

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
The central nervous system uses ascending and descending pathways to communicate with the external environment. In this article, we will introduce the concept of ascending pathways, the different pathways to understand and provide context for these with real-world clinical examples.
Ascending pathways transport sensory information in afferent pathways from the body to the brain.
Afferent is derived from ‘ad’ (toward) and ‘-ferre-‘ (to carry).
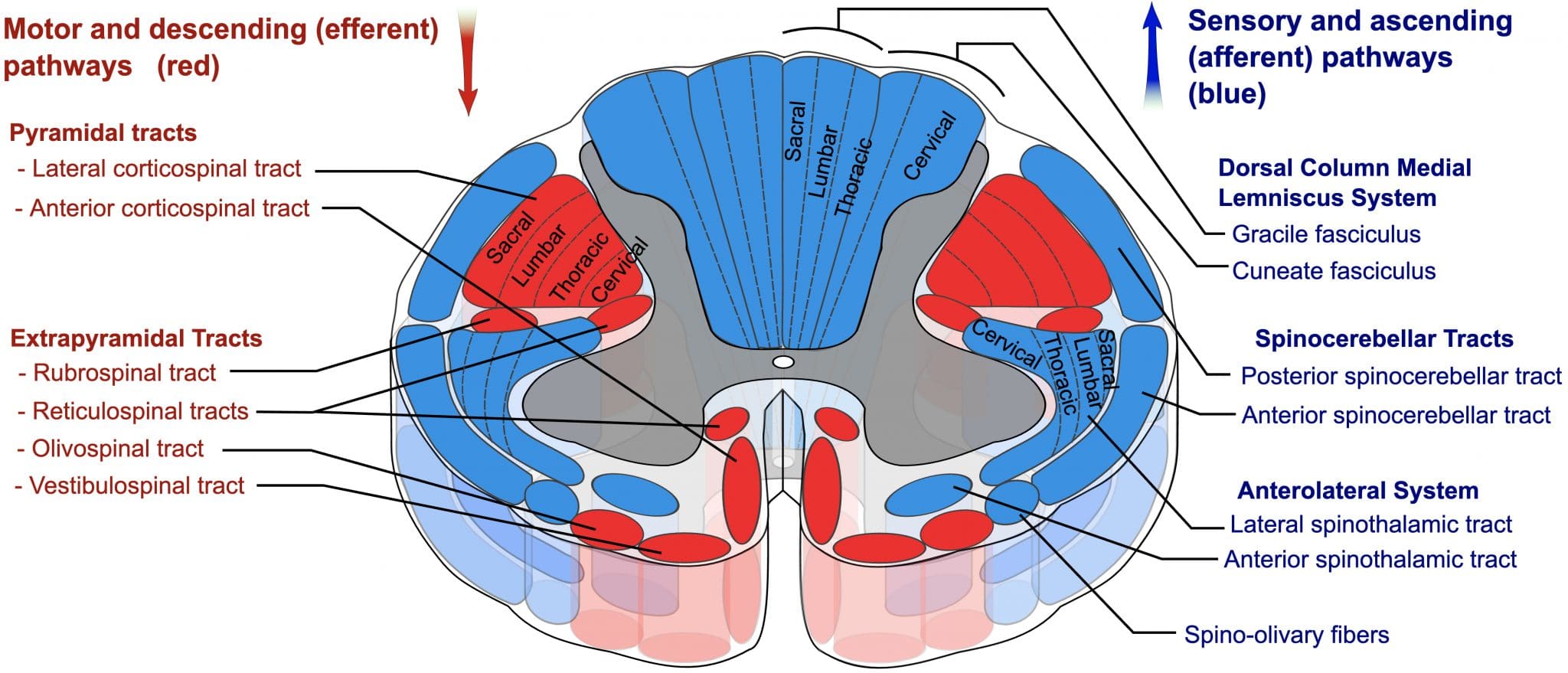
The spinal cord is like the highway for nerves; a streamlined structure that allows sensory and motor signals to communicate with both the brain and the body. There are certain lanes in this highway that transport different signals. These are:
- Dorsal column and the medial lemniscus
- Spinothalamic tracts
- Spinocerebellar tracts
Dorsal column-medial lemniscus (DCML)
The DCML pathway transports information about vibration, proprioception and fine touch. Information from these modalities is transported in the dorsal column, two large white matter tracts located between the dorsal grey horns of the spinal cord.
These dorsal columns are divided into two regions:
- Fasciculus gracilis (more medial): information from below T6-T8;
- Fasciculus cuneatus (more lateral): information from above T6-T8 but below the head.
