

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Toothache, and other dental problems, are common presenting complaints in both primary and secondary care.1 Having a basic understanding of the dentition (or teeth) is important for all healthcare professionals.
This article will discuss adult and child dentition, different tooth types, basic tooth cross-sectional and surface anatomy, and the various methods of dental notation. Relevant clinical considerations are discussed throughout the article.
Primary and permanent dentition
In the human mouth, teeth make up roughly 20% of the total surface area of the oral cavity.
There are 2 types of dentition that develop in humans:
- Primary (colloquially termed baby or milk) teeth of which there are 20 in total, made up of 8 incisors, 4 canines and 8 molars.
- Permanent (or adult) teeth of which there are 32 in total, made up of 8 incisors, 4 canines, 8 premolars and 12 molars.
The location of teeth can be divided into upper (maxillary) or lower (mandibular) and into left and right halves down the midline to form quadrants (upper right, upper left, lower right, and lower left).
Tooth types
The 4 main tooth types are incisors, canines, premolars, and molars. Premolars are only present in the permanent dentition.
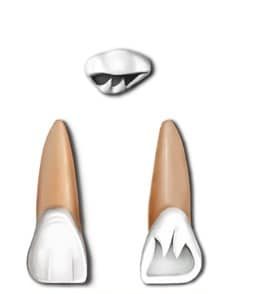
Incisors
There are 8 incisors in both the permanent and primary dentition, with four in each dental arch. The two types are the central incisors and lateral incisors.
The central incisors are closest to the midline and the lateral incisors are the second teeth from the midline. The mandibular and maxillary incisors function together to cut food, enable articulate speech, help maintain lip support and aesthetics.2
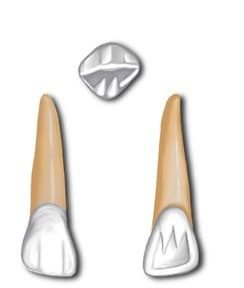
Canines
There are 4 canines in both primary and permanent dentition; 2 maxillary and 2 mandibular. They are the third teeth from the midline and function to pierce or tear food during mastication using the pointed tip (or cusp).
Due to their larger crown, the overlap of maxillary and mandibular canines separates the posterior teeth when the mandible is moved from side to side. This prevents potentially damaging forces to the premolar and molar teeth.
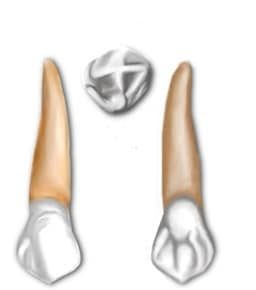
Premolars
These 8 teeth are only present in the permanent dentition. There are 4 maxillary and 4 mandibular premolars; divided into 1st premolars and 2nd premolars, with the former lying closer to the midline.
They lie between canines and molars and generally have 2 cusps. Their role is to assist the canines in shearing or cutting food and to maintain the vertical dimension of the face, by supporting the corners of the mouth and cheeks.2

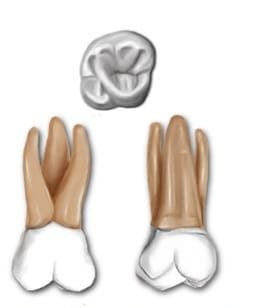
Molars
There are 8 molars in the primary dentition: 4 maxillary and 4 mandibular. There are 12 molars in the permanent dentition: 6 maxillary and 6 mandibular. They are the most posterior teeth in the mouth and their function is to crush and chew food, maintain vertical dimensions of the face and they help maintain continuity between both arches keeping other teeth in alignment.2
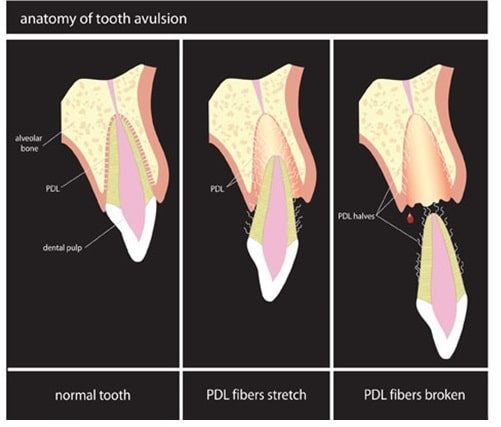
Clinical relevance: tooth avulsion
The most important dental injury to be aware of is an avulsed permanent tooth; one of the few dental emergencies. Commonly affecting the incisors (due to their anterior position in the mouth), a significant force can lead to the whole tooth (crown and root) losing its attachment to the bone.
