

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Cranial nerve II, the optic nerve, controls the special sense of vision. As a direct extension of cerebral tissue, the retina is involved in the reception of photons and transmission of these light signals to the occipital cortex. These signals follow a complex pathway to get to the occipital cortex, we break this down into digestible pieces of information below, with a useful guide to clinical application.
Check out our summary of the cranial nerves here.
You can also check out our Cranial nerve anatomy quiz here.
The retina
Cranial nerve two is also known as the optic nerve. The optic nerve passes from the extracranial retina to the intracranial optic chiasm. The retina is a multi-layered cellular structure that receives light in the form of photons and converts this to an electrochemical action potential.
The layers of the retina are described in other articles, and the most important of these layers to know are the retinal ganglion cells.
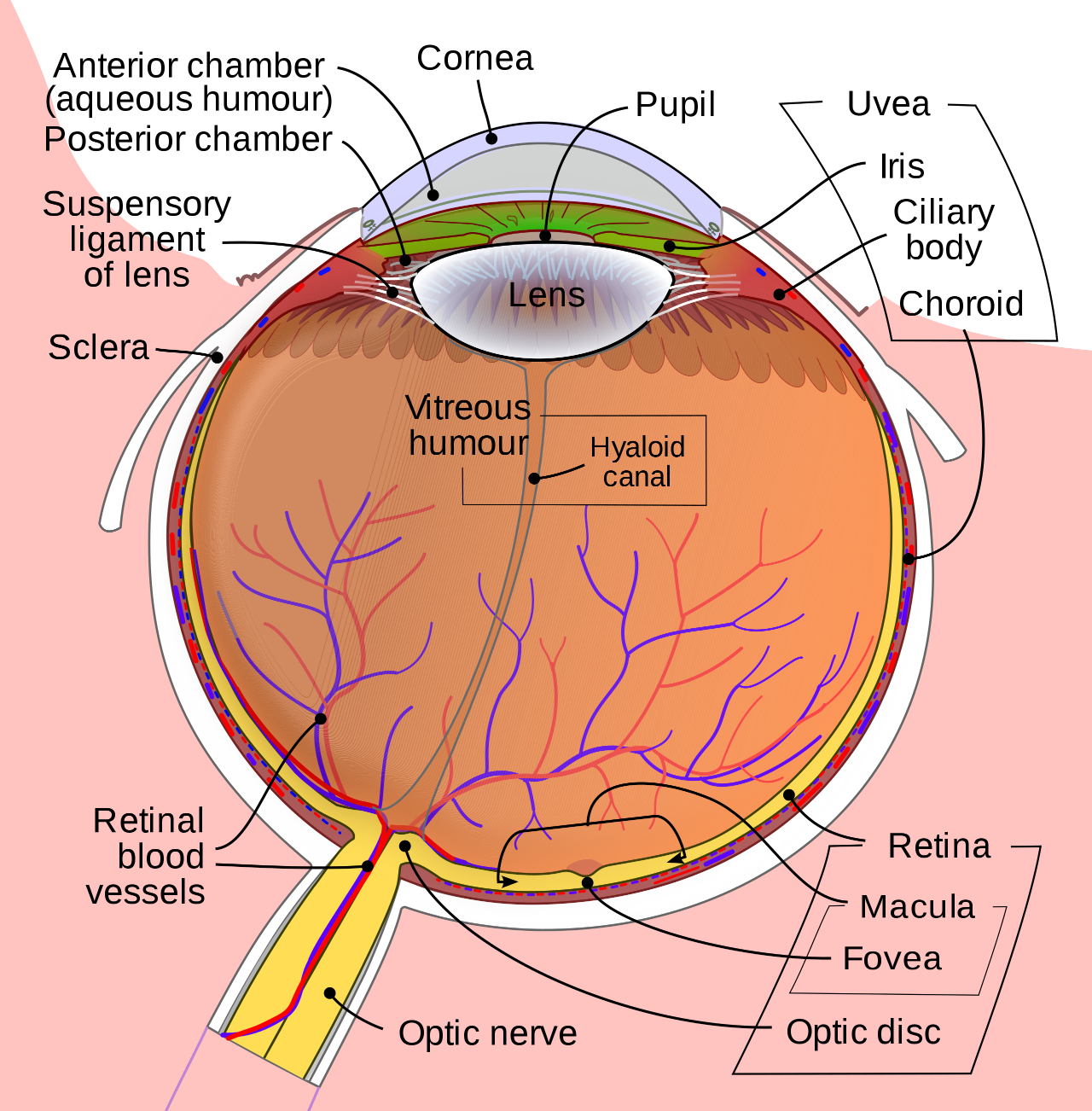
A retinal ganglion cell (RGC) is a type of neuron located near the inner surface (the ganglion cell layer) of the retina of the eye. It receives visual information from photoreceptors (e.g. rods and cones).
