

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
The tongue is a muscular structure in the mouth covered by mucosa whose primary functions are in mastication, taste, and speech. It can be divided into the anterior two-thirds which makes up part of the oral cavity and the posterior-third, part of the oropharynx.1
The tongue consists of a tip, dorsal surface, ventral surface, and root. It is made up of four pairs of muscles:1
- Intrinsic (entirely within the tongue): superior longitudinal, inferior longitudinal, vertical, and transverse muscles. Their role is to change the shape of the tongue, having a role in facilitating speech, eating, and swallowing.
- Extrinsic (which have bony attachments): genioglossus, hyoglossus, styloglossus and palatoglossus. Their role is to alter the tongue’s position.
This article will focus on tongue embryology, origin, insertion, and action of the extrinsic muscles, followed by innervation, blood supply and lymphatic drainage of the tongue. Relevant clinical points will be explored and relevant diseases affecting the tongue explained.
Embryology
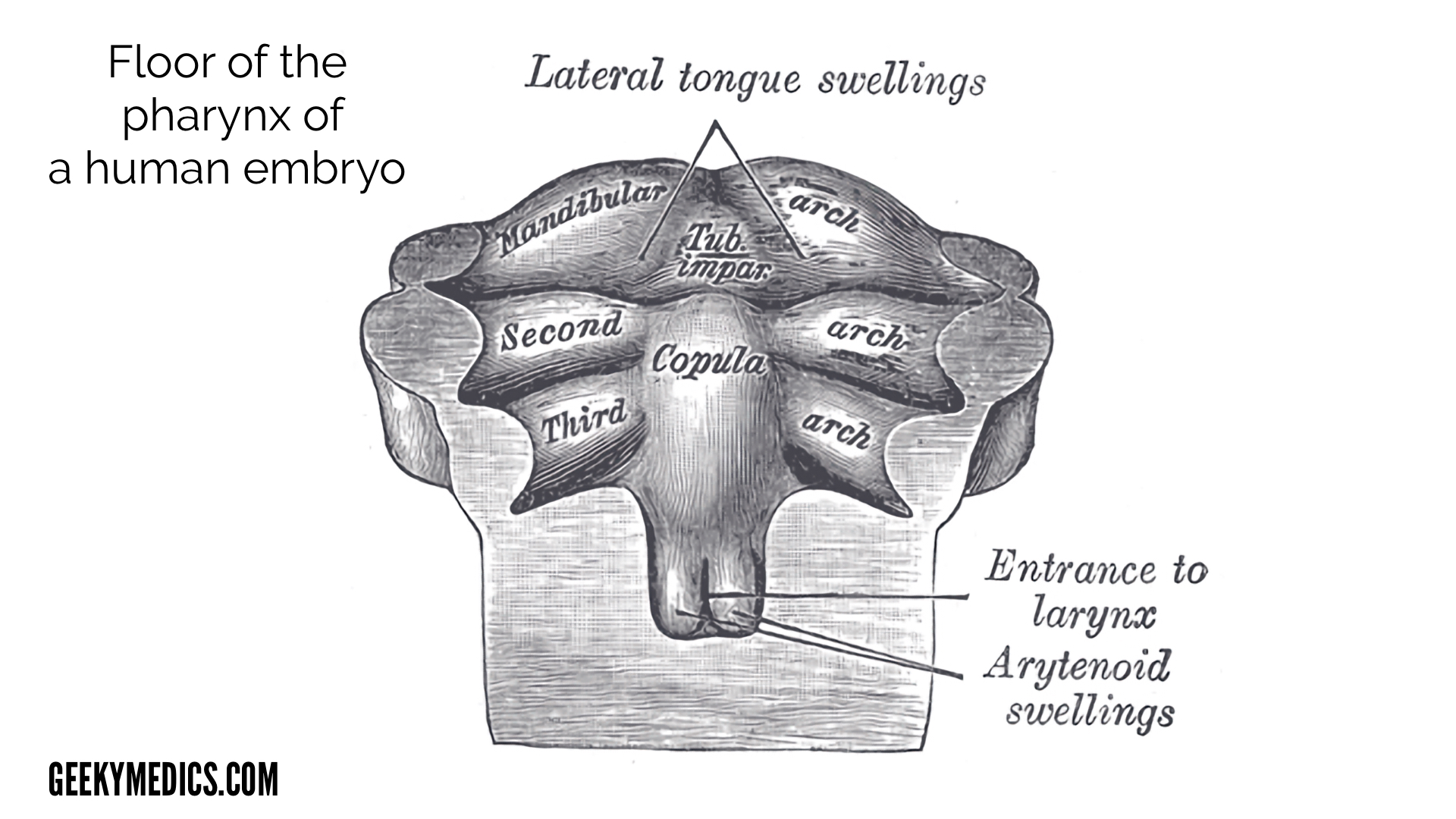
The tongue begins development in the fourth week of life from the median tongue bud or tuberculum impar (arising from the 1st pharyngeal arch). In week five, paired lateral lingual swellings begin to grow and cover the median tongue bud and fuse to form the anterior two-thirds of the tongue with the line of the fusion demarcated by the median sulcus. Around the lingual swellings, the cells degenerate to form a sulcus freeing the tongue from the floor of the mouth except in the midline where an attachment remains (midline lingual frenulum). The copula (which eventually becomes the posterior one-third) forms in the fourth week from the third and fourth pharyngeal arch and overgrows the second pharyngeal arch from week five. By week 8, the anterior two-thirds and posterior one-third fuse at a junction called the sulcus terminalis, an inverted V-shaped groove. At the tip of the sulcus terminalis lies the foramen caecum, a small pit-like depression which is the beginning of the thyroglossal duct. This forms the migration pathway of the thyroid gland into the neck.2
