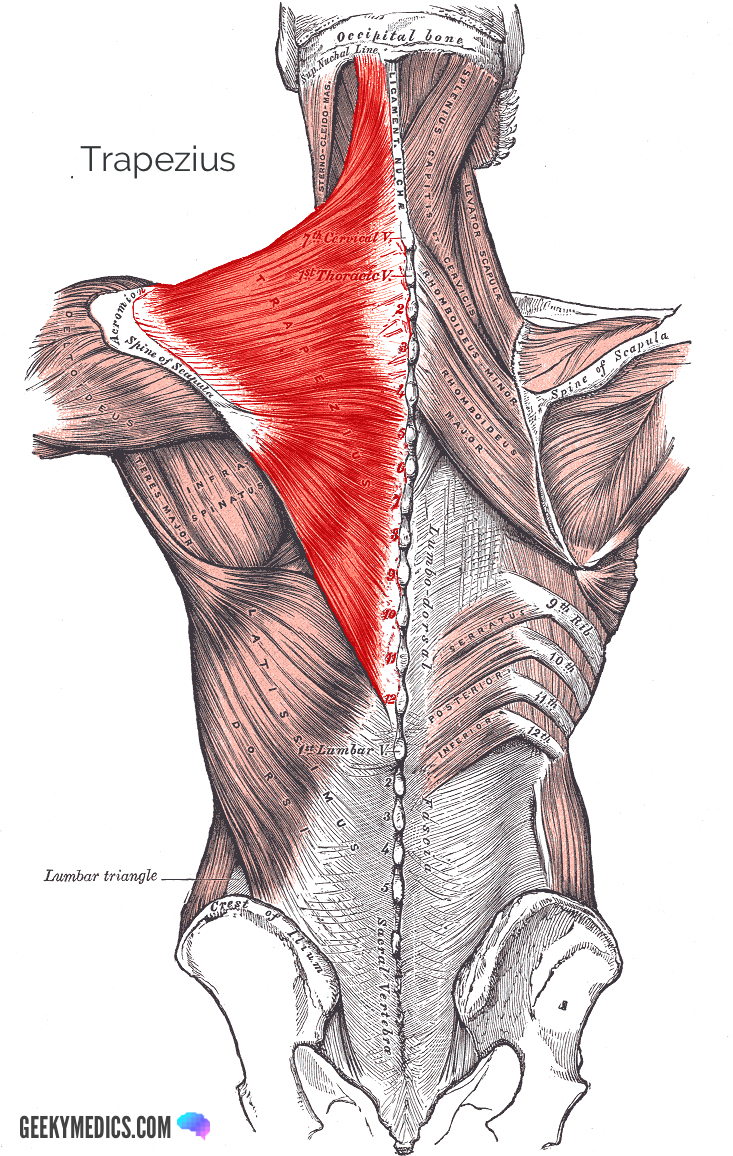
The trapezius is a primary mover of the scapula that assists in superior and inferior rotation, retraction, and elevation and depression of the scapula and shoulder complex.
It is a triangular muscle unilaterally and appears as a trapezoid-shaped muscle when the left and right trapezius are viewed on the back.
It is divided into three distinct segments, named the superior (s), middle (m) and inferior (i) trapezius, which have slightly varied attachment points.
Origin and insertion
Originating from the superior nuchal line (s), nuchal ligament (s; m) and the spinous processes of C7 to T12 (m; i), the trapezius muscle converges onto the lateral 1/3 of the clavicle (s), acromion (m) and spine of the scapula (i).
Fibre orientation
The trapezius fibres originate broadly along the vertical midline of the vertebral column before converging on their insertion points around the acromion, spine of the scapula and lateral one-third of the clavicle.
Function
We will consider the different heads of the trapezius:
- Superior head: elevation, rotation during arm abduction
- Middle head: retraction
- Inferior head: depression, rotation during arm adduction
- All three heads together: retraction and fixation of the scapula
Innervation
The motor innervation is derived from the spinal accessory nerve (cranial nerve XI). The sensory innervation is derived from the dorsal ramus of spinal nerves C3-C4.
Arterial supply
The trapezius is supplied by either of the superficial cervical arteries, or the superficial branch of the transverse cervical artery.
