

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
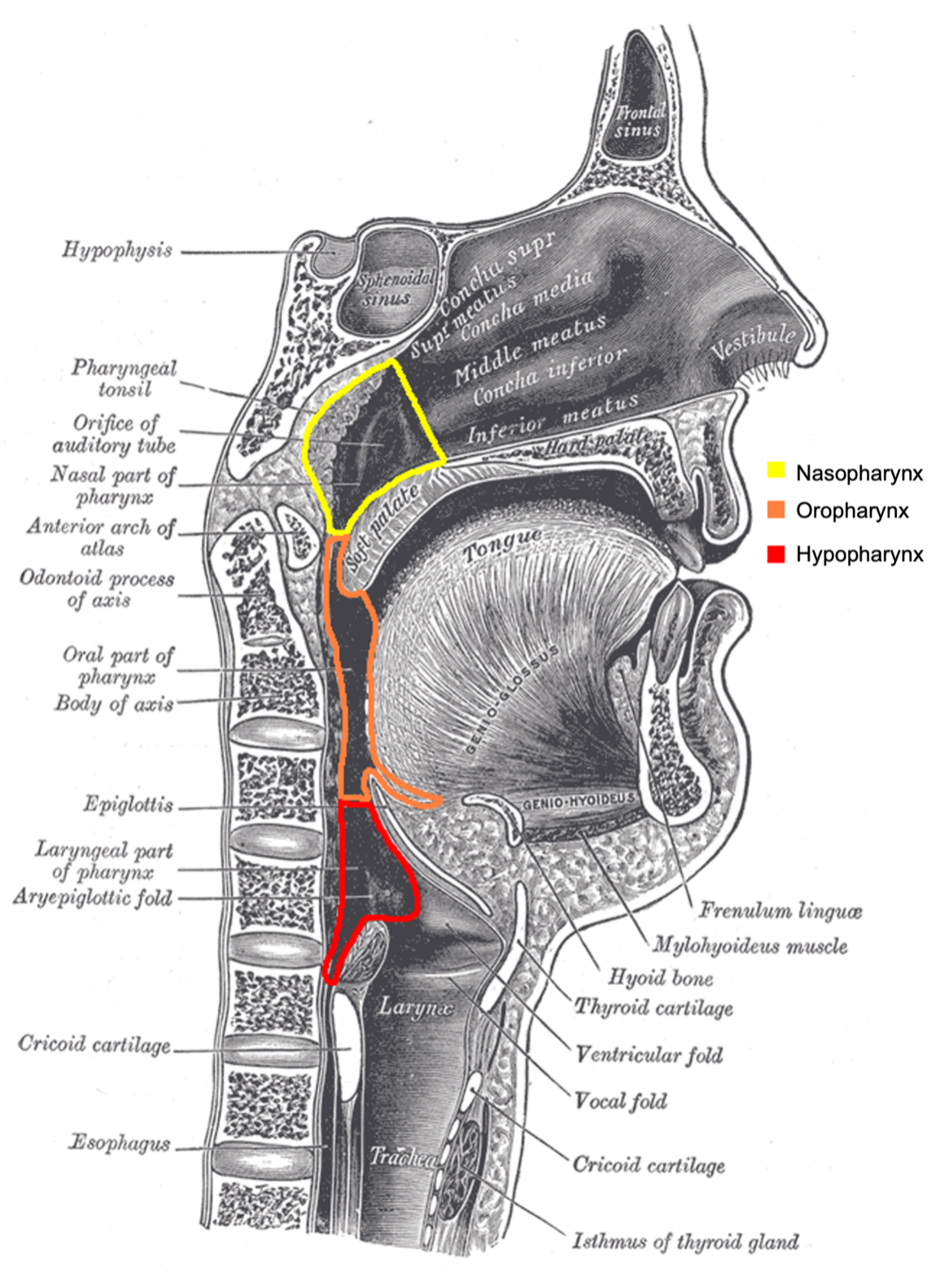
The pharynx extends from the skull base to the cricoid cartilage and can be divided into three parts: the nasopharynx, oropharynx, and laryngopharynx.
The pharynx is a cylindrical tube made up of skeletal muscle, fascia, and mucosa, that transports air to the laryngeal inlet and food to the digestive inlet.
This article will explore the three sections of the pharynx and highlight the anatomy, function, and clinical considerations.
Nasopharynx
Anatomy
The nasopharynx is the superior aspect of the pharynx. It is attached to the pharyngeal tubercle superiorly and mostly sits at the back of the nose, extending from the nasal cavity to the top of the soft palate. The nasopharynx is bound by the superior constrictor muscle.