Clinical significance
Ankyloglossia (commonly called tongue-tie) is a condition where the median lingual frenulum forms a short attachment with the tongue and can restrict its movement to varying degrees. Though many are asymptomatic, this can lead to breastfeeding difficulties due to an inability to suck effectively, causing soreness for the mother and poor infant weight gain. In these cases, division of the tongue-tie can be carried out to alleviate symptoms.

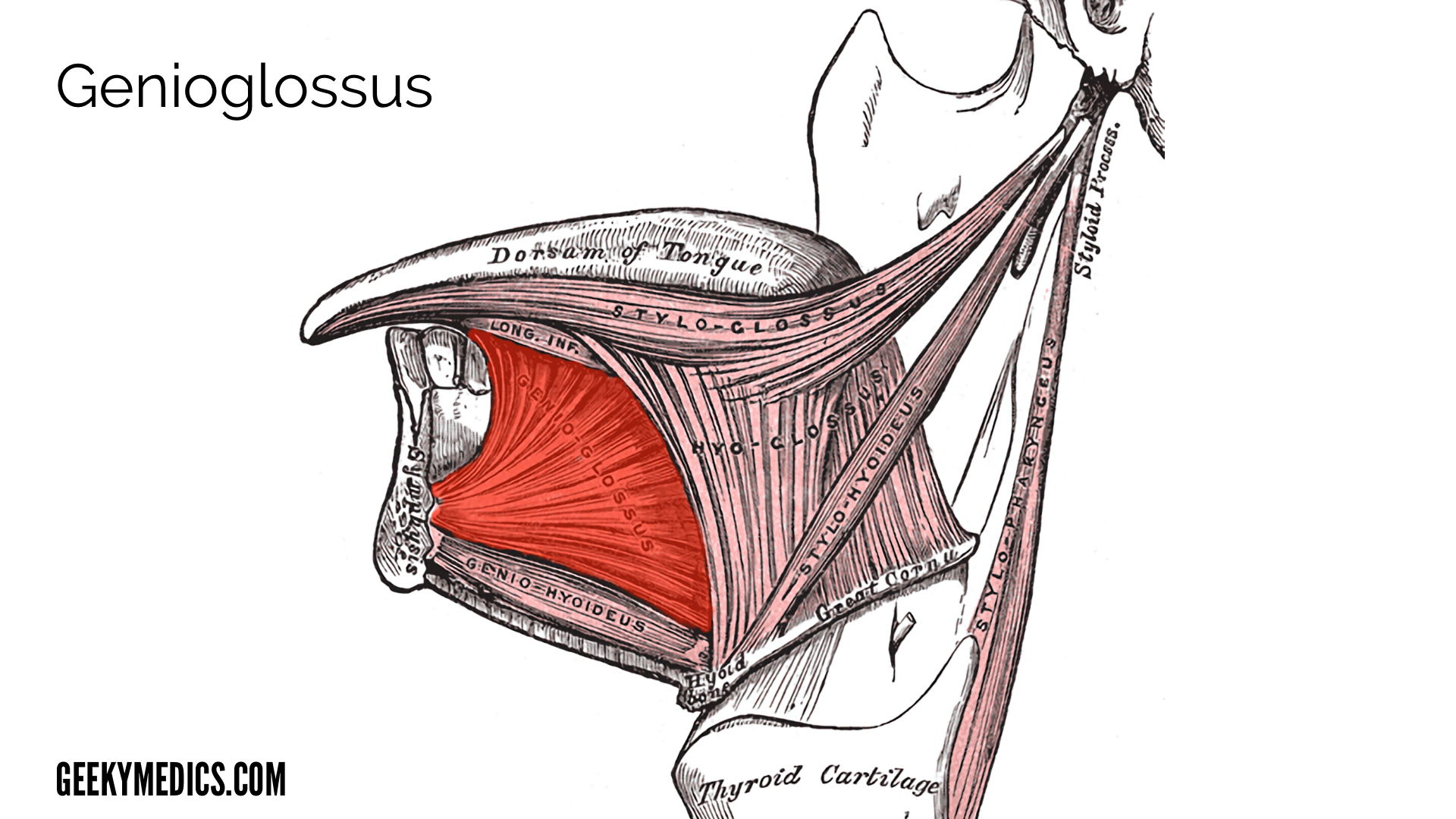
Genioglossus
Genioglossus is a fan-shaped muscle that accounts for most of the body of the tongue.
Origin
Superior genial tubercle (mental spine of the mandible).1
Insertion
Tongue mucosa, with the most inferior fibres inserting into the hyoid bone.1
Blood supply
Lingual artery and submental branches of the facial artery.
Action
