

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
White patches of the oral mucosa are common and may represent a benign disorder (e.g. frictional keratosis), an oral potentially malignant disorder (e.g. leukoplakia), or malignancy (e.g. squamous cell carcinoma).1 Given the high-risk nature of some white patches, it is important to perform a thorough history and examination. A surgical sieve approach can then be used to classify the lesions, establish a differential diagnosis and decide on appropriate management. For those routinely examining the oral mucosa, such as dentists, referrals should be in accordance with local guidance, others should refer to specialist centres.
This article provides a brief overview of the clinical features and aetiology of white patches.
Clinical features
History
Alongside a thorough medical, social and dental history, key aspects to cover include:
- Presence of symptoms (e.g. oral discomfort, burning) – white patches are often asymptomatic.
- Previous history of white patches or oral biopsies (especially dysplasia).
- Recent antibiotic therapy (oral candidosis).
- Medication changes (oral lichenoid lesion).
- Recent dental treatment (oral lichenoid lesion, frictional keratosis).
- Any history of extra-oral changes (e.g. skin rashes, scalp lesions/hair loss and genital soreness may occur in conditions such as lichen planus, systemic lupus erythematosus and discoid lupus erythematosus).
Clinical examination
- The site, size and distribution of the white patches.
- Do the white patches wipe away? – suggests debris, mucosal sloughing or oral candidosis
- Is there any associated ulceration or mucosal redness? – lichen planus, speckled leukoplakia
- Is the overall appearance homogeneous? – uniform appearance, no differences in thickness, colour
- Is the overall appearance non-homogeneous? – non-homogenous white patches are considered higher risk lesions.
Traumatic
Frictional keratosis
Pathophysiology
- Chronic abrasion of the mucosa by dentures, or rough edges of teeth or restorations.
Site
- Buccal mucosa and the alveolar ridge in edentulous areas.
Appearance
- Variable from pale to densely white, smooth regions that merge gradually into surrounding normal mucosa.
Cheek/tongue biting
Pathophysiology
- Habitual biting of the cheek or tongue, triggering reactive areas of keratosis.
Site
- Buccal mucosa and lateral tongue along an occlusal plane.
Appearance
- Ragged tags of white, shredded mucosa with an uneven surface.
- Tongue scalloping may be concurrent.
Stomatitis nicotina
Pathophysiology
- Thermal trauma from heavy smoking/pipe use triggers inflammation of minor salivary glands with hyperkeratosis of the surrounding mucosa.
Site
- Hard palate
Appearance
- A diffuse white area across the palate, with small, raised red areas.
- May show ‘crazy paving’ appearance.2
Other
- Chemical burns (commonly caused by aspirin or clove oil used to treat toothache).
- Scars
- Skin grafts
Infective causes of white patches
Fungal
Oral candidal infection can cause white patches. The infection may be asymptomatic or may present with symptoms such as oral mucosal soreness or burning. Not all forms of oral candidosis cause white patches (the mucosa can be red with no obvious plaques of candida), but white patches may be a feature of the following three types.