Function
The function of the nasopharynx is to transmit air to the laryngeal inlet to aid breathing and speaking.
The musculature also aids in maintaining equilibrium and ventilation to the middle ear by opening and closing the eustachian tubes. Additionally, on swallowing the soft palate blocks the nasopharynx to prevent regurgitation of fluids and food upwards.
Clinical relevance
The nasopharynx is subject to diseases of inflammatory, infectious, and neoplastic nature. There are two main structures that are commonly affected within the nasopharynx, the pharyngeal tonsil and the eustachian tube openings.
Pharyngeal tonsil
The pharyngeal tonsils, or adenoids, are located in the roof and posterior wall of the nasopharynx. They are part of Waldeyer’s ring of lymphoid tissue and reach their largest size at 6-10 years of age, after which they typically get smaller.
This is the most common cause of nasal obstruction and sleep-disordered breathing in children. Children affected by this often experience symptoms of mouth breathing, snoring, apnoeic episodes, nasal discharge, ear pain and reduced hearing.
Management involves an adenoidectomy, where the excess tissue is scraped, cauterised or dissolved away. This removes the obstruction but there remains a small risk of regrowth of the lymphoid tissue and recurrence of symptoms.
Eustachian tube opening
The eustachian tube extends downwards and forwards from the middle ear along the medial pterygoid plate to the nasopharynx.
It works to drain, regulate the pressure, and oxygenate the middle ear. The distal opening of the eustachian tube opens into the nasopharynx.
Blockage of the eustachian tube can result in middle ear effusions and infections. In children, adenoid hypertrophy is the most common cause of eustachian tube obstruction and subsequent middle ear effusions. In adults, obstruction of the eustachian tube may be caused by nasopharyngeal carcinoma.
Oropharynx
Anatomy
The oropharynx continues inferiorly from the soft palate to the vallecula, at the base of the epiglottis. It contains many important structures including the base of the tongue, valleculae, epiglottis, palatine tonsils, tonsillar pillars, and uvula.
The oropharynx is largely bound by the middle constrictor. The oropharynx is partly innervated by the glossopharyngeal nerve (CN IX) which has connections with the middle ear via Jacobson’s nerve. This means often oropharyngeal pathology may result in ipsilateral referred otalgia.
Function
The oropharynx has two main functions: aiding swallowing and breathing. On swallowing, the food bolus is delivered to the oropharynx, where, on contact with the palatoglossal arches, results in a coordinated complex movement. The nasopharynx is sealed, and the tongue base applies pressure on the epiglottis to close the laryngeal inlet, which allows the food bolus to be delivered to the oesophagus in a safe manner.
Clinical relevance
The oropharynx is a common site of inflammatory, infectious, and neoplastic diseases. Unlike the other sub-sections of the pharynx, it is more exposed and therefore pathology can be more readily visualised.
Base of tongue
The base of the tongue can be the site of neoplasia and infection. It houses the lingual tonsil, which forms part of Waldeyer’s ring, which can be subject to hypertrophy or infection. The base of the tongue can be the site of neoplasia. As a sub-unit of the oropharynx, it is an important site to consider with symptoms of oropharyngeal cancer.
Vallecula
The vallecula is the groove at the base of the tongue just anterior to the epiglottis. Its function is to prevent saliva and debris from entering the laryngeal inlet. It is a common site of capture following foreign body ingestion.

Epiglottis
The epiglottis is a cartilaginous structure that sits anterior to the laryngeal inlet and closes the inlet to prevent aspiration of liquids or solids on swallowing.
Epiglottitis is a life-threatening condition that results in inflammation and swelling of the epiglottis and neighbouring structures. It is often caused by bacteria, namely Haemophilus influenza, and can result in airway obstruction.
Palatine tonsils
The palatine tonsils lie between the two tonsillar pillars. Like other structures of Waldeyer’s ring, they reach their greatest size at the age of 6-10 before regressing. Their size can be graded between 1-4, based on the space they occupy within the oropharynx.
Tonsillar hypertrophy can result in sleep-disordered breathing in children.
Infections of the tonsils (tonsillitis) are common and most commonly viral in nature. However, on occasion, they are bacterial in nature and require antibiotics. The Centor score has been developed to estimate the probability of streptococcal pharyngitis requiring antibiotics.
A complication of tonsillitis can be localised spread to the peritonsillar space where an abscess may accumulate. This often requires the administration of intravenous antibiotics and drainage. For more information, see the Geeky Medics guide to peritonsillar abscesses (Quinsy).
Chronic unilateral tonsillar swelling in an adult can be indicative of a neoplastic process and should be investigated.
Hypopharynx
Anatomy
The final part of the pharynx is the hypopharynx, or laryngopharynx, which extends inferiorly from the vallecula to the cricoid cartilage at level C6.
It is funnel-shaped and bound by the middle and inferior constrictor muscles.
Function
The hypopharynx continues the final stage of swallowing. As the food bolus is transported to the opening of the oesophagus, powerful contraction of the pharyngeal constrictor muscles pushes the bolus down toward the stomach.
Clinical relevance
The hypopharynx is a common site for pharyngeal cancers to occur. Patients often present with difficulty swallowing, pain, or referred ear pain. Hypopharyngeal cancers can be treated with chemotherapy, radiotherapy, or surgery.
A pharyngolaryngectomy is sometimes required to remove the tumour, which may result in a stoma being placed at the front of the neck with no communication to the oral or nasal cavity.
The hypopharynx can also be the site of persistent gastro-oesophageal reflux. This can result in symptoms of heartburn, chronic cough and voice changes.
Reviewer
Mr Daniel Schofield
ST6 ENT North London Trainee
Editor
Dr Chris Jefferies
References
- A, S. and A, A., 2021. Anatomy, Head and Neck, Ear Eustachian Tube. Available from: [LINK]
- Chen, R., Khorsandi, A., Shatzkes, D. and Holliday, R., 2009. The Radiology of Referred Otalgia. American Journal of Neuroradiology, 30(10), pp.1817-1823.
- DM, B. and H, S., 2021. Anatomy, Head and Neck, Laryngopharynx. Available from: [LINK]
- K, P., E, R. and D, P., 2021. Physiology, Swallowing. Available from: [LINK]
- KS, A. and RA, L., 2021. Anatomy, Head and Neck, Pharynx. Available from: [LINK]
- NL, M. and B, B., 2021. Anatomy, Head and Neck, Nasopharynx. Available from: [LINK]
Image references
- Figure 1. Henry Vandyke Carter. Sagittal section of nose, mouth, pharynx, and larynx. License: [Public domain]
- Figure 2. Henry Vandyke Carter. Lateral wall of the nasal cavity. License: [Public domain]
- Figure 3. Henry Vandyke Carter. The entrance to the larynx, viewed from behind. License: [Public domain]
