
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Cranial nerve IV is the trochlear nerve. The Latin ‘trochlear’ loosely translates to the modern English ‘pulley,’ named for the ligamentous sling that the muscles loops through before attaching to the globe.
The trochlear nerve only consists of motor fibres and is the only cranial nerve to exit the brainstem posteriorly. We describe the anatomical course of the trochlear through the skull, with consideration to its function and clinical relevance.
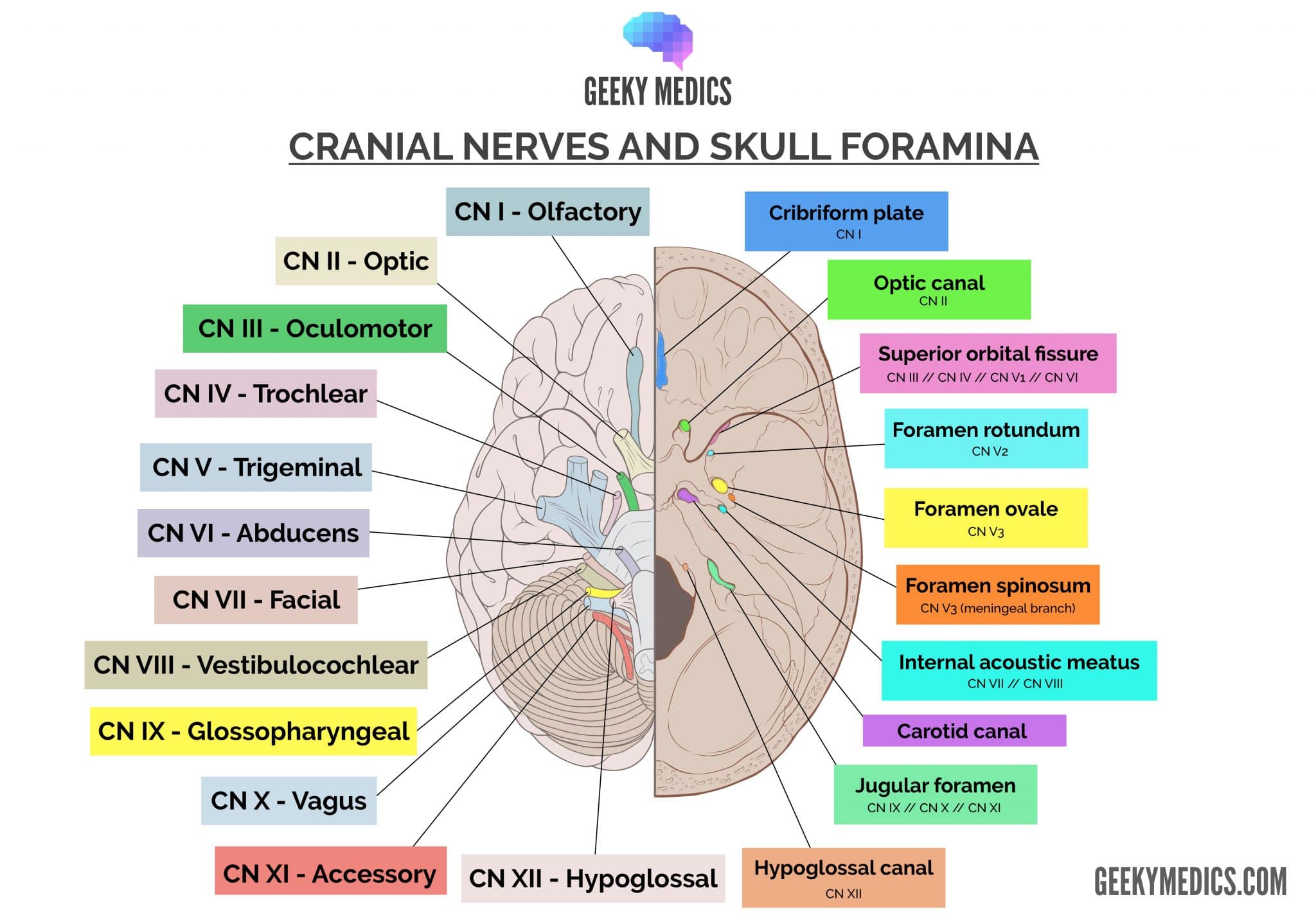
Check out our summary of the cranial nerves here.
You can also check out our cranial nerve anatomy quiz here.
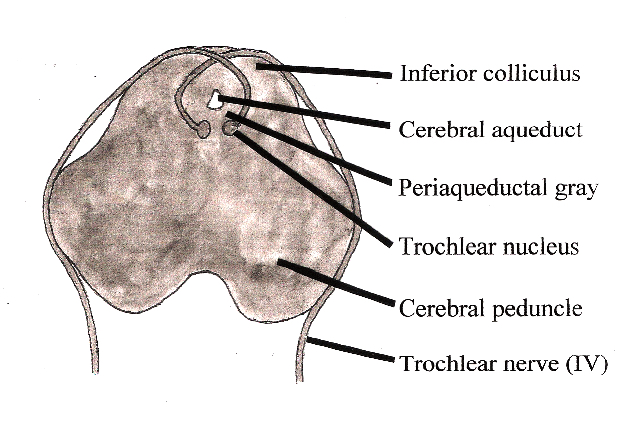
The trochlear nucleus
The trochlear nucleus is found immediately anterior to the cerebral aqueduct at the level of the inferior colliculus.