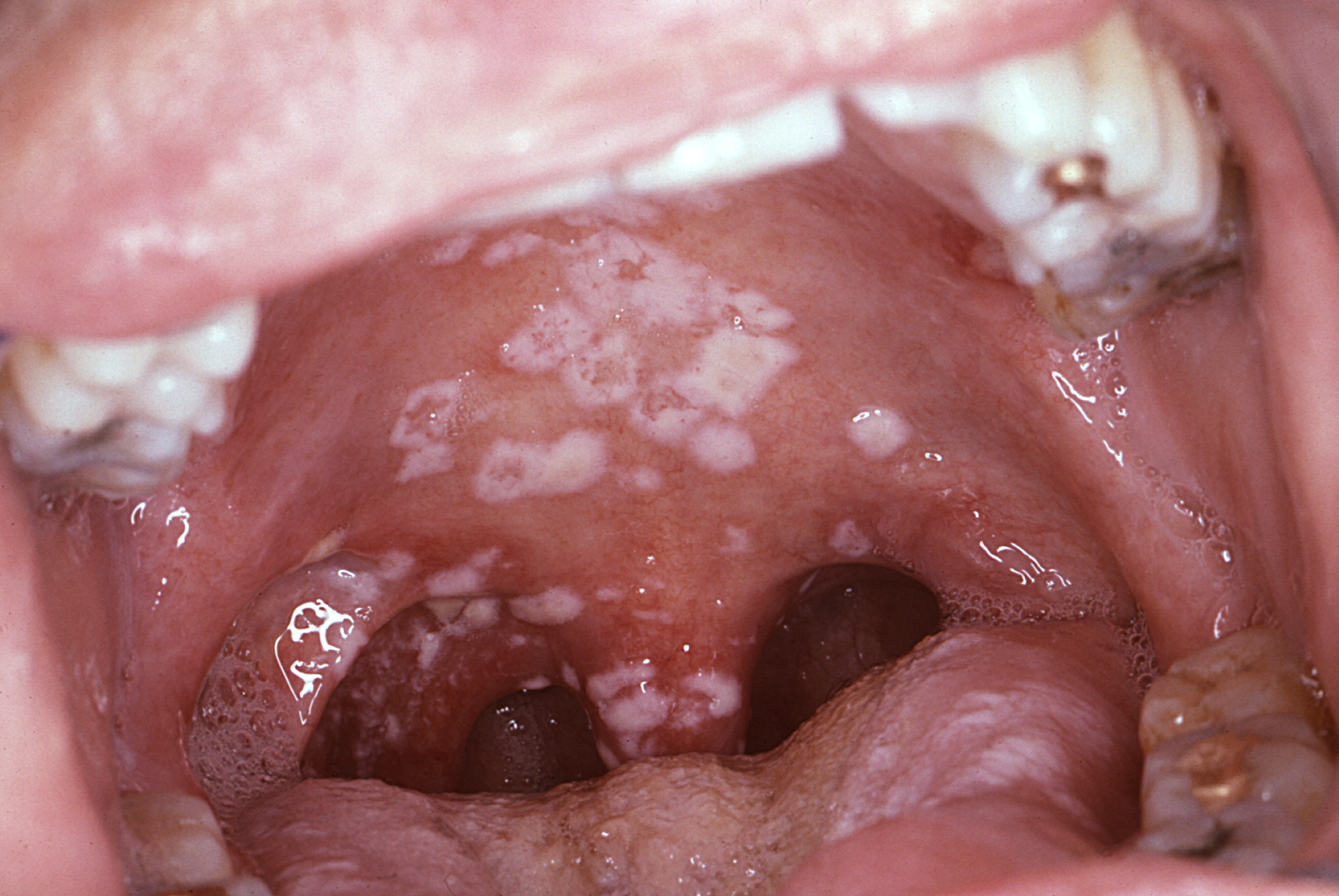
Acute pseudomembranous candidosis (thrush)
Pathophysiology:
- Opportunistic candidal colonisation of superficial mucosa in response to disturbance of the normal oral flora. This may be due to immunosuppressant drug use, following antibiotic therapy, or as a result of poor denture hygiene.
Site:
- Dorsal tongue
- Buccal mucosa
- Soft palate
Appearance:
- Soft white plaques which can be easily wiped off to reveal red underlying mucosa.
Chronic hyperplastic candidosis
Pathophysiology:
- Chronic low-level candidal infection induces keratosis; this is often classified as an oral potentially malignant disorder (i.e. over the long-term, malignant transformation may be observed).
Risk factor:
- Smoking
Site:
- Buccal commissures
- Dorsum of the tongue
Appearance:
- Well-defined, raised white plaques which may be speckled or nodular.
- Cannot be rubbed off.
