

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Table of Contents
Introduction
Nasal trauma is a common presentation to the emergency department. It can range from minor injuries and bleeds to complex fractures with functional and aesthetic complications.
Depending on the severity of the nasal trauma, a multidisciplinary approach may be required, usually from emergency medicine, otolaryngology (ENT), maxillofacial and plastic surgery.
Understanding the complexity of nasal trauma is crucial as it allows for effective approach, management, and prevention. This article will cover common nasal injuries, diagnostic approach, and management.
Aetiology
Nasal traumas are observed more commonly in men, with alcohol use and intoxication being the leading contributor.1,2
Common mechanisms of injury include:3
- Blunt trauma: leading cause of nasal injuries. This can be seen in various settings, such as physical altercations or sports-related injuries.
- Road traffic collisions: common causes include motor vehicle accidents, cycling, or pedestrian accidents
- Falls: an important cause especially in older patients and children. This can highlight an underlying balance issue.
- Penetrating trauma: results from sharp objects (e.g. stab wounds) breaking the skin into the body
- Assault: can involve a mixed presentation of the above
Clinical anatomy
The nose is a prominent central feature of the face, consisting of nasal bones, cartilage, mucosa, vascular plexus, and paranasal sinuses. It serves both structural and functional roles, acting as a filter, humidifier, and airway passage, while also enabling the sense of smell. Additionally, it contributes significantly to the aesthetic appearance of the face.
Internal and external structures
External nose4-5
Nasal bones: two paired, centrally located small bones that form the nose bridge. Fuses with other bones to form:
- Bony vault: lateral connection to the maxillary bones