The pathway of the DCML from the limb periphery to the brain is shown in table 1.
Table 1. Dorsal column-medial lemniscus pathway
| Order neuron | Nervous system structure | Ipsilateral | Contralateral |
| First-order neuron | Peripheral sensation | X | |
| Dorsal root | X | ||
| Dorsal horn of the spinal cord | X | ||
| Fasciculus gracilis or cuneatus (dorsal column) | X | ||
| Second-order neuron | Nucleus gracilis (NG) or cuneatus (NC) | X | |
| Medial lemniscus after NG and NC | X | ||
| Third-order neuron | Ventralposterolateral thalamus | X | |
| Thalamocortical tract | X | ||
| Somatosensory cortex | X |
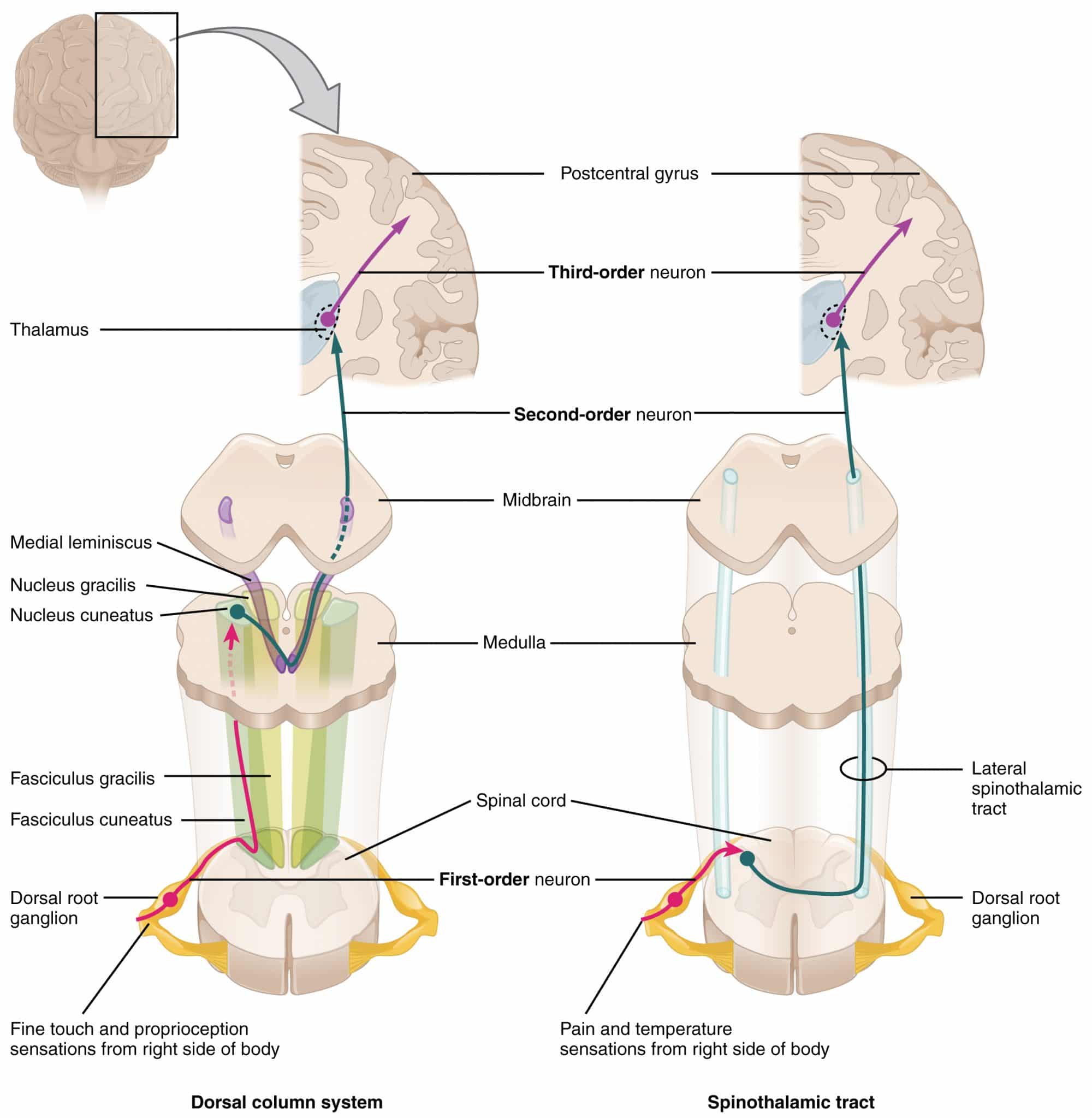
Spinothalamic tract (anterolateral system)
The spinothalamic tract has two components, often referred to collectively as the anterolateral system. They are the anterior and lateral spinothalamic tracts (STT):
- Anterior STT: crude touch and pressure
- Lateral STT: pain and temperature
The pathway of the spinothalamic tracts is shown in the table 2.