Clinical relevance: trapezius
Lower brainstem and upper cervical cord lesions can interfere with the function of the spinal accessory nerve (CN XI), leading to paresis or paralysis of the trapezius (and sternocleidomastoid) muscles. Patients may not be able to shrug their shoulders and will have significant weakness against inferior shoulder resistance.1,2
The trapezius, with sensory innervation from C3 and C4 may also be the site of origin of tension headaches. Chronic tension or contraction of these muscles can cause localised elevations of prostaglandins and lactate, irritating nociceptive receptors. This irritation can cause a referred pain in the distribution of C2-C4, manifesting as a headache or neck pain.3
Latissimus dorsi
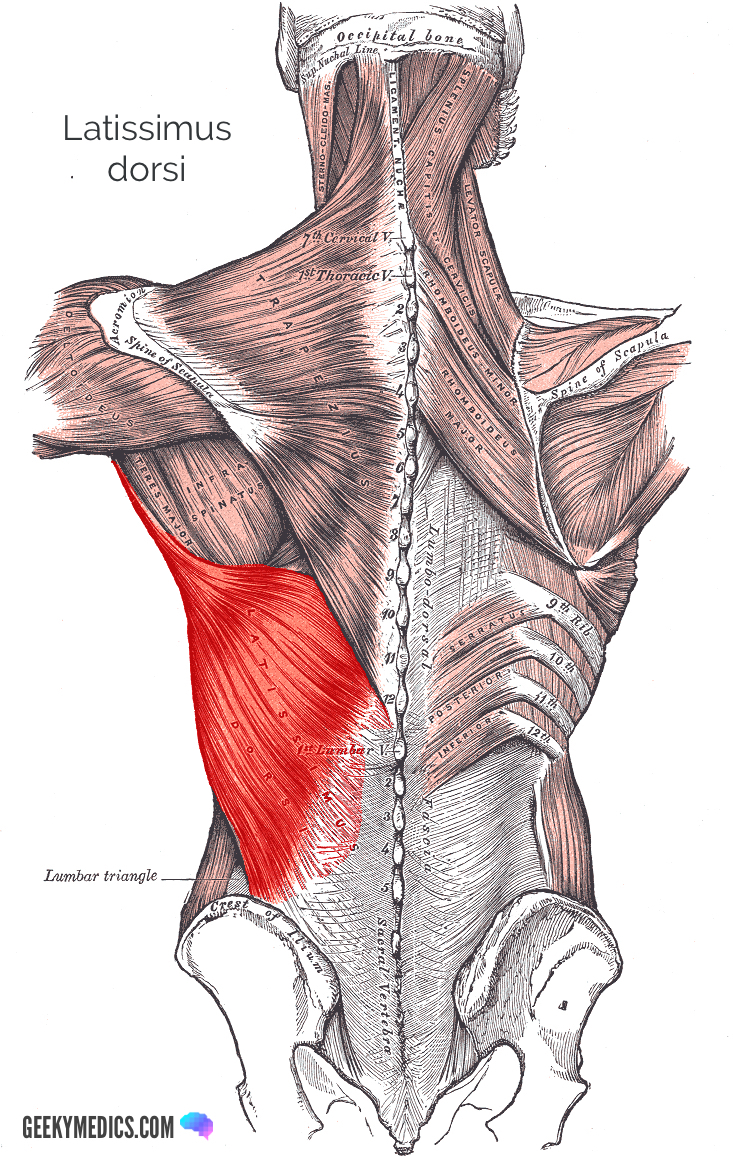
The latissimus dorsi is a broad, flat muscle that covers the entire lower back.
Origin and insertion
The latissimus dorsi originates from the iliac crest, thoracodorsal fascia and T7-L5 spinous processes, converging to insert via a single, flat tendon in the floor of the intertubercular (bicipital) groove of the humerus.
Fibre orientation
The fibres of latissimus dorsi begin broadly and converge onto a single common tendon.
Function
A powerful extensor and adductor of the shoulder, latissimus dorsi also assists in internal rotation of the humerus.
Innervation
The motor and sensory innervation is supplied by the thoracodorsal nerve, which derives fibres from spinal roots C6-C8.