The role of the genioglossus is primarily in tongue protrusion (inferior fibres) and deviation to one side. The middle fibres depress the centre of the tongue towards the back. The superior fibres draw the tip back and down.
Clinical significance
The genioglossus plays a major role in the maintenance of airway patency. Basic airway manoeuvres such as a chin lift (alongside a head tilt) and jaw thrust, aim to prevent the tongue (mainly genioglossus) from falling back in the oropharynx, via to its attachment to the mandible. Also, relaxation of this muscle during REM sleep is said to be responsible for obstructive sleep apnoea.6
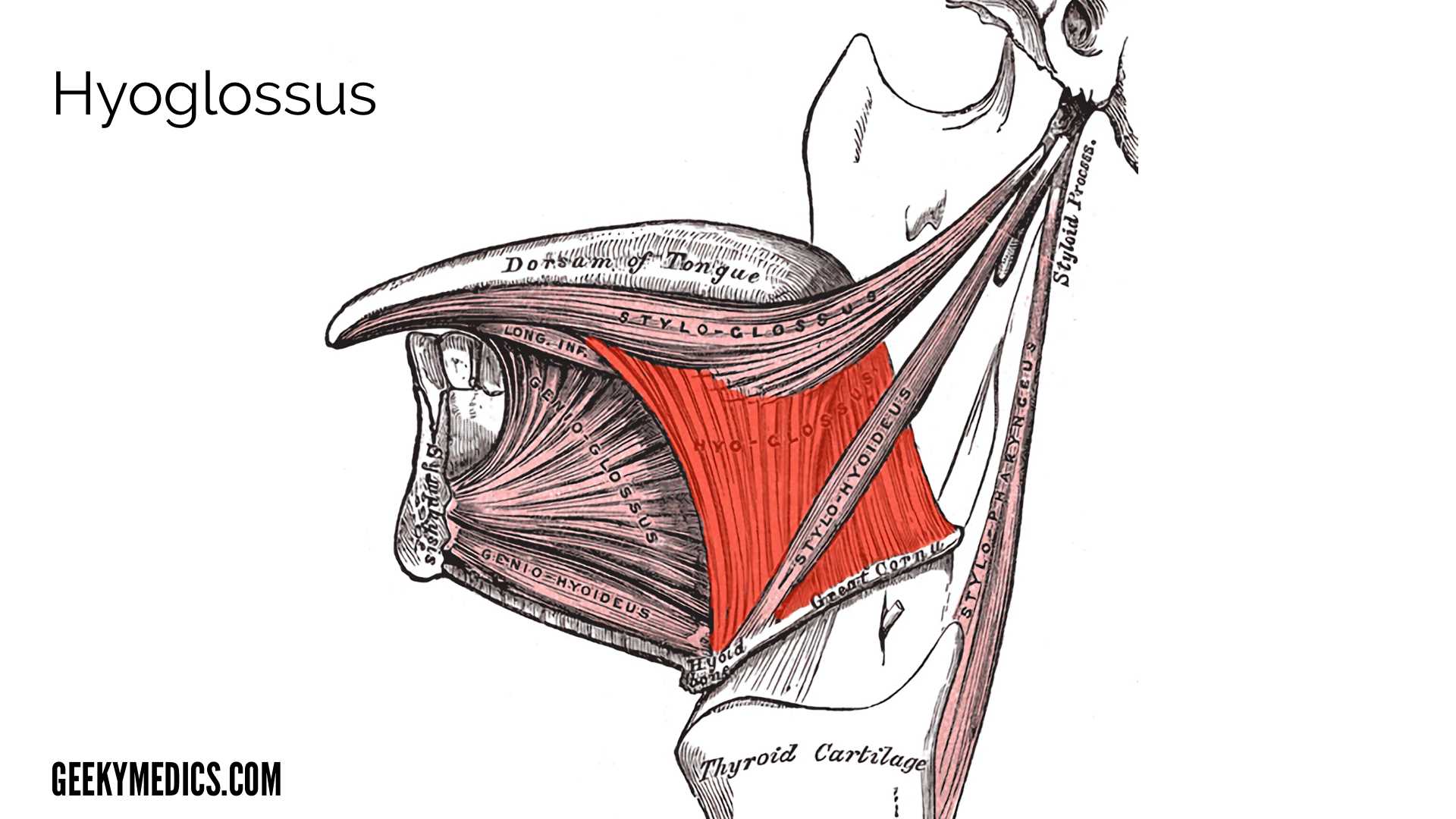
Hyoglossus
Hyoglossus is a thin, flat quadrilaterally shaped muscle in the upper neck and floor of the mouth.
Origin
Body and greater cornu of the hyoid bone.1
Insertion
Inferolateral aspect of the tongue between styloglossus laterally and inferior longitudinal muscle medially.1
Blood supply
Sublingual branch of the lingual artery and the submental branch of the facial artery.
Action
Depresses and retracts the tongue.