Table 2. The spinothalamic tract.
| Order neuron | Nervous system structure | Ipsilateral | Contralateral |
| First-order neuron | Peripheral sensation | X | |
| Dorsal root | X | ||
| Dorsal horn of the spinal cord | X | ||
| Second-order neuron | Substantia gelatinosa | X | |
| Anterior grey commissure | X* | X* | |
| Spinothalamic tracts | X | ||
| Third-order neuron | Ventralposterolateral thalamus | X | |
| Thalamocortical tract | X | ||
| Somatosensory cortex | X |
*The spinothalamic tract is special, and the nerve fibres cross at the anterior grey commissure at the level of the spinal nerve, but sometimes continue to cross in the 2-3 spinal levels superior
Spinocerebellar tracts
The spinocerebellar tracts transmit proprioceptive signals from the body to the brain. They transmit information about muscle stretch and the rate of muscle stretch from golgi tendon organs (GTO) and muscle spindle (MS) complexes. There are four of them:
- Dorsal (D) spinocerebellar: MS and some GTO from lower limb
- Cuneocerebellar (C): MS and some GTO from upper limb
- Ventral (V) spinocerebellar: GTO only from lower limb
- Rostral (R) spinocerebellar: GTO only from upper limb
There are three extra points to note with these pathways:
- The ventral spinocerebellar tract decussates twice, terminating in the IPSILATERAL cerebellum
- The other (spinocerebellar) tracts do not decussate and terminate in the IPSILATERAL cerebellum
- Each of these tracts can be group into the ventral spinocerebellar tract (ventral and rostral spinocerebellar tracts) and a dorsal spinocerebellar tract (cuneocerebellar and dorsal spinocerebellar tract)
The pathway of the spinocerebellar tracts is shown in table 3.
Table 3. The spinocerebellar tracts.
| Order neuron | Nervous system structure | Ipsilateral | Contralateral |
| First-order neuron | Peripheral sensation | DCVR | |
| Dorsal root | DCVR | ||
| Dorsal horn of spinal cord | DCVR | ||
| Second-order neuron | Spinocerebellar tract | DCR | V |
| Inferior cerebellar peduncle | DCR | ||
| Midbrain (level of inferior colliculus)* | V | ||
| Superior cerebellar peduncle* | V | V | |
| Third-order neuron | Cerebellum | DCVR |
*The midbrain and superior cerebellar peduncle are only involved in the ventral spinocerebellar tract; the cuneocerebellar, and dorsal and rostral spinocerebellar all enter the cerebellum at the medulla through the inferior cerebellar peduncle.
Clinical relevance: assessing the ascending tracts
Clinically, we assess two major sensory systems: the dorsal columns and the anterolateral system. On its own, the spinocerebellar system is rarely involved in pathology, and testing it clinically can be difficult.