Blood supply
Latissimus dorsi is supplied by the thoracodorsal branch of the subscapular artery.
Clinical relevance: latissimus dorsi
Latissimus dorsi is a large muscle that, when atrophied, can cause significant asymmetry in the back.
While it is a strong muscle for adduction, internal rotation and extension of the humerus, we can do without it. The tendon for latissimus dorsi can be harvested for tendon repairs or tendon transfers. An asymmetric or non-functional latissimus dorsi is not always due to a nerve lesion and can result from prior transfer surgery.2
Levator scapulae
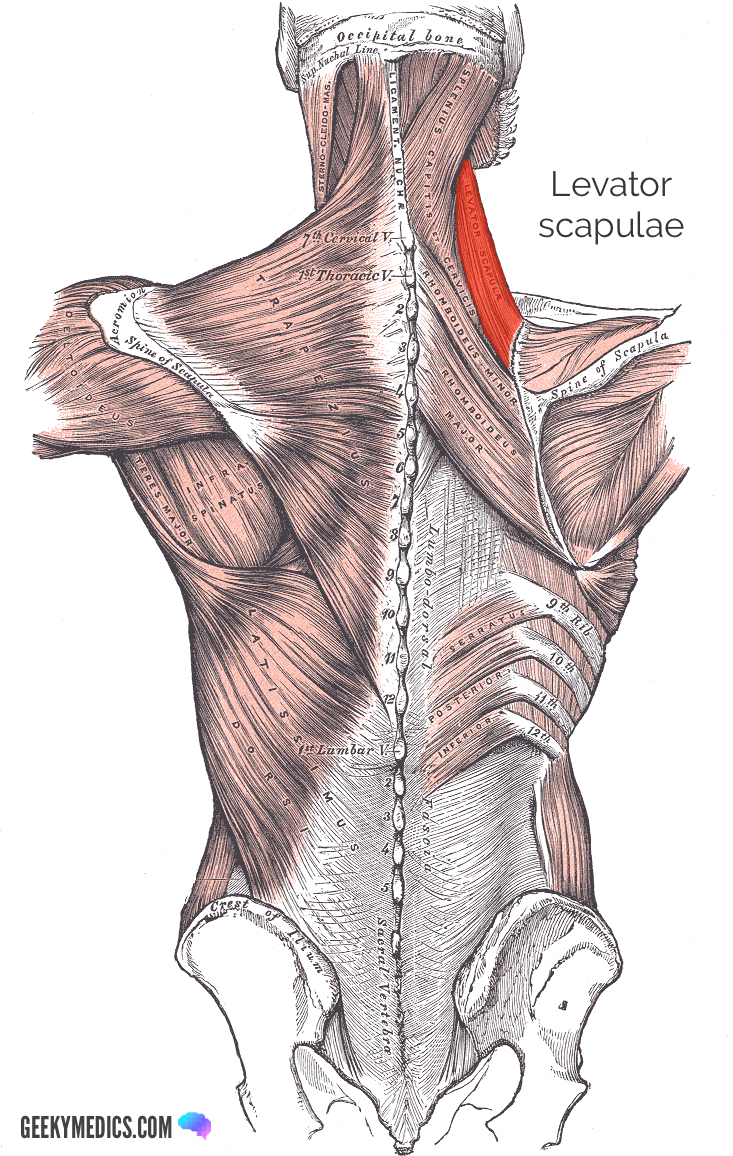
Levator scapulae is a relatively short and thin strap muscle of the superficial back compartment.
Origin and insertion
Levator scapulae originates from the transverse processes of C1-C4, and inserts onto the medial border of the scapula at the superior angle.
Fibre orientation
The fibres of levator scapulae have a straight orientation, consistent with a strap.
Function
Levator scapulae is a synergist (assistor) in elevation of the scapula.
Innervation
The motor and sensory innervation of levator scapulae is derived from the dorsal scapula nerve, the first branch of the brachial plexus arising from the C5 nerve root.
Blood supply
Levator scapulae is supplied by the similarly named dorsal scapular artery.