Healthcare professionals should be aware of the advice to give in these situations:8
- Find the tooth and pick it up by the crown (white part). Avoid touching the root.
- If the tooth is dirty wash it for no more than 10 seconds under cold running water and try to replant the tooth back into position. Bite on a clean handkerchief to hold it in position.
- If this is not possible, store the tooth in a glass of milk, saline or in the mouth keeping it between the back teeth and inside of the cheek.
- If the patient is young and there is a risk of swallowing the tooth, get them to spit into a container and place the tooth in it.
- Avoid storage in water.
- Seek emergency dental treatment immediately.
Tooth anatomy
The tooth can be divided into two main components: the crown and the root (figure 7). The crown is the part of the tooth that is visible in the mouth and the root is the part that lies within the jawbone.
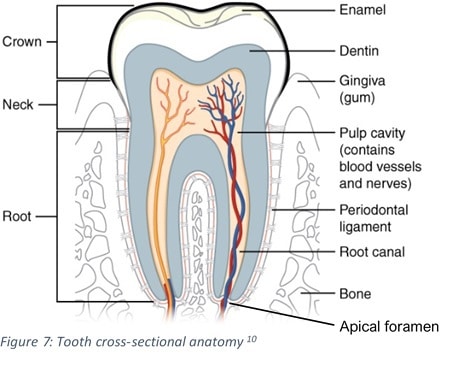
Enamel
The crown is covered by a hard, white, mineralised layer called enamel. This is the hardest substance in the human body made mostly of hydroxyapatite, a crystalline calcium phosphate.
Enamel is an avascular substance and contains no nerve supply. Due to its high mineral content, enamel is at risk of demineralisation. The main reasons for enamel loss are:
- Dental caries (or tooth decay): acid releasing bacteria utilising dietary sugars as an energy source. The main causative bacteria is streptococcus mutans.
- Erosion: exposure of the teeth to acid which can be from extrinsic sources (acidic food and drink or medications) or intrinsic sources (gastric acid from the stomach contacts the teeth).
- Attrition: caused by tooth to tooth contact.
- Abrasion: mechanical wear other than tooth to tooth contact, such as excessive toothbrushing.
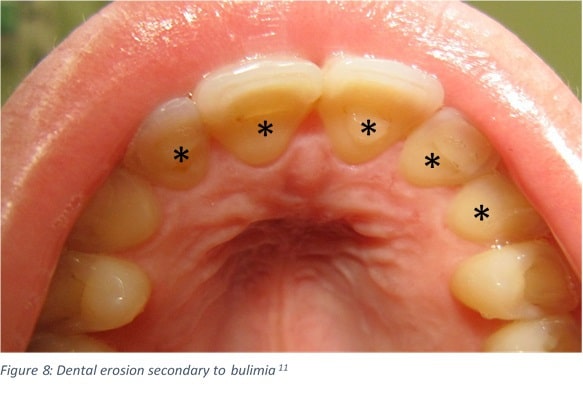
Clinical relevance: tooth enamel erosion
Tooth enamel erosion is considered an oral manifestation of several medical conditions, including eating disorders associated with vomiting practices, such as bulimia and occasionally gastroesophageal reflux disease (GORD).
Typically, erosions present on the inner (palatal) surfaces of the maxillary teeth (figure 8 starred).
Dentine
This layer lies beneath the enamel and cementum. Dentine is a yellow coloured, vascular and innervated tissue that makes up most of the tooth structure.