- Nasion: superior connection to the frontal bone
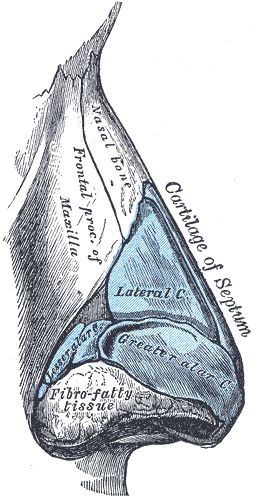
Nasal cartilages:
- Alar cartilages: found at the tip of the nose. Gives structure to the nostrils
- Lateral nasal cartilages: found below the nasal bones
- Septal cartilage: extends from the nasal bones to the vomer and divides the nasal cavity in half
Internal nose
Structures of the internal nose include:
- Nasal septum: consists of septal cartilage, vomer bone inferiorly, and perpendicular plate of ethmoid bone superiorly
- Nasal mucosa: mucus membrane that lines the nasal cavity
- Nasal conchae (turbinates): three pairs of superior, middle, and inferior mucosa-lined bony cavities
- Nasal meatus: three paired spaces located under each of the conchae (Superior, middle, inferior) facilitating sinus drainage
Blood supply
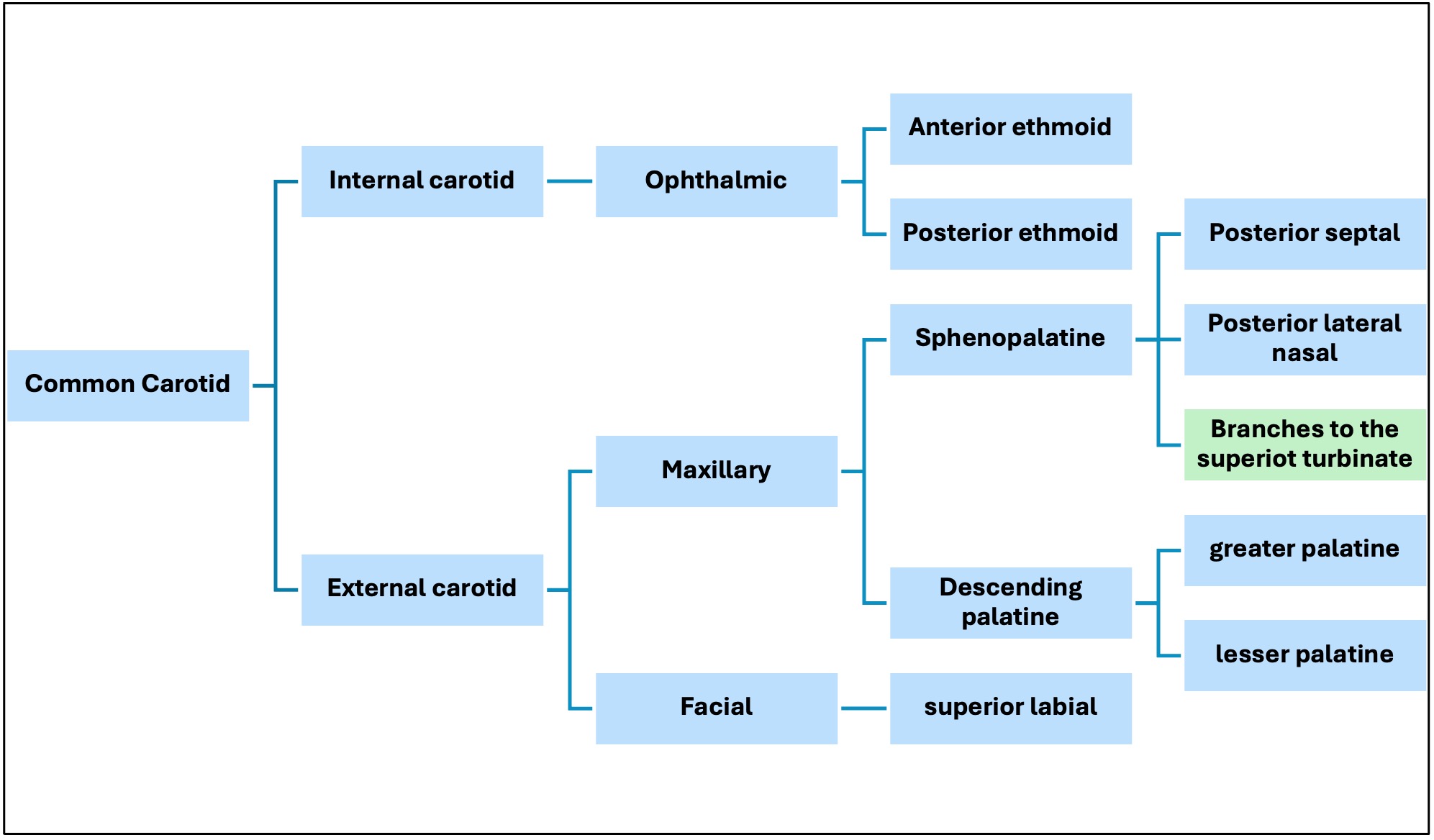
Interestingly, the nasal cavity is the only area in the head and neck to receive dual blood supply from both the internal and external carotid arteries.
Branches from these arteries supply form an anastomosis known as Kiesselbach’s plexus, supplying the anterior portion of the nasal cavity. Little’s area can be located within this plexus, an area which is prone to trauma and bleeds (epistaxis).
Arterial supply includes branches from:6,7
Internal carotid artery:
- Anterior ethmoid artery
- Posterior ethmoid artery
External carotid artery:
- Sphenopalatine artery
- Superior labial artery
- Greater palatine artery
Paranasal sinuses
There are four paired sinuses: maxillary, frontal, ethmoid and sphenoid.
Types of nasal injuries
Nasal injuries can vary in severity and complexity, some common presentations include:1,2
- Contusion: refers to the swelling and bruising of soft tissues of the nose. It is minor in nature and often resolves with conservative management.
- Lacerations: involves cuts or tears in the nasal skin or mucosa commonly due to penetrating trauma, often presenting with pain and bleeding.
