
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
The ability to write in a patient’s notes effectively is an essential skill all medical students need to learn. Accurate documentation is also incredibly important from a medicolegal perspective. This guide provides an overview of how to write in a patient’s notes and should hopefully make you feel a little more prepared when you have your first attempt on the ward.
The basics
Ok, so a blank continuation sheet has been thrust towards you and you’ve been asked to document something – let’s remind ourselves of the basics of documentation.
What should I use to write with?
You need to use a pen with black ink, as this is the most legible if notes are photocopied.
Patient details
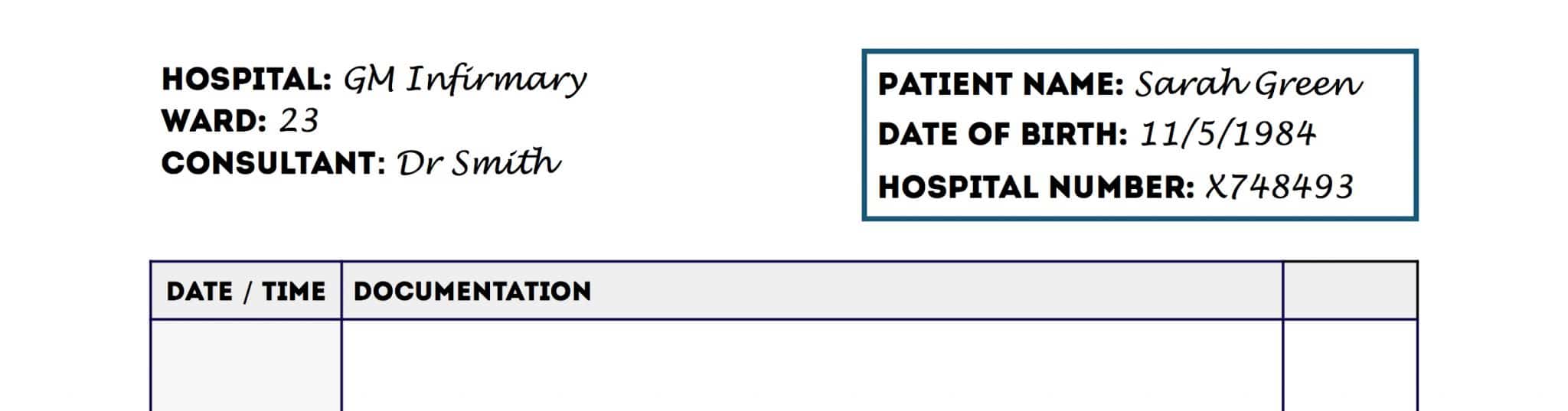
For every new sheet of paper your first task should be to document at least three key identifiers for the relevant patient:
- Full name
- Date of birth