Clinical significance
Along with contributing to airway patency, it is an important landmark in the floor of the mouth for identifying important structures during submandibular gland and oral cancer surgery. In the sublingual space, the muscle separates the lingual artery (medial) from the lingual vein and submandibular duct (laterally).1
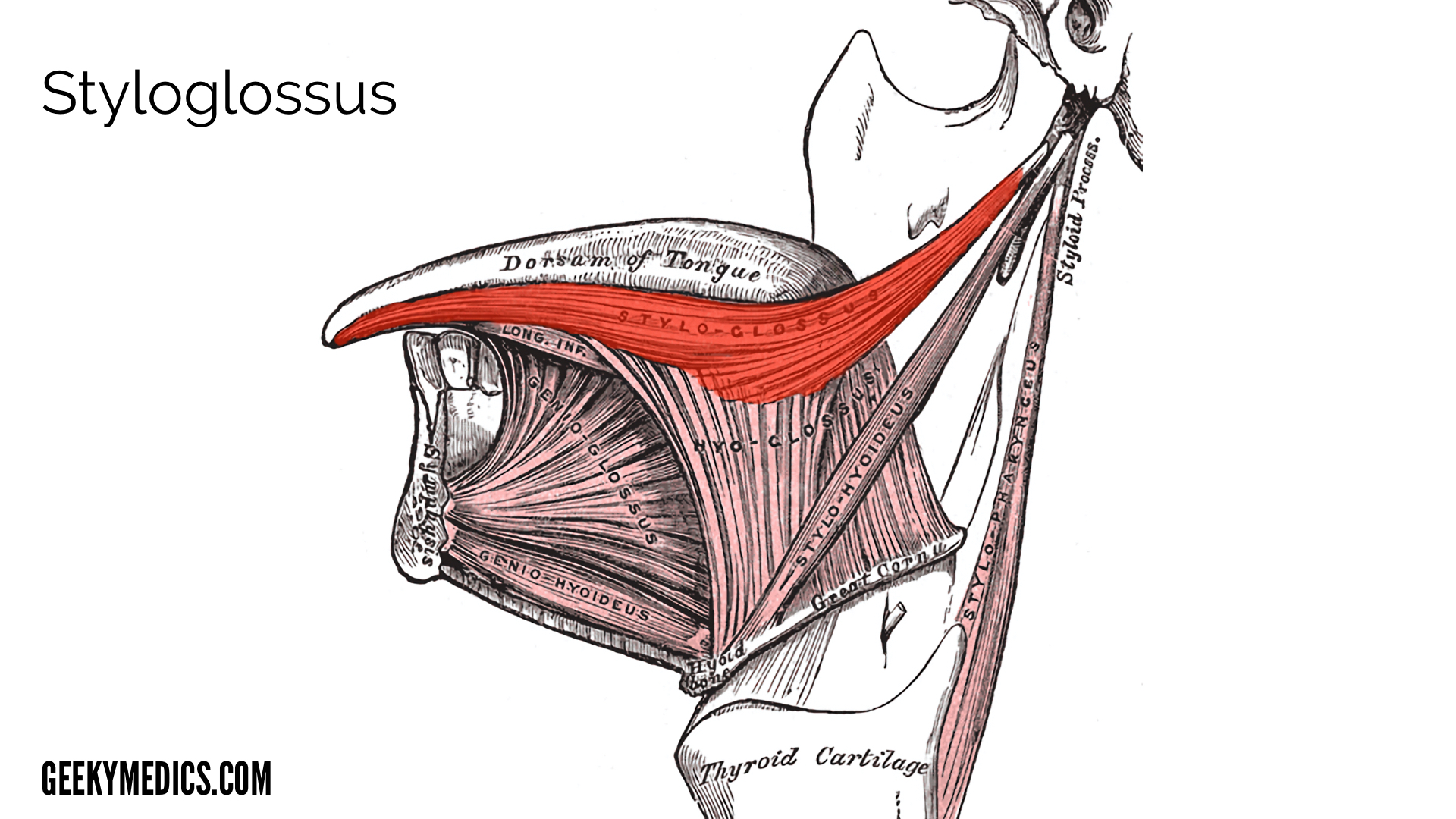
Styloglossus
A triangular muscle, which is the shortest and smallest of the three styloid muscles.
Origin
Anterolateral surface of the styloid process.1
Insertion
Passes forward to the postero-lateral surface of the tongue, blending with the inferior longitudinal and hyoglossus muscles.1
Action
Retracts and elevates the tongue, aiding initiation of swallowing.
Blood supply
Ascending pharyngeal artery.