- Nasal fractures: a common, and more serious presentation associated with blunt trauma. It accounts for more than 50% of all facial fractures.8 They can present as open or closed, simple or complex, and in isolation or with other facial bone fractures.
- Epistaxis: refers to nosebleeds from one or both nostrils. The bleed can be either anterior or posterior in nature.
- Septal hematoma: blood collection within the nasal septum. Observed as a fluctuating mass on examination of the nasal cavity. If left untreated, avascular necrosis could develop, leading to subsequent infections or abscess formation, and potentially resulting in nasal septal perforation.
- Nasal dislocation: associated with more significant trauma displacing the nasal bones from their normal position. Clinically presents with obvious nose deformities, asymmetry, and sometimes breathing difficulties.
Clinical assessment
History
A comprehensive history of nasal trauma should include the following:
- Mechanism of injury: blunt/penetrating, impact and direction
- Pain severity
- Time of the injury
- Presence of nasal discharges or bleeding
- Presence and degree of nasal obstruction
- Any changes in the sense of smell
- Any history of pre-existing nasal deformities or trauma
Other important areas to cover in the history include:
- Medical and surgical history (e.g. previous nose surgery, bleeding disorders)
- Medications and allergies
- Family history
- Alcohol intoxication
Clinical examination
Before examining the nose, you should always follow the (C)ABCDE approach and treat any other life-threatening injuries first.
General inspection
- Assess the overall appearance and note any bruising or lacerations on the face
- Pay close attention to the orbits and jaw
Nasal inspection
On inspection of the nose’s external structures, you should:
- Inspect the external structure superiorly (bird’s eye view), anteriorly and laterally
- Check for any sign of asymmetry, deformity, or deviation
- Assess the nasal contour and misalignment of the nasal bone
- Check for skin abrasion or bruising
Once you completed the external inspection, continue to examine the nasal cavity:
- Ask the patient to tilt their head back slightly
- Using a headlamp and a nasal speculum assess for any septal deviation, perforation, abscess, or haematoma
- Evaluate for any signs of nasal obstruction, including oedema or discharges
Palpation
Following the inspection, continue with palpation of the nose as follows:
- Gently palpate the nasal bones and cartilages, starting at the nose bridge and working your way down to the nose tip
- Assess for tenderness, depression, crepitus, or any bony irregularity
- Gently check nasal mobility
Other areas to examine
Other areas to examine include:
- Airway assessment: ask the patient to breathe from each nostril separately to assess the airway patency
- Oropharyngeal cavity: posterior epistaxis is associated with blood stains on the posterior pharyngeal wall
- Periorbital evaluation: nasal and orbital fractures can be associated with periorbital swelling or bruising. Assessment of extraocular movements is vital in severe cases.
- Endoscopes: may be used to locate the source of bleeding, or if there is any obstruction
For more information, see the Geeky Medics guide to nasal examination.
Investigations
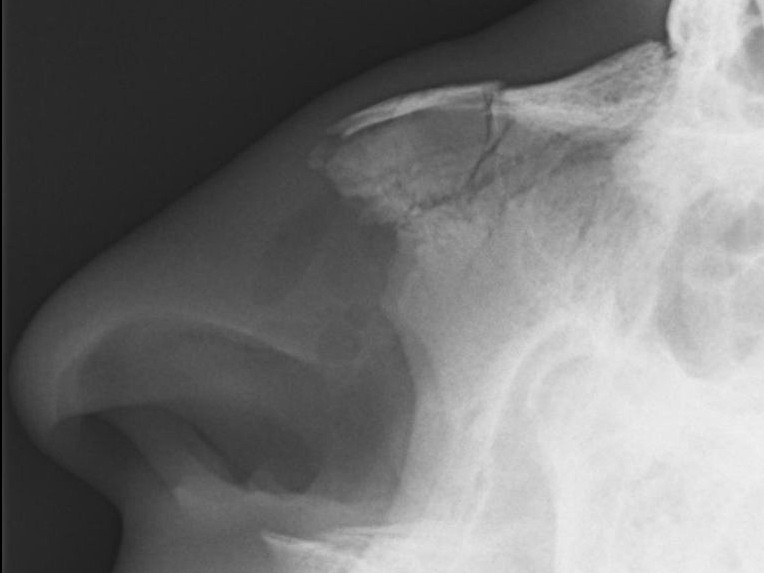
Computed tomography (CT) is indicated for complicated nasal fractures with suspected orbital, maxillary, or other facial fractures.9,10
X-rays are usually not helpful and, therefore, not required for diagnosis or treatment.