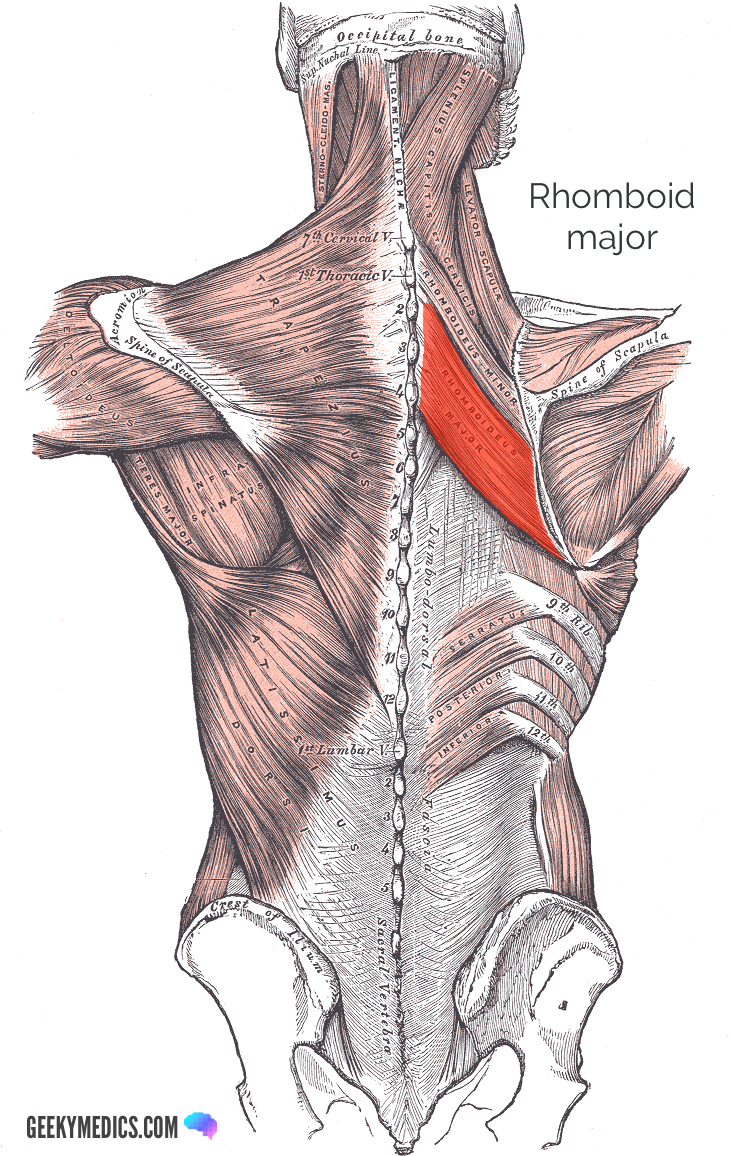
Rhomboid major
The rhomboid major is a broad and thin strap-like muscle that connects the scapula to the spinous processes of the vertebral column.
Origin and insertion
Rhomboid major originates on the spinous processes of T1-T5, before inserting on the medial border of the scapula.
Fibre orientation
The fibres of rhomboid major resemble a strap muscle.
Function
Rhomboid major is a scapula retractor and inferior rotator (when adducting the humerus).
Innervation
The motor and sensory innervation of the rhomboid major muscle is derived from the dorsal scapular nerve of the C5 nerve root.
Blood supply
Rhomboid major is supplied by the dorsal scapular artery.