- Unique patient identifier
- Home address
If a patient label containing at least three identifiers is available, then this can be used instead of writing out the information manually.
Location details
You should indicate the patient’s current location on the continuation sheet:
- Hospital
- Ward
Making a new entry in the notes
At this point, you should already be holding a pen with black ink and you should have ensured the continuation sheet has at least three key patient identifiers at the top.
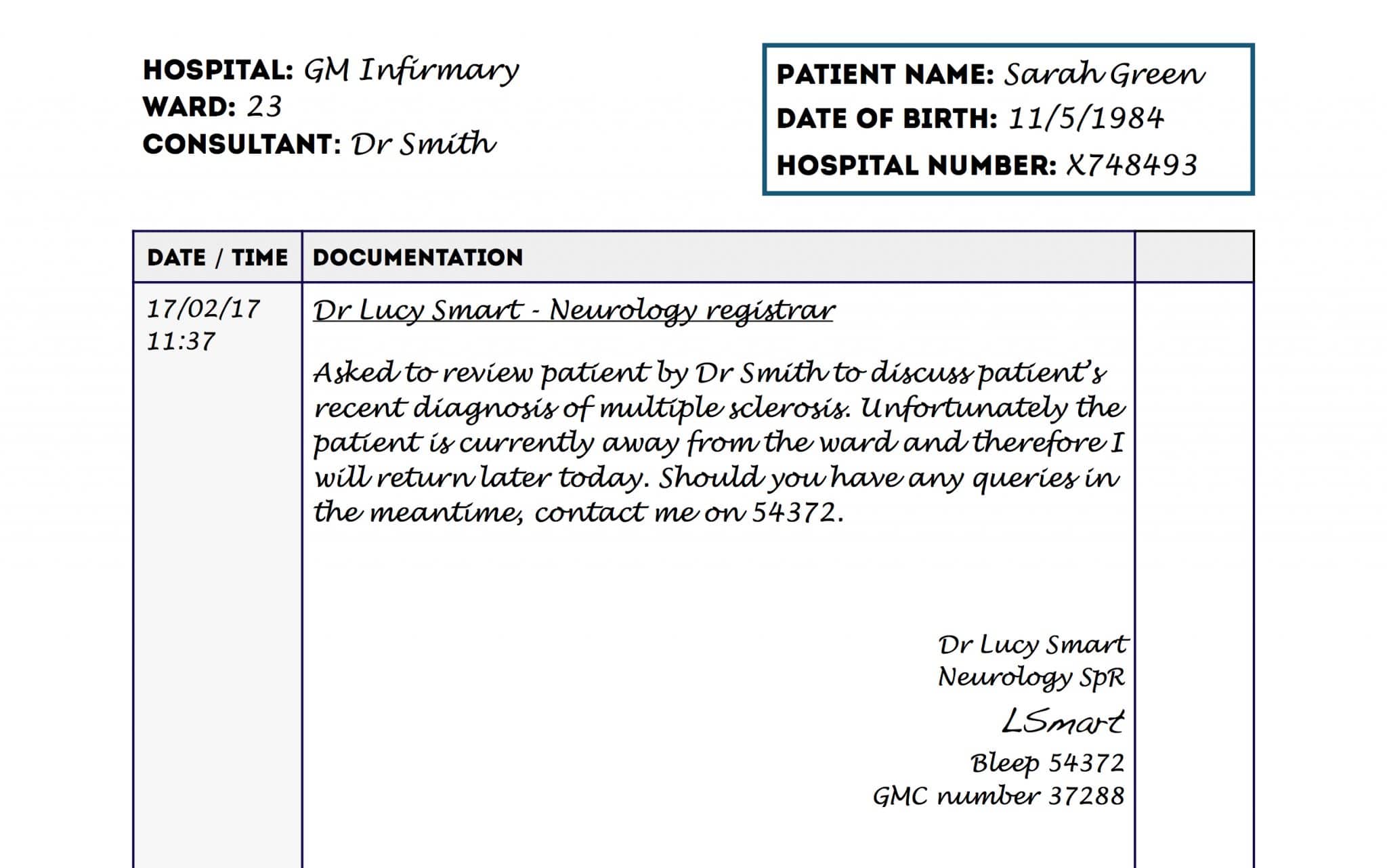
How to make an entry in a patient’s notes
1. Add the date and time (in 24-hour format) of your entry.
2. Write your name and role as an underlined heading.
3. Make your entry in the notes below this heading (see our other documentation guides).
4. At the end of your entry to need to include the following:
- Your full name
- Your grade/role (e.g. Medical Student/F2/Neurology Registrar)
- Your signature