Dentine is less mineralised than enamel and softer, therefore more at risk of breakdown due to the same causes of enamel loss. Its role is to provide support to enamel and allow transmission of nerve impulses detected as pain.
Clinical relevance: tetracycline staining
The antibiotic tetracycline should not be given in pregnancy and is contraindicated in children under 12 years old.
Administration of the drug whilst the teeth are undergoing calcification (from in utero up to 12 years old), will cause a yellow or brown-banded discolouration on the teeth, due it binding to the dentine (figure 9).

Pulp and root
Beneath the dentine lies a neurovascular bundle called the pulp. The pulp comprises a central chamber, pulp horns and root canal. The primary functions of the pulp are to lay down more dentine, supply nutrients to the organic components of the tooth tissue and detect changes in temperature and pressure, transmitting these as nerve impulses detected by the brain as pain (this is a protective function).
The maxillary branch (V2) of the trigeminal nerve (CN V) supplies all sensory innervation to the upper teeth and the mandibular branch (V3) supplies all sensory innervation to the lower teeth.
Part of the pulp cavity along with the root canal make up the root of the tooth. The root is the part of the tooth that sits within the alveolus of the maxilla and mandible. Its most superficial surface is covered by cementum, a specialised calcified substance which attaches the teeth to the bone by anchoring the periodontal ligament (PDL).
The PDL serves to help with load-bearing of the teeth, transmit information with it being highly innervated tissue, providing nutrition to surrounding tissue and remodelling of the surrounding alveolar bone.
The root canal serves as a continuation of the pulp cavity through which the neurovasculature resides and then enters/exits through the apical foramen.
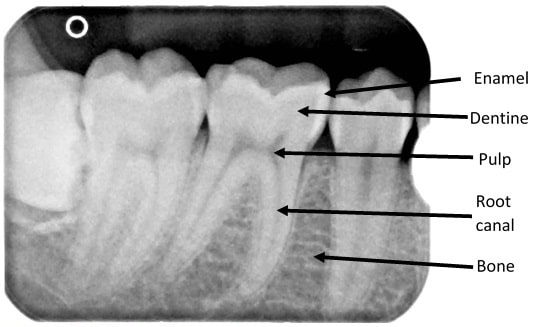
Clinical relevance: dental pathology
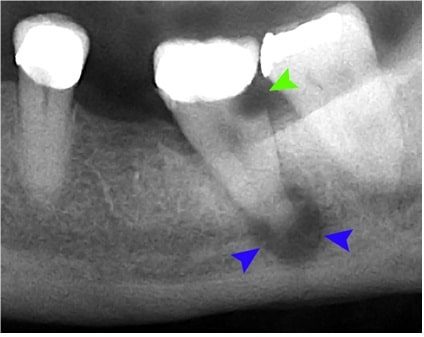
When examining dental radiographs (figure 10), the enamel appears as the outermost superior radiopaque layer. The dentine is less mineralised so appears less radiopaque and is deep to the enamel, followed by the pulp and root canals which are generally radiolucent in comparison. The alveolar bone which provides the socket in which the tooth sits has a radiopaque trabeculated appearance that lies between teeth at the root level.
Dental caries (or tooth decay) appear radiolucent on a dental radiograph (figure 11 green arrow). As bacteria progress into the pulp, this leads to inflammation and a condition called pulpitis. Symptoms include increased sensitivity to hot and cold, pain can be intermittent and brief episodes that resolve after minutes if the stimulus is removed (reversible) or continuous severe pain that arises without provocation (irreversible).
When bacteria track down the root canal system and egresses through the apical foramen, this can lead to the formation of a radiolucency at the apex causing a periapical abscess or dental abscess (figure 11 blue arrows). Typical clinical features of an abscess include:
- Intense throbbing pain
- Referred pain to the ear, jaw or neck
- Bad taste
- Redness or swelling of the gum around the offending tooth (figure 12)
If the infection spreads, systemic features can develop including fever, malaise and lymphadenopathy.