Chronic mucocutaneous candidosis
Pathophysiology:
- Rare inherited condition characterised by increased susceptibility to candida infection. This results in recurrent or persistent oral and extra-oral candidal infections throughout life.
Site:
- Oral mucosa
- Skin
- Nails
Appearance:
- Extensive red and white patches throughout the mouth, often with ulceration.
- Cannot be rubbed off.
Oral hairy leukoplakia
Pathophysiology
- Epstein-Barr virus infection in immunosuppressed patients (e.g. immunosuppressive medication or late-stage or untreated HIV infection).
Site
- Lateral tongue
Appearance
- A painless, adherent, soft, white raised lesion with vertical corrugations.

Other
- Syphilis
- Papillomas
Neoplastic and potentially-malignant disorders
Leukoplakia
Definition
- ‘A white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer’.3
Pathophysiology
- Keratosis which is idiopathic in nature.
- The keratosis may or may not be dysplastic (showing disturbed growth patterns), with the epithelial cells demonstrating a ‘combination of architectural and cytological abnormalities… that indicate a risk of developing carcinoma’.2
- If dysplasia is present, it may be histologically defined as mild, moderate or severe.
- Generally affects adults over 50.
- Biopsy and histopathology is required to exclude all other clinical or pathological causes.4
Site
- May occur anywhere on the oral mucosa
- Sites considered ‘high risk’ of dysplastic changes include the ventrolateral tongue, floor of the mouth and retromolar region
Appearance
- Well-defined, tough, adherent white plaques usually with a wrinkled, uneven surface.
Oral submucous fibrosis
Pathophysiology
- Habitual use of paan with areca nut (paan) triggers fibroblast proliferation and collagen synthesis, causing fibrosis of oral mucosa.
Site
- Buccal or labial mucosa or soft palate.
Appearance
- Pale, hard mucosa with palpable fibrous bands. May be accompanied by limited mouth opening and dark brown stained teeth.
Smoker’s keratosis
Pathophysiology
- Chronic irritation caused by heavy smoking triggers diffuse hyperkeratosis. Long-standing lesions may show dysplasia.
Site
- Generalised across the oral mucosa.
Appearance
- Generalised whitish discolouration of the oral mucosa. Margins are not sharply defined.
- Smokeless tobacco use (less common in the UK) causes discrete, whitish thickenings of the oral mucosa which may be wrinkled. These lesions are localised to the area where the tobacco is held (usually buccal sulcus).
Other
- Carcinoma (usually oral squamous cell carcinoma)
Normal variants
Fordyce spots
Pathophysiology
- Normal anatomical variant where sebaceous glands are present in the oral mucosa.
Site
- Labial mucosa of the upper lip
- Buccal mucosa
Appearance
- 1-2 mm creamy-yellow, raised papules
- Tend to occur in clusters
Leukoedema
Pathophysiology
- A variant of normal anatomy, with thickening of the parakeratin layer in the superficial epithelium.
- Particularly affects those of African heritage.
Site
- Bilateral buccal mucosa.
Appearance
- Diffuse, greyish-white discolouration which disappears if the mucosa is stretched.
Inherited dyskeratoses
White sponge naevus
Pathophysiology
- Rare autosomal dominant developmental anomaly
- Mutation in genes coding keratin
Site
- Non-keratinised mucosa (especially buccal mucosa)
- Can affect other body sites such as the vagina (Cannon’s disease)
Appearance
- Thickened, folded, soft white patches which fade into normal mucosa.
Other
- Dyskeratosis congenita
- Darier’s disease
- Tylosis
Immune-mediated
Lichen planus
Pathophysiology
- An immune-mediated chronic inflammatory condition, with T cell infiltration and destruction of the basal layer with responsive hyperkeratosis.
Risk factors
- Slight female predisposition
- Age range 30-65
Site
- Buccal and gingival mucosa
- Tongue
Appearance
- Bilateral and symmetrical
- Variable appearance and symptoms depending on whether the patient is in the destructive or reparative phase of the disease.