Rods are photoreceptors that distinguish between light and dark and are in higher densities in the peripheral retina. Cones are important for colour perception and are found in increasing and density closest to the fovea centralis. The fovea itself is almost entirely saturated with cones.
For simplicity, we will divide the retina in each eye into four fields (quadrants): superior left retinal field, superior right retinal field, inferior left retinal field and inferior right retinal field.
It is important to understand that these retinal fields all perceive the opposite visual field. That is, the left superior retinal field sees the right inferior visual field, and the right superior retinal field sees the left inferior visual field (Figure 3).

The optic nerve
As the light signal is received in rods and cones, an action potential is sent from each retinal ganglion cell to the convergence of all retinal neuron fibres at the optic disc.
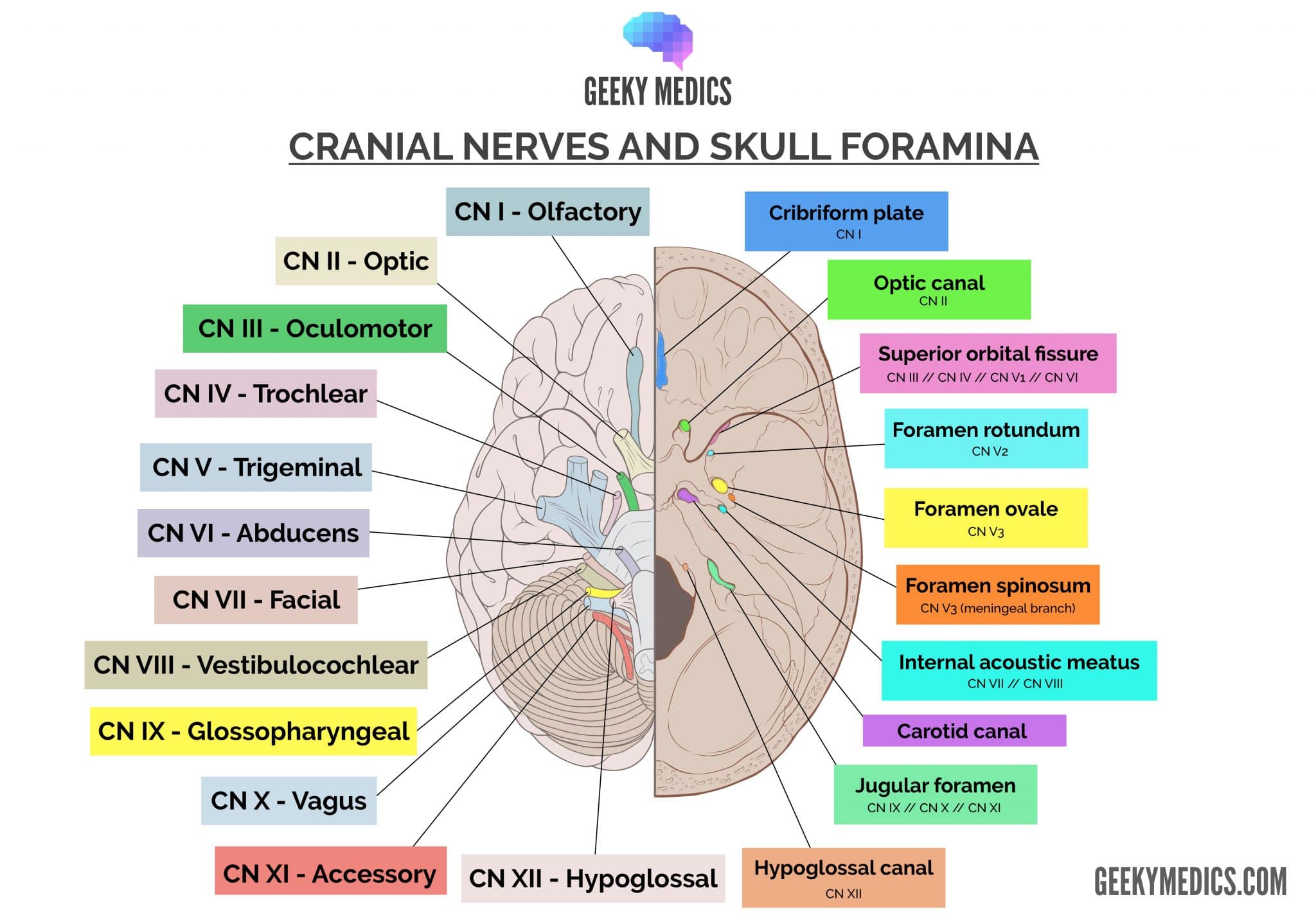
Upon exiting the retina through this disc, the fibres remain in a single bundle that we refer to as the optic nerve. This optic nerve travels posteromedially in the orbital cavity, passing through the optic canal in the sphenoid bone, and emerging in the middle cranial fossa.