In severe cases, the infection can spread into the fascial spaces of the head and neck leading to reduced mouth opening and airway compromise. This would require urgent hospital admission with anaesthetic and maxillofacial input.
Treatment of a dental abscess involves removing the nidus of infection and draining the pus. This can be achieved in several ways:
- Root canal treatment (RCT): removal of the pulp and neurovasculature of the root canal system, irrigating with disinfectant and sealing the root canal and empty chamber with filling materials.
- Removal of the tooth (extraction)
- Incision and drainage: can be done intraoral (inside the mouth) or extra-orally (usually on the neck) depending upon how extensive the swelling is. This is usually only a temporary solution and the tooth still requires either a RCT or extraction.

Tooth surface terminology
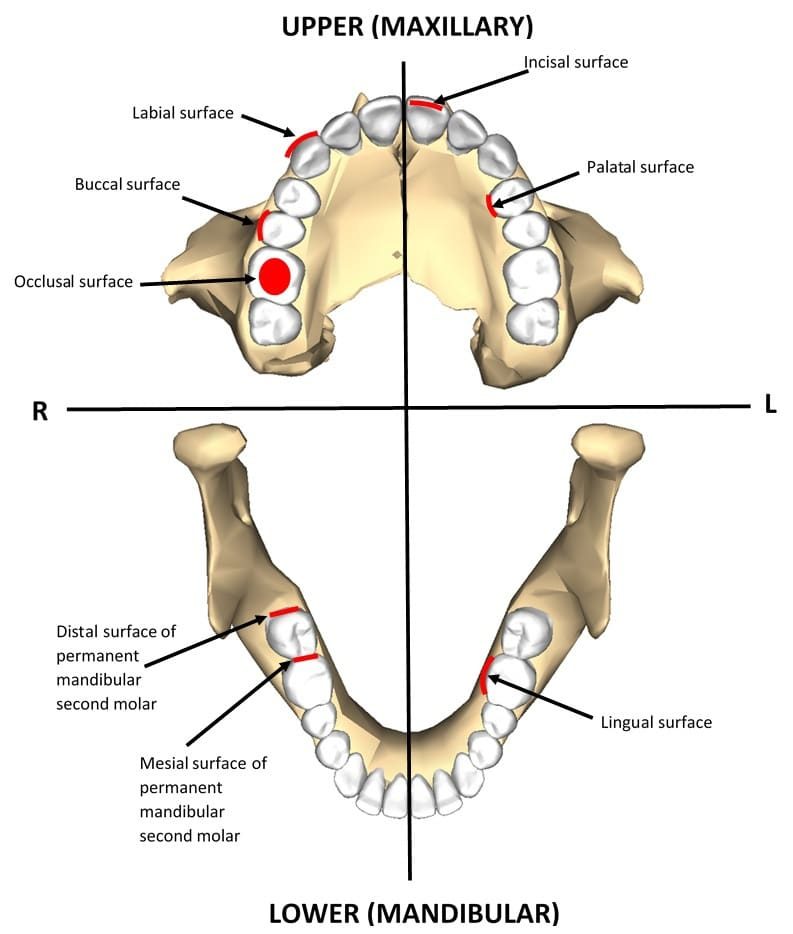
All teeth have 5 surfaces that are named according to their usual alignment within the dental arch. These are termed:
- Facial: this is the surface facing towards the face so resting either against the inner lips or cheek. In anterior teeth (incisors and canines) they are also referred to as labial surfaces and in posterior teeth (premolars and molars) buccal.
- Lingual: this is the surface facing towards the tongue. In maxillary teeth this surface is also referred to as palatal, due to their proximity to the hard and soft palate.
- Masticatory: this is the surfaces that are used for mastication. In anterior teeth, they are referred to as incisal surfaces and occlusal surfaces in posterior teeth.
- Mesial: this is the surface on the tooth that lies closest to the midline.
- Distal: this is the surface of the tooth that lies further from the midline.
Tooth notation
The three main systems for tooth designation are the Universal Numbering System (UNS), the International Numbering System (INS) and the Palmer Notation Method. There is also an Alpha-numeric variant of the Palmer notation.