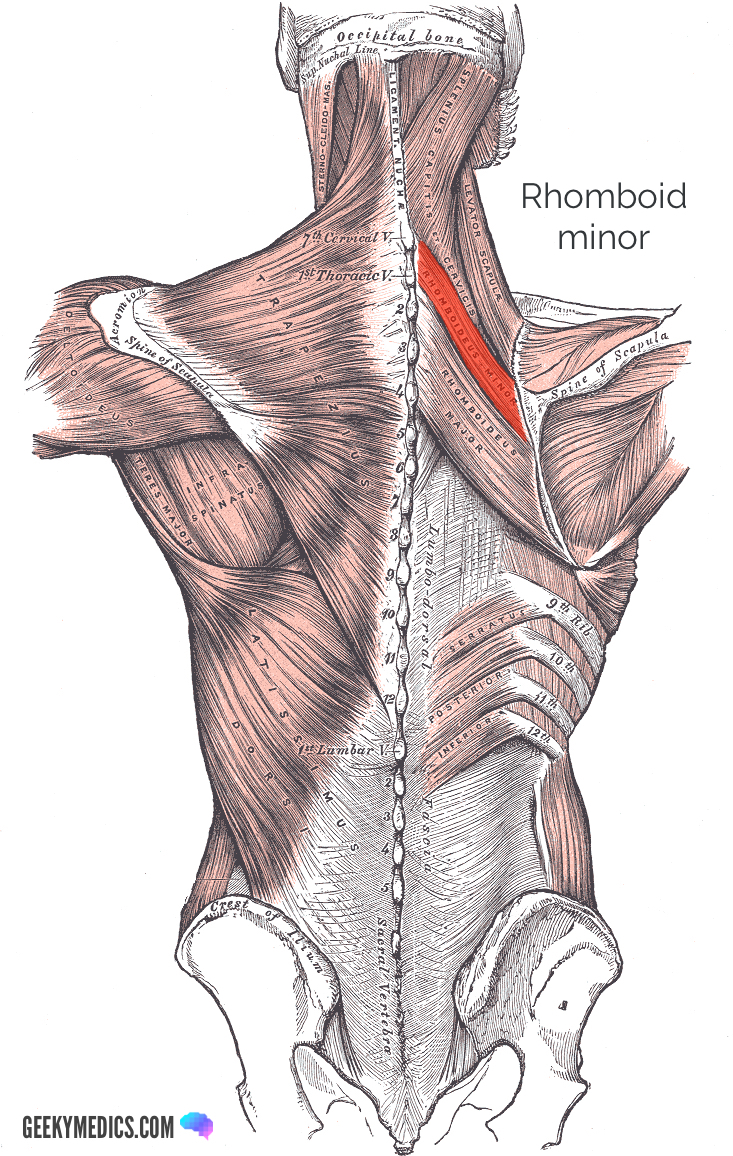
Rhomboid minor
The rhomboid minor is a narrow and thin strap-like muscle that connects the scapula to the spinous processes of the vertebral column. It is smaller and more superiorly located than the adjacent rhomboid major.
Origin and insertion
Rhomboid minor originates on the spinous processes of C7-T1, before inserting on the medial border of the scapula (superior to rhomboid major).
Fibre orientation
The fibres of rhomboid minor resemble a narrow strap muscle.
Function
Rhomboid minor is a scapula retractor and inferior rotator (when adducting the humerus).
Innervation
The motor and sensory innervation of the rhomboid minor muscle is derived from the dorsal scapular nerve of the C5 nerve root.
Blood supply
Rhomboid minor is supplied by a deep branch of the transverse cervical artery.
The next article will focus on the intermediate muscles of the back.
Clinical relevance: rhomboid muscles
Weakness in the rhomboid major and minor muscles can contribute to scapula winging.
This refers to weakness in the muscles that assist the scapula in adhering closely to the ribs and thoracic cage. Serratus anterior is the primary muscle contributing to this, and scapula winging is classically described as a lesion to the long thoracic nerve of the brachial plexus.
Quiz
Test your knowledge of the superficial muscles of the back to the test with our quiz.
References
Reference images
- Trapezius: By Mikael Häggström, used with permission. License: [Public domain]
- Latissimus dorsi: By Mikael Häggström, used with permission. License: [Public domain]
- Levator scapulae: modified by Uwe Gille. License: [Public domain]
- Rhomboid major: modified by Uwe Gille. License: [Public domain]
- Rhomboid minor: modified by Uwe Gille. License: [Public domain]
Reference texts
- Sinnatamby, C. S. (2011). Last’s Anatomy, International Edition: Regional and Applied. Elsevier Health Sciences.
- Moore, K. L., Dalley, A. F., & Agur, A. M. (2013). Clinically oriented anatomy. Lippincott Williams & Wilkins.
- Nardone, R., & Tezzon, F. (2003). The trigemino‐cervical reflex in tension‐type headache. European journal of neurology, 10(3), 307-312.