The optic chiasm
The optic nerve lies above (not within) the cavernous sinus as it courses either side of the hypophyseal infundibulum (pituitary stalk). It is at this point that fibres begin to cross.
Fibres from the temporal (more lateral) retinal fields will always stay on the same side. Fibres from the nasal (more medial) retinal fields will always cross sides.
This process occurs so that immediately after the optic chiasm, the right optic tract will contain the right (superior and inferior) retinal fields of both eyes, and the left optic tract contains the left (superior and inferior) retinal fields for both eyes.
The optic tract
After the optic chiasm, the visual pathway continues as the optic tract. The optic tract passes around the thalamus to reach the dorsal thalamic nuclei known as the lateral geniculate nucleus (LGN).
The LGN then passes visual information to the primary visual cortex by the dorsal optic radiations. Some fibres will be sent back to the pre-tectal nuclei in the midbrain for integration as the afferent limb of the light reflex. This is discussed in more detail in the CN III article.
The dorsal optic radiations
The dorsal optic radiations are two fascicles of axons in each hemisphere. The first is known as the Baum loop or the superior dorsal optic radiation. The Baum loops transmit information from the superior retinal quadrants (responsible for the inferior visual fields).
The second loop is the Meyer loop or the inferior dorsal optic radiation. The Meyer loops transmit information from the inferior retinal quadrants (responsible for the superior visual fields).
The primary visual cortex
Both the superior and inferior dorsal optic radiations converge on either side of the brain at the calcarine sulcus of the occipital lobe, otherwise known as the primary visual cortex. The calcarine sulcus is a depression between gyri of the occipital lobe that projects anteriorly for 5cm from the occipital pole.
Information from the superior retinal fields is sent to the occipital cortex immediately superior to the calcarine sulcus. Information from the inferior retinal field is sent to the occipital cortex immediately inferior to the calcarine sulcus. Information from the periphery of the eye is sent more proximally on the calcarine sulcus. Information from the central retinal regions is encoded closer to the occipital pole.
Clinical relevance: pathology
The visual pathway follows a long course through the skull and brain, enduring several different vascular supplies. As such, pathologies at different parts of the visual pathway manifest as distinct clinical entities.

Clinical relevance: a systematic approach
When examining the eye, have a systematic approach to conditions such as reduced visual acuity. A reasonable way to approach this is to think of the structures that light must pass through on its way from outside the eye to the calcarine sulcus:
- Cornea: keratitis, corneal abrasions, foreign bodies
- Lens: cataracts
- Vitreous humour: glaucoma
- Retina: retinal detachment, retinitis pigmentosa
- Optic nerve: optic neuritis
- Optic chiasm: pituitary lesions
- Optic tract: strokes, tumours, vascular lesions (aneurysm, arteriovenous malformation)
- Lateral geniculate nucleus: strokes, tumours, vascular lesions
- Dorsal optic radiations: strokes, tumours, vascular lesions
- Occipital lobe: strokes, tumours, vascular lesions
While this may seem like an extensive list, it is a useful way to recall the structures of the visual pathway with clinically applicable pathologies.
Key points
- CN II is the optic nerve
- It provides special somatic afferent fibres for vision
- It connects to the brain (not the brainstem!)
- It is the afferent limb for the pupillary light reflex
- It passes through the optic canal of the skull
References
Reference texts
- Sinnatamby, C. S. (2011). Last’s Anatomy, International Edition: Regional and Applied. Elsevier Health Sciences.
- Moore, K. L., Dalley, A. F., & Agur, A. M. (2013). Clinically oriented anatomy. Lippincott Williams & Wilkins.
- Nolte, J. (2002). The human brain: an introduction to its functional anatomy.
- Snell, R. S. (2010). Clinical neuroanatomy. Lippincott Williams & Wilkins.
Reference images
- Patrick J. Lynch, medical illustrator. License: [CC BY]. Modified by Dr Lewis Potter.
- Rhcastilhos. And Jmarchn. Eye and retina. License: [CC BY-SA]
- Ratznium. Complete visual pathway. License: [CC BY-SA]