This article will focus on the INS, Palmer and Alpha-numeric systems as they are common in the UK, unlike the UNS which is mostly used in the US.
International Numbering System (INS)
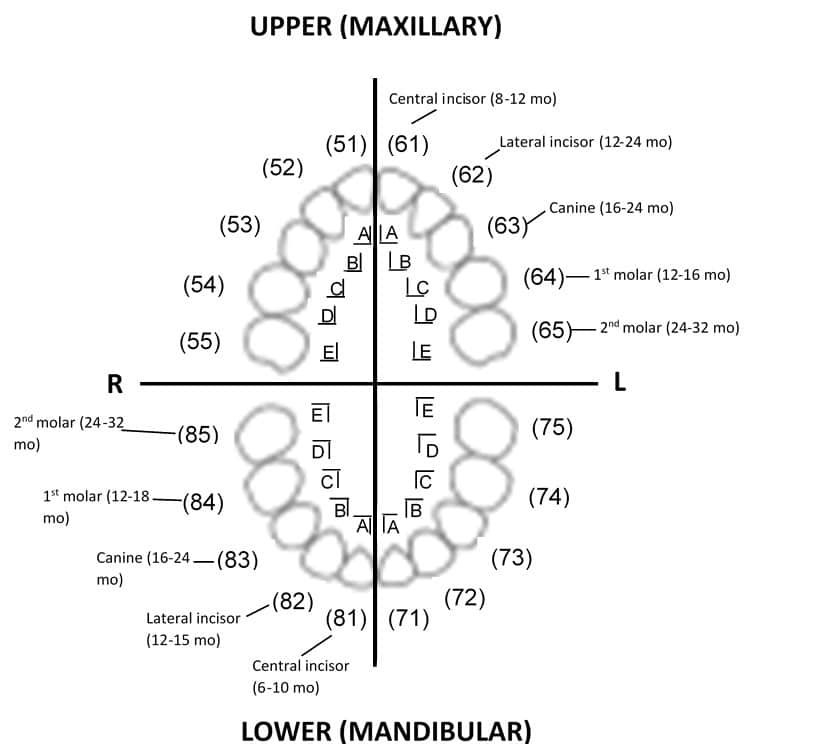
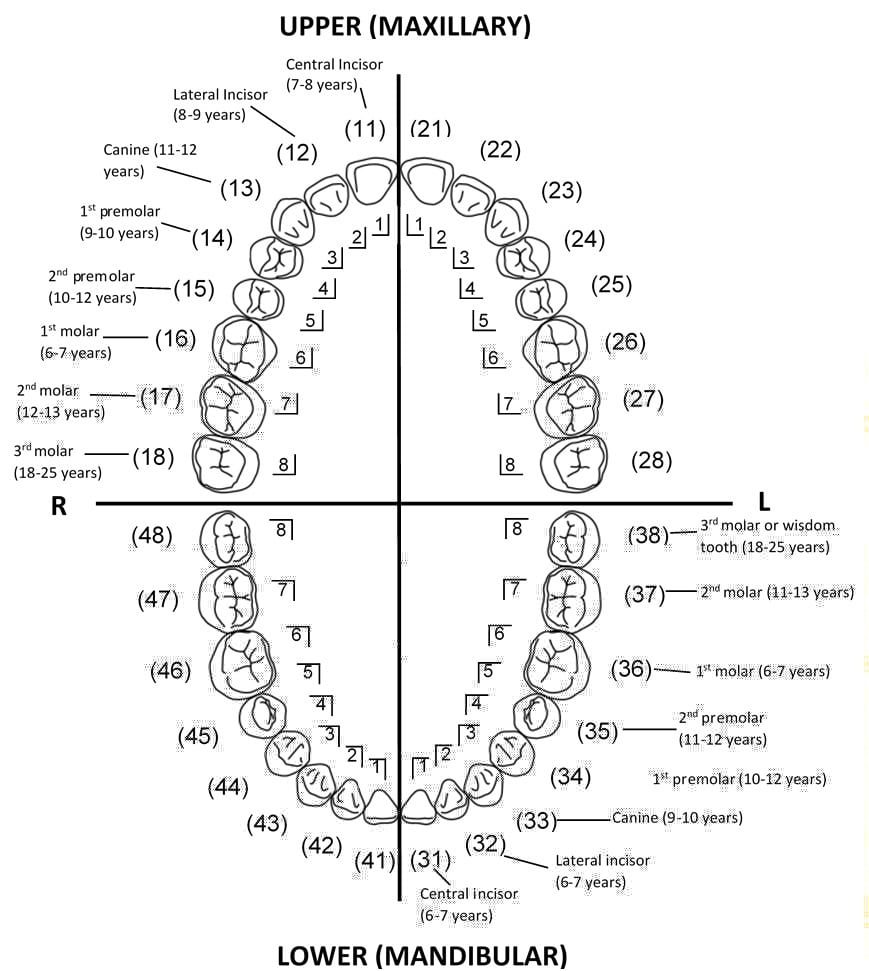
Designed by ISO and the WHO, the teeth are designated a two-digit code; the first digit representing the quadrant (1 to 4 for permanent and 5 to 8 for primary), whilst the second digit indicates the tooth’s position in the quadrant (1 to 8 for permanent and 1 to 5 for primary). For example, 11 = upper right central incisor.
Palmer notation and Alpha-numeric
This consists of a symbol (or abbreviation in the Alpha-numeric system) designating the quadrant and a number that indicates the tooth position from the midline. Permanent teeth are numbered 1 to 8, with primary teeth represented by a letter A to E.
- ┘ or UR = upper right quadrant
- └ or UL = upper left quadrant
- ┐ or LR = lower right quadrant
- ┌ or LL = lower left quadrant
Figure 14 and 15 demonstrate both the INS and Palmer notation method for classifying primary and permanent teeth. The D-A-Q-T System is used to help users describe an individual tooth:
- D for dentition (primary or permanent)
- A for arch (maxillary or mandibular)
- Q for quadrant (left or right)
- T for tooth type (incisor, canine, premolar or molar)
Editor
Dr Chris Jefferies
References
- British Dental Association. NHS dental charge increases covering cuts and undermining prevention. 2019. Available from: [LINK]
- Scheid RC, Weiss G. Woelfel’s Dental Anatomy. 8th Philadelphia. Lippincott Williams & Wilkins. 2012.