Clinical significance
It is an important marker for staging squamous cell carcinoma (SCC) of the lateral oropharynx, with its involvement leading to a higher reclassification of tumours from T1-3 to T4a, ultimately affecting treatment options and surgical approaches for resection.1
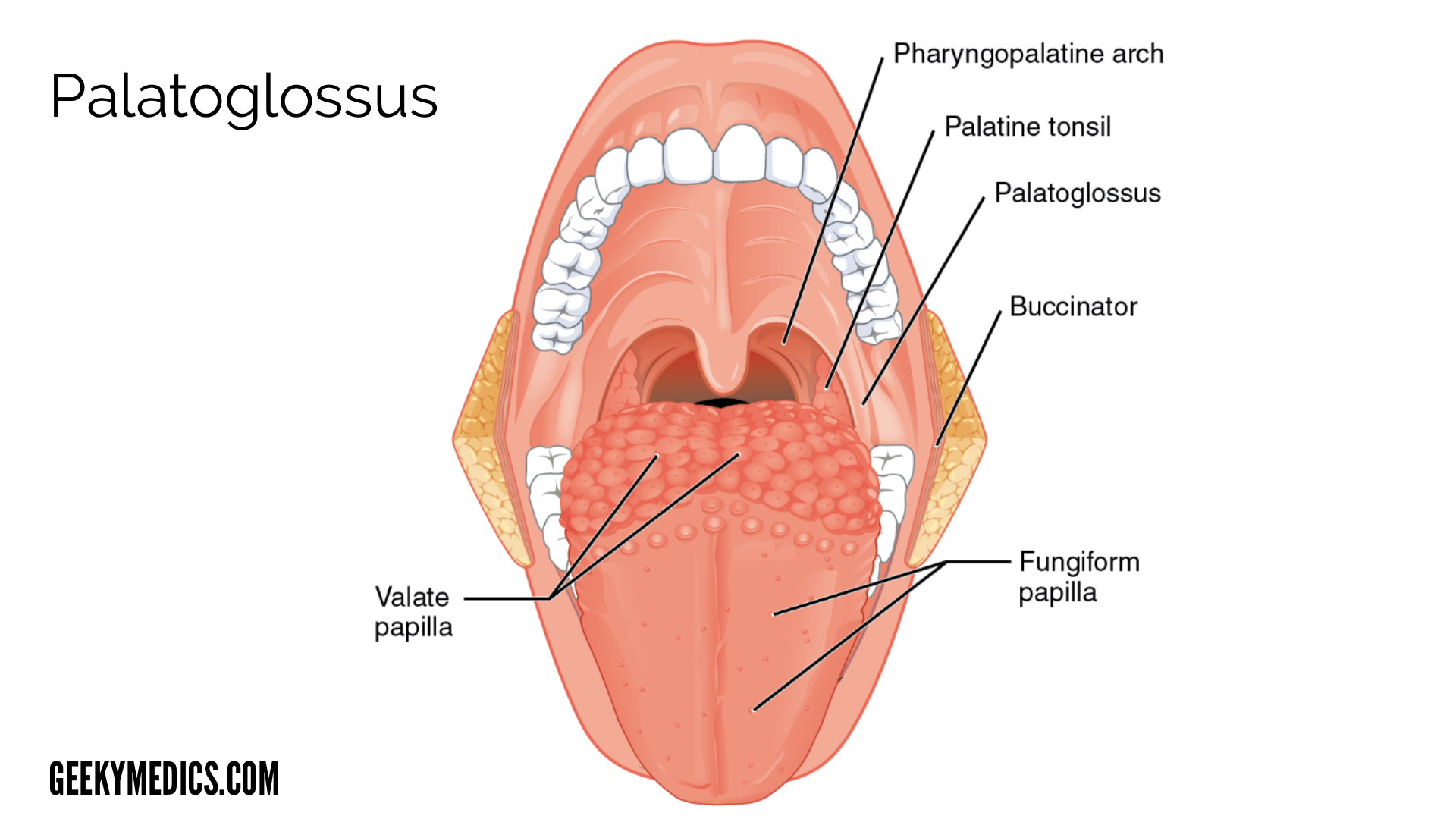
Palatoglossus
A thin muscle, narrower in the middle than its ends, that creates ridges in the lateral oropharyngeal wall, called the palatoglossal arch (or anterior faucial pillar). This marks the lateral border of the oral cavity and oropharynx.9
Origin
Inferior surface of the palatine aponeurosis.9
Insertion
Postero-lateral tongue and contributing to the palatoglossal arch.9
Blood supply
Lingual artery and collateral supply from the tonsillar artery (a branch of the facial artery).
Action
Elevates the posterior portion of the tongue and draws the soft palate inferiorly.