- Can categorise into several presentations: reticular, atrophic, ulcerative, plaque-type, desquamative gingivitis, bullous and vulvovaginal-gingival
- Patients may have concurrent skin lesions (purple, polygonal, pruritic papules)

Oral lichenoid lesion
Pathophysiology
Identical to lichen planus but triggered by a causative agent.
Causative agents include:
- Local amalgam/gold filling
- Medication (including antihypertensives, oral hypoglycaemics and anti-malarial medication)
- Graft-versus-host disease
- Hepatitis C infection
Site
- Buccal and gingival mucosa
- Tongue
Appearance
- Variable appearance as with lichen planus.
- If local cause may see discrete area adjacent to restoration.
Systemic lupus erythematosus(SLE)/discoid lupus erythematosus(DLE)
Pathophysiology
- Auto-immune connective tissue disease where the body produces autoantibodies against double-stranded DNA, triggering inflammation.
Risk factors
- Female sex
- Asian or African heritage
Site
- Soft and hard palate
- Buccal mucosa
- Gingival mucosa
- Tongue
Appearance
- In SLE, lesions appear similar to lichen planus (see above).
- Discrete red and white areas (sometimes with associated ulcers).
- In DLE lesions are often unilateral with central erythema and radiating white striae – ‘sun-ray’ appearance.
A general approach to management
For all new white patches that are not easily explained by trauma or normal anatomical variation, management should begin with a prompt referral for a specialist opinion.5
The majority of patients will undergo a biopsy to assist in attaining a definitive diagnosis.
Further management steps are outlined below.
Primary care
- Habit cessation and patient education (smoker’s keratosis, leukoplakia)
- Replacement of fillings/denture if required (oral lichenoid lesion, frictional keratosis)
- Treatment of acute infections e.g. acute pseudomembranous candidosis
- Appropriate referral
- Regular monitoring of the oral mucosa
Secondary care
Management will be guided by the specific condition, but treatment may include:
- Topical corticosteroids (lichen planus, SLE, DLE)
- Immunomodulating or immunosuppressant drugs (lichen planus, SLE, DLE)
- Topical or systemic antifungals (oral candidosis)
- Removal of the lesion by surgical or laser excision (moderate-severe dysplasia/oral squamous cell carcinoma)
- Ongoing monitoring of the oral mucosa
Reviewers
Shalini Nayee
Registrar in Oral Medicine, Guy’s and St Thomas’ NHS Foundation Trust
Martyn Ormond
Specialty Doctor in Oral Medicine, Guy’s and St Thomas’ NHS Foundation Trust
References
- Felix, D H, Luker, J and Scully, C 2013, ‘Oral Medicine: 6. White Lesions’, Dental Update, vol. 40, no. 2, pp. 146-154
- Odell, E W 2017, Cawson’s Essentials of Oral Pathology and Oral Medicine (Ninth Edition), Elsevier, Amsterdam
- Warnakulasuriya, S, Johnson, N W and Van Der Waal, I (2007) ‘Nomenclature and classification of potentially malignant disorders of the oral mucosa’, Journal of Oral Pathology & Medicine, vol. 36, no 10 pp. 575-580
- Mortazavi, H, Safi, Y, Baharvand, M, Jafari, S, Anbari, F and Rahmani, S 2019, ‘Oral White Lesions: An Updated Clinical Diagnostic Decision Tree’, Dentistry Journal, vol. 7, no. 1, pp. 15-39
- Holland, I 2010, ‘Management of White Patches’, Dental Update, vol. 37, no. 8, pp. 526-531
- Sol Silverman, Jr./CDC. Secondary oral pseudomembranous candidiasis. [public domain] [LINK]
- Sol Silverman, Jr./CDC. Oral hairy leukoplakia. [public domain] [LINK]
- Robert E. Sumpter/CDC. Lichen planus. [public domain] [LINK]