- Ανώνυμος Βικιπαιδιστής. Maxillary central incisor. Adapted by Geeky Medics. License: [CC-BY]. Available from: [LINK]
- Ανώνυμος Βικιπαιδιστής. Maxillary lateral incisor. Adapted by Geeky Medics. License: [CC-BY]. Available from: [LINK]
- Ανώνυμος Βικιπαιδιστής. Maxillary canine. Adapted by Geeky Medics. License: [CC-BY]. Available from: [LINK]
- Ανώνυμος Βικιπαιδιστής. Maxillary first premolar. Adapted by Geeky Medics. License: [CC-BY]. Available from: [LINK]
- Ανώνυμος Βικιπαιδιστής. Maxillary first molar. Adapted by Geeky Medics. License: [CC-BY]. Available from: [LINK]
- Dental Trauma Guide. IADT treatment guidelines for avulsion. Available from: [LINK]
- Endsurg. Dental avulsion. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- OpenStax College. 2409. Adapted by Geeky Medics. License: [CC-BY]. Available from: [LINK]
- James Heilman, MD. BulemiaEnamalLoss. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- Clifton M.Carey. Examples of tooth staining. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- Dr. Cross. ZELLFAZE MN01 MP10 012. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- Coronation Dental Specialty Group. Tooth decay and abscess xray. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- Damdent. Abces parulique. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- Anatomography. Maxilla close-up inferior. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- Anatomography. Mandible close-up superior. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- Renee1137. Mandibular second premolars01-01-06. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
- Kaligula. Human dental arches. Adapted by Geeky Medics. License: [CC-BY-SA]. Available from: [LINK]