- Your professional registration number (e.g. GMC number)
- Your contact number (e.g. phone/bleep)
Other things to be aware of…
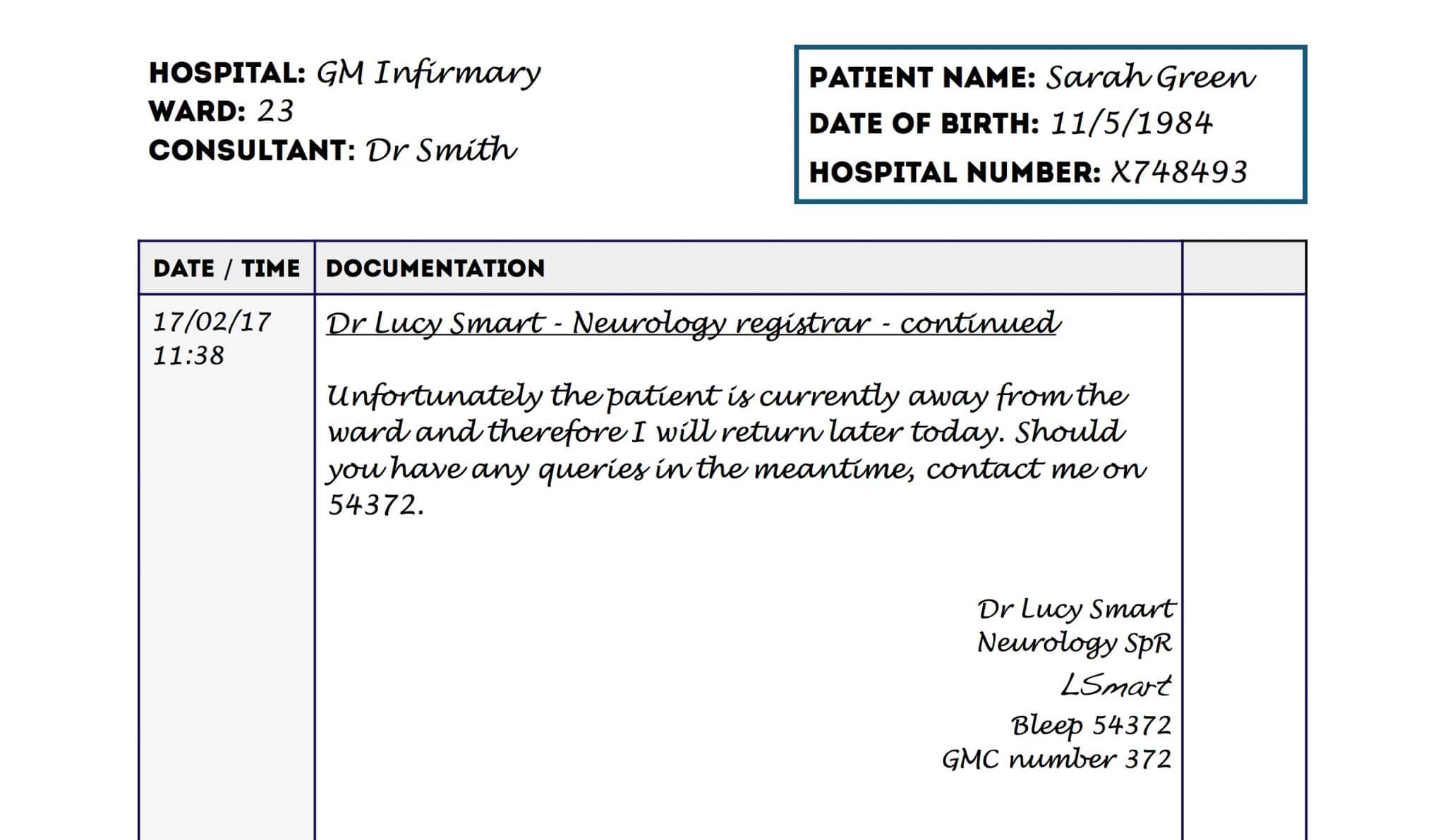
What if your entry spans more than one page?
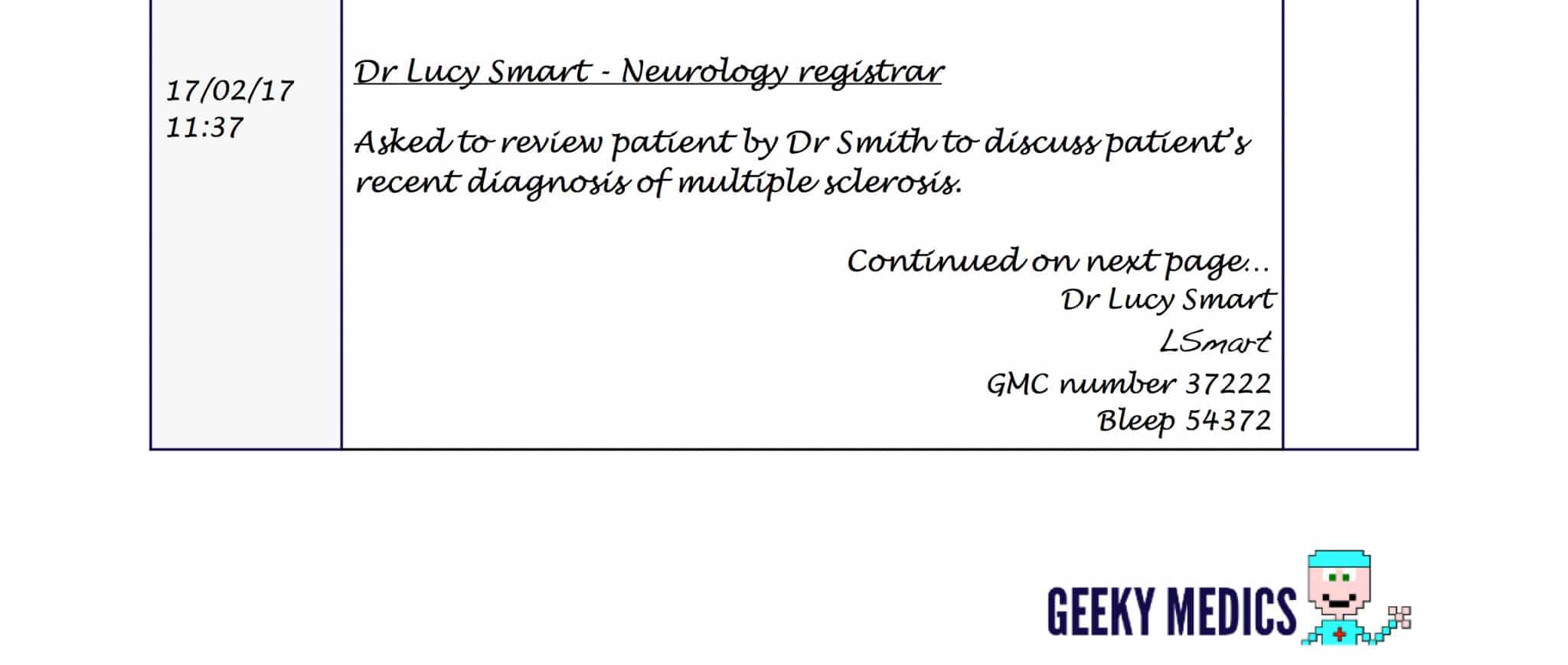
If your entry in the notes happens to span more than one page:
1. Write “continued on the next page” or “continued” with an arrow pointing off the page after the entry on the first page.
2. Write your name, signature, professional registration number and contact number at the end of the first page.
3. Add the patient’s name, date of birth and unique identifier to the new page.
4. Write the date and time of the entry on the second page.
5. Write your name and role, followed by the word “continued” as an underlined heading.
6. Continue the entry from the previous page.
7. At the end of this entry, you need to include all of your details:
- Your full name