The dorsal columns are assesed by:
- Vibration: 128 Hz tuning fork
- Joint propriocption: small-joint movement (thumb, big toe)
- Light touch: cotton wool
The spinothalamic tracts are assessed by:
- Pain: pin-prick
- Temperature: cool and warm metal object
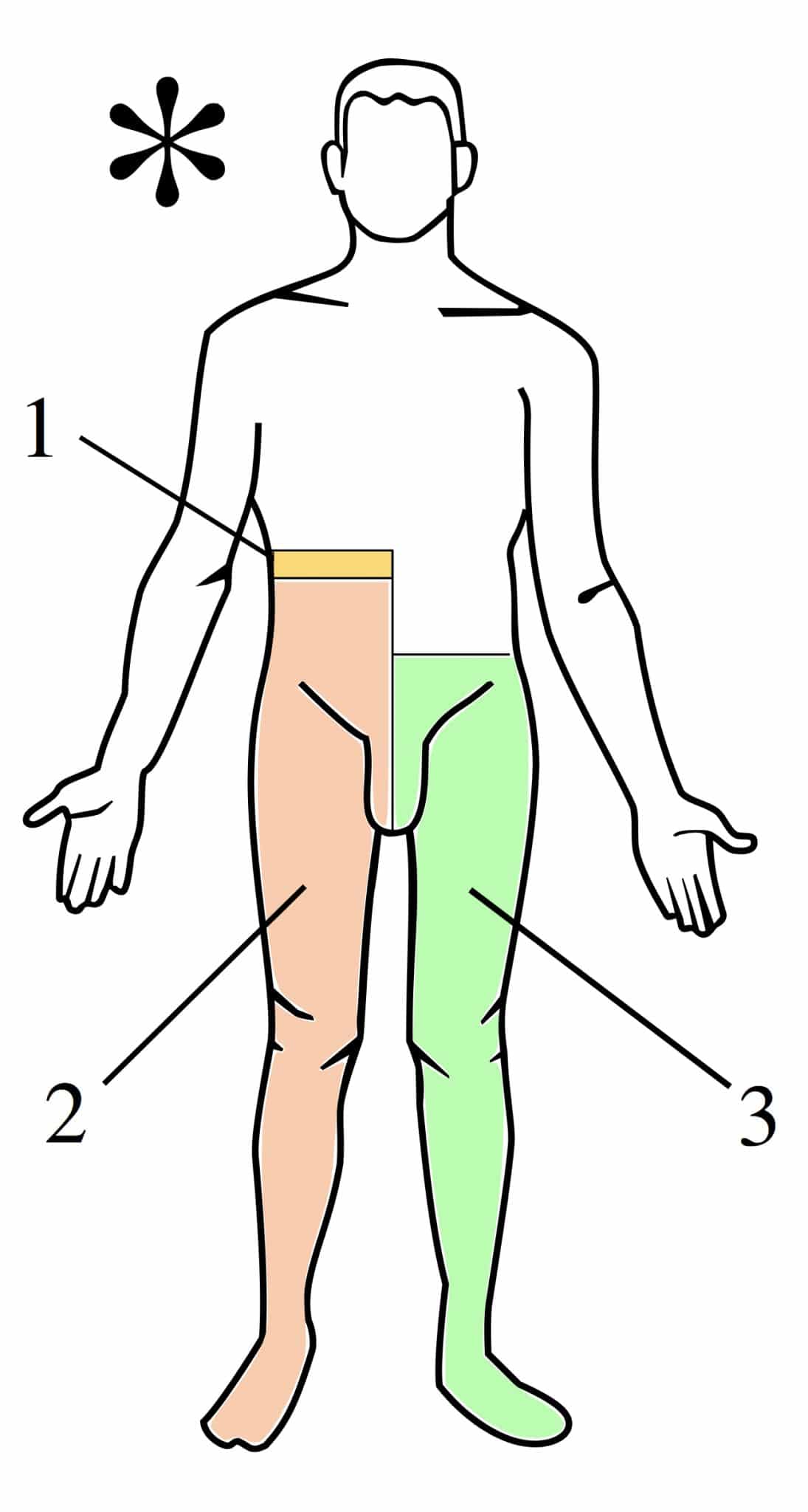
Clinical relevance: spinal cord syndromes
A hemitransection, also known as Brown-Sequard syndrome, is the severing of one half of the spinal cord.
Typically, this will be the result of trauma such as a knife wound, stroke or inflammatory diseases like multiple sclerosis or tuberculosis. It is a highly examinable topic pathology due to the level of understanding of anatomy needed.
Here, we will integrate what we know about decussation of the sensory and motor systems (covered in the descending tract article here) to correlate with a pathology severing the communication with the cerebral cortex.

Notice that all the tracts affected are ipsilateral except for the spinothalamic tract, which is the only tract to decussate at or near the level of the spinal nerve root.
In a right-sided hemitransection syndrome, there are right-sided (ipsilateral) corticospinal and dorsal column defects with a contralateral (left-sided) spinothalamic defect.
In terms of symptoms of a right hemitransection syndrome, there is right-sided paresis/paralysis and loss of vibration, proprioception and light touch; with a left-sided loss of pain and temperature.
These deficits can be tailored to a lesion occurring at any spinal level.
References
Reference texts
- Sinnatamby, C. S. (2011). Last’s Anatomy, International Edition: Regional and Applied. Elsevier Health Sciences.
- Moore, K. L., Dalley, A. F., & Agur, A. M. (2013). Clinically oriented anatomy. Lippincott Williams & Wilkins.
- Nolte, J. (2002). The human brain: an introduction to its functional anatomy.
- Snell, R. S. (2010). Clinical neuroanatomy. Lippincott Williams & Wilkins.
Reference images
- OpenStax College. License: [CC BY]
- Polarlys and Mikael Häggström. License: [CC BY-SA]
- Rhcastilhos. License: [CC BY-SA]