The trochlear nucleus contains somatic motor neuronal cell bodies that exit the nucleus posteriorly. With a slightly medial projection, the efferent motor fibres of the trochlear nerve cross over (decussate) and exit the brainstem just lateral to the inferior colliculi. This is important, as the left trochlear nucleus gives rise to the right trochlear nerve and vice versa.
The intracranial trochlear nerve
The trochlear nerve adheres close to the lateral surface of the midbrain as it passes within the subarachnoid space of the middle cranial fossa.
Upon reaching the posterior clinoid process of the sphenoid bone, the trochlear nerve pierces the dura mater and enters the cavernous sinus.
The trochlear nerve travels anteriorly in the lateral wall of the cavernous sinus before passing though the superior orbital fissure.
The extracranial trochlear nerve
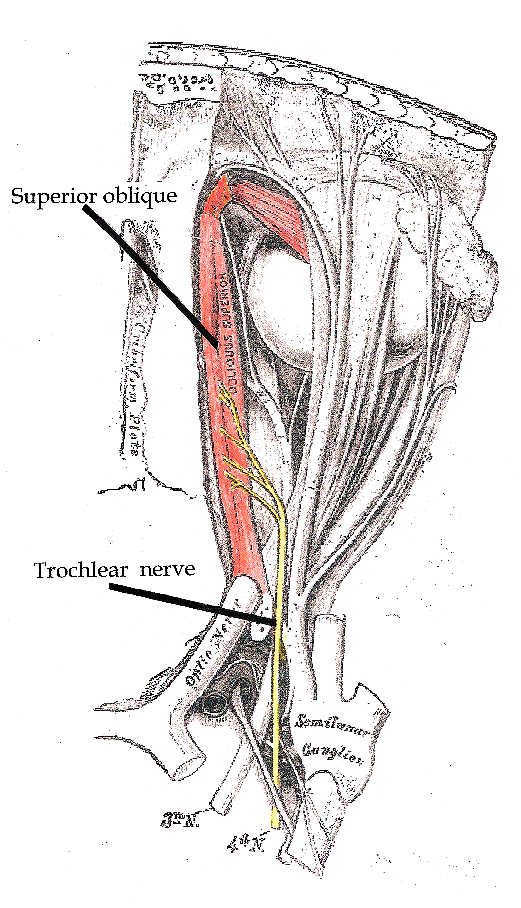
As the trochlear nerve moves through the superior orbital fissure, it moves medially within the orbital cavity to send motor fibres segmentally to the superior oblique extraocular muscle.
Attachments of the superior oblique muscle
The superior oblique muscle is the only structure innervated by the trochlear nerve.
The superior oblique muscle originates on the sphenoid bone at the orbital apex and runs adjacent to the sphenoid and then frontal bones as it approaches the trochlea (ligamentous pulley).
Passing through the trochlea, the superior oblique muscle turns postero-inferolaterally and inserts onto the supero-lateral aspect of the posterior quadrant of the globe.
Functions of the superior oblique muscle
The function of the superior oblique muscle is a confusing area. Due to the muscle’s insertion in the posterior half of the eye and its anterior fixation by the trochlea, it has three distinct roles:
- Abduction: when the muscle pulls toward the trochlea, it causes lateral deviation of the pupil and globe
- Depression: the trochlea is located superiorly to the insertion of the superior oblique muscle, and pulling on the postero-lateral quadrant causes the globe to turn down
- Intorsion: a combination of the abduction and depression movements is known as intorsion or medial rotation of the globe
Clinical relevance: examination
The superior oblique muscle is one of three extraocular muscles that are assessed with a moving target. The superior oblique muscle assists in abduction and depression of the eye, and these can be tested by drawing the letter ‘H’ in front of a patient with a fixed head.
Inability to abduct the eye manifests as horizontal diplopia, where the images are side-by-side. Inability to depress the eye manifests as vertical diplopia, where the one image lies atop the other.
A combination of these can lead to diagonal diplopia and may point to cranial nerve IV disease, narrowing your differential diagnosis.
Clinical relevance: pathology
Another way to examine the trochlear nerve is with the ‘Bielchowsky head tilt test.’ When a trochlear nerve palsy is suspected, the diplopia can be abolished by tilting the head toward the shoulder of the unaffected side.
Given the small size of the trochlear nerve, it is prone to injury from shearing forces seen in head trauma. Other causes of trochlear nerve injury are vascular injuries, diabetes mellitus, and transient viral infections causing a pseudo-Bell’s palsy phenomenon.
Key points
- CN IV is the trochlear nerve.
- It provides general somatic efferent to the extraocular superior oblique muscle.
- It assists in depressing and abducting the eye.
- It connects to the midbrain and is the only cranial nerve to leave the brainstem posteriorly.
- It passes through the superior orbital fissure of the skull.
References
Reference texts
- Sinnatamby, C. S. (2011). Last’s Anatomy, International Edition: Regional and Applied. Elsevier Health Sciences.
- Moore, K. L., Dalley, A. F., & Agur, A. M. (2013). Clinically oriented anatomy. Lippincott Williams & Wilkins.
- Nolte, J. (2002). The human brain: an introduction to its functional anatomy.
- Snell, R. S. (2010). Clinical neuroanatomy. Lippincott Williams & Wilkins.
References images
- Patrick J. Lynch, medical illustrator License: [CC BY]. Modified by Dr Lewis Potter.
- Btarski. License: [Public domain]
- Originally uploaded by Btarski (Transferred by Vojtech.dostal) License: [CC BY-SA]