Clinical significance
The majority of tonsillar carcinomas originate from the anterior faucial pillar. Since the palatoglossus muscle makes up this structure it can provide a pathway for cancer to spread to the hard and soft palate.11
Lymphatic drainage of the tongue
The lymphatic drainage of the tongue is complex, consisting of superficial and deep networks. This can be simplified into the following:
- Anterior two-thirds of the tongue: initially into submental and submandibular nodes, which then empty into the deep cervical lymph nodes.
- Posterior one-third of the tongue: directly into the deep cervical nodes.
Clinical significance
Appreciation of the lymphatic drainage of the tongue into lymph node levels of the neck is important when understanding the metastatic spread of tongue malignancies. Bilateral drainage is common from central segments and ‘skip metastasis’ without the involvement of intervening levels can occur.1
Innervation of the tongue
The innervation of the tongue is divided into sensory and motor components.
Sensory supply
Sensory supply to the tongue involves several different nerves:
- Anterior two-thirds: Lingual nerve (a branch of the mandibular division of the trigeminal nerve – V3)
- Posterior one-third: Glossopharyngeal nerve (cranial nerve IX), plus a small branch of the internal laryngeal nerve (branch of the vagus nerve, cranial nerve X).
- Taste sensation is carried by special sensory nerve fibres of the chorda tympani (branch of the facial nerve). This nerve also carries secretomotor fibres to the submandibular and sublingual glands.1
Motor supply
All the intrinsic and extrinsic tongue muscles are supplied by the hypoglossal nerve (cranial nerve XII) EXCEPT the palatoglossus, which is supplied by the pharyngeal branch of the vagus nerve.
Clinical significance
Damage to the hypoglossal nerve can lead to weakness and atrophy of the ipsilateral tongue. When one of the two nerves are damaged the tongue when protruded will deviate towards the side of the damaged nerve, due to overaction the functioning genioglossus on the unaffected side.

Key points
- The tongue is a muscular organ of the oral cavity that has an important role in taste, swallowing, speech and can impact upon airway patency.
- It is made up of four paired extrinsic and intrinsic muscles, of which the latter determine tongue position.
- The muscles, neurovasculature and lymphatics of the tongue serve an important role in determining the spread of malignancy and surgical approach to head and neck pathology.
- Damage to the hypoglossal nerve leads to deviation towards the side of the lesion.
Reviewer
Mr Mark Singh
Consultant Oral and Maxillofacial Surgeon
References
- Brennan PA, Mahadevan V, Evans BT. Clinical Head and Neck Anatomy for Surgeons. London. CRC Press. 2016.
- Fehrenbach MJ, Popowics T. Illustrated Dental Embryology, Histology and Anatomy. 4th ed. Missouri. Elsevier Saunders. 2016.
- The floor of the pharynx of a human embryo of about the end of the fourth week. Adapted by Geeky Medics. Public domain. Available from: [LINK].
- Gzzz. Ankyloglossia. Adapted by Geeky Medics. Licence: CC BY-SA Available from: [LINK]
- Genioglossus. Adapted by Geeky Medics. Public domain. Available from: [LINK].
- Cori JM, O’Donoghue FJ, Jordan AS. Sleeping tongue: current perspectives of genioglossus control in healthy individuals and patients with obstructive sleep apnoea. Nat Sci Sleep. 2018; 10:169‐179. Published 2018 Jun 15. doi:10.2147/NSS.S143296.
- Hyoglossus. Adapted by Geeky Medics. Public domain. Available from:[LINK].
- Styloglossus. Adapted by Geeky Medics. Public domain. Available from: [LINK].
- Gray H. Anatomy of the Human Body. 20th New York. Bartleby. Published in 2000.
- OpenStax. Adapted by Geeky Medics. Licence: CC BY. Available from: [LINK].
- Rathee M, Jain P. Anatomy, Head and Neck, Palatoglossus Muscle (Glossopalatinus, Palatoglossal) [Updated 2019 Oct 15]. In: Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing; 2020 Jan-. Available from: [LINK].
- Mukherjee SK, Gowshami CB, Salam A, Kuddus R, Farazi MA, Baksh J. Adapted by Geeky Medics. Licence: CC BY. Available from: [LINK].