- Your grade/role (e.g. Medical Student/F2/Neurology Registrar)
- Your signature
- Your professional registration number (e.g. GMC number)
- Your contact number (e.g. phone/bleep)
Although this may seem tedious it’s actually really important, as it ensures the chronology of your entry is clear to others reading it later.
What if you are too busy dealing with sick patients to write in the notes at the time?
You should always try to document your patient encounters as soon as possible to both reduce the risk of forgetting key details and to ensure other team members are aware of any changes to a patient’s condition or management plan. However, in reality, this isn’t always possible, for instance, if you’re dealing with an acutely unwell patient you need to prioritise their management over the documentation of the sequence of events.
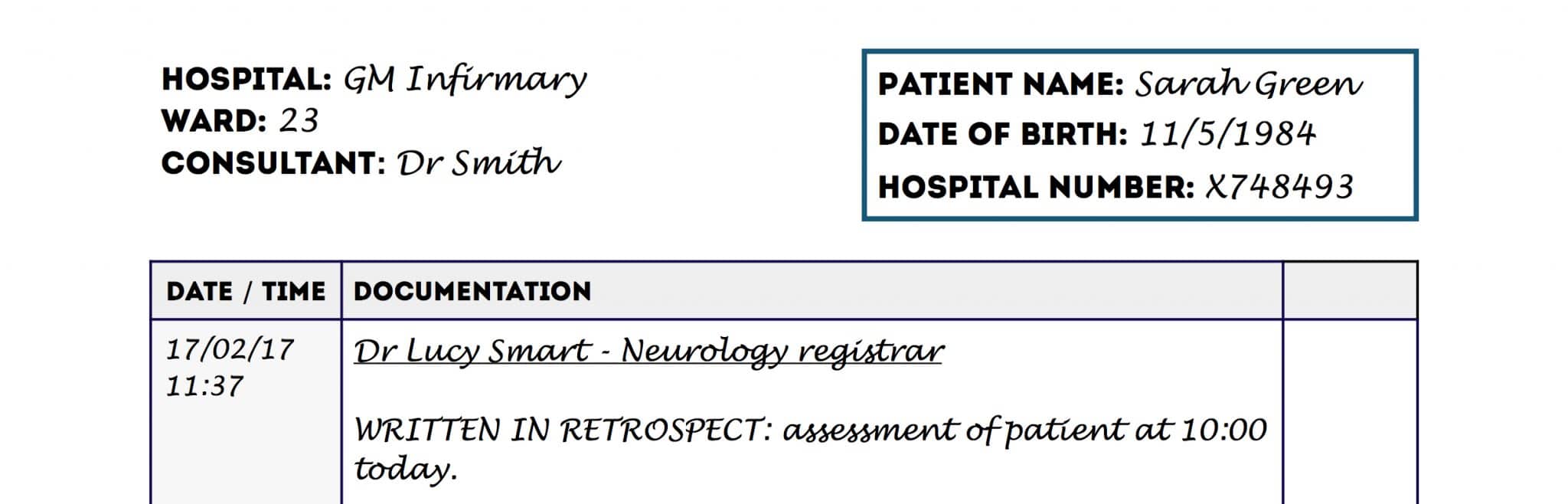
When you return to the patient’s notes at a later time you need to:
1. Ensure the continuation sheet has the patient’s three key identifiers as previously described.
2. Document the current time and date of your entry.
3. Write your name and grade as an underlined title.
4. Begin the entry by stating that this is written in retrospect, with the time the entry is referring to documented clearly.
5. Complete the entry in the notes.
6. At the end of this entry, you need to include all of your details:
- Your full name
- Your grade/role (e.g. Medical Student/F2/Neurology Registrar)
- Your signature
- Your professional registration number (e.g. GMC number)
- Your contact number (e.g. phone/bleep)
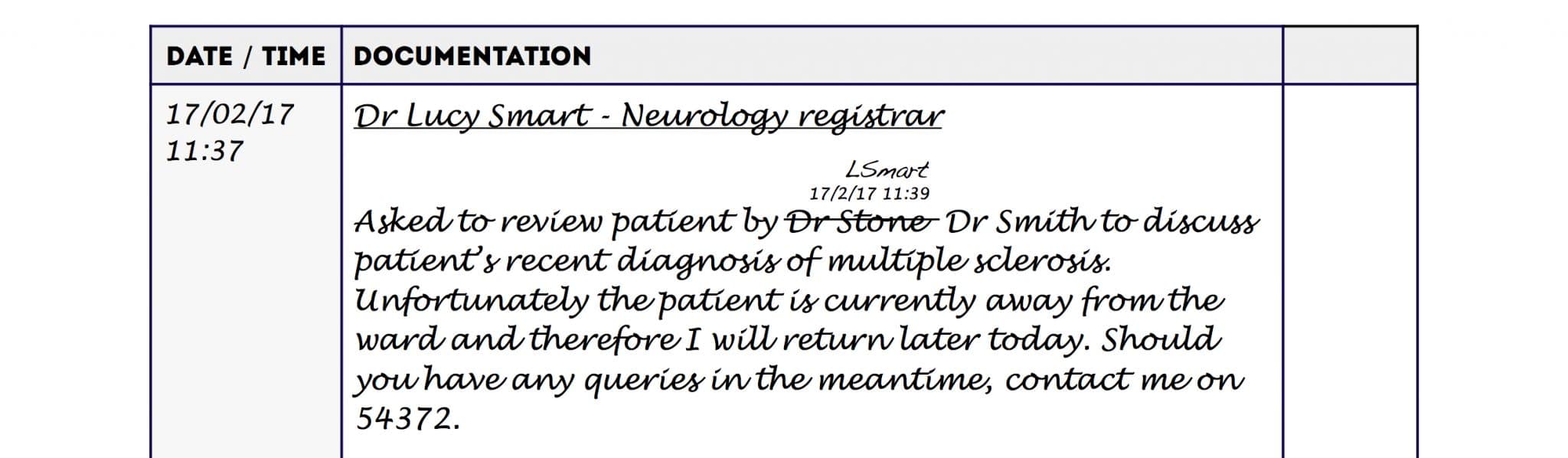
What if I write something incorrectly in the notes?
If you make a mistake whilst making your entry (e.g. factual error/spelling error):
- Simply cross the mistake out with a single line through the erroneous words.
- Write your signature in addition to the time and date beside the area crossed out.
- Do not use Tipp-Ex to erase the errors.
- Do not excessively scribble over the errors to make them unreadable.
Filing the documentation appropriately
You should ensure that you file your documentation in the appropriate place within a patient’s notes. This can differ significantly between hospitals, so ask the team if you’re unsure.
Make sure to put the patient’s notes back in the appropriate trolley or storage area on the ward once you’re finished.
Summary
Hopefully, that was a useful overview of the basics of documentation. Check out our collection of documentation guides to further refine your skills.
References
- Royal College of Physicians. Generic medical record-keeping standards. Available at: [LINK].