Management
The management of nasal trauma will depend on the severity of the presentation, type of injury sustained, and timing.
Initial management
On presentation, initial management should include:11
- Follow the (C)ABCDE approach and treat any life-threatening injury first.
- Ask the patient to lean forward and control any bleeding by applying direct pressure to the nose
- Apply an ice pack or a cold compress to the nose
Specific management
Contusions
Minor injury in nature requiring conservative management. This includes applying ice packs for 15-20 minutes, and simple painkillers.8
Lacerations
When treating lacerations, the following steps are essential:8,11
- Use an antiseptic or saline solution to thoroughly clean the site
- Remove any debris or foreign bodies, and if required debride the site
- Sutures may be required for larger wounds. Usage of non-absorbable sutures or steri-strips is preferred
- Where primary closure of the wound is not possible, referral to plastic surgery may be required
- Analgesia should be provided following WHO analgesic ladder
- Consider giving antibiotics and tetanus prophylaxis
Fractures
For simple fractures, management usually involves waiting until the swelling subsides (10-14 days), then performing a closed reduction of the fracture under local or general anaesthetic.8-9
For complex fractures, surgical intervention is required to realign or stabilise nasal structures.
External splints or nasal packing can be used for stabilisation post-reduction. Analgesia should be provided following the WHO analgesic ladder.
Epistaxis
The following steps should be used to manage epistaxis:
- Ask the patient to lean their head forward to avoid any backtracking or blood swallowing, and pinch the cartilage (soft) part of the nostrils for 10-15 minutes to stop/control the bleeding
- Ask the patient to spit any backtracking blood
- For persistent bleeding, use nasal packing (for anterior bleeds, gauze can be used, while posterior bleeds may require balloon nasal packing)8
- Topical vasoconstrictors (e.g. cophenlycaine) may also be used to reduce the bleeding.12
- For recurrent or severe cases, cauterisation may be required.
- Treat the underlying cause of epistaxis. For example, if a bleeding disorder is suspected, referral to haematology is required. Similarly, if epistaxis is a result of poorly controlled hypertension, the patient may require anti-hypertensive medications.
Septal haematoma
Once recognised, immediate drainage is required under local or general anaesthetic.8,10,12
Nasal packing is used to prevent the blood from reaccumulating and antibiotics should be prescribed to prevent infection.
Nasal dislocation
Nasal dislocations are often managed as follows:10
- Manually reduce and realign the nose
- External splinters or nasal packing can be used for stabilisation.
- Analgesia should be provided
- Consider prescribing antibiotics if there are associated lacerations
Follow up
For simple cases, an initial follow-up should be scheduled within 1-2 weeks after the injury to assess healing, ensure proper alignment, and rule out any possible complications, as outlined below.
Nasal packing, splints, and other instruments can be removed during these visits. For more complex presentations, regular check-ups might be required.
Between visits, patients are advised to:
- Monitor any signs of infections
- Keep proper wound care (e.g. keep the area clean and dry)
- Apply topical antibiotics as required if prescribed
- Avoid blowing their nose harshly post-fracture
- Protect their nose during the healing process (e.g. avoid contact sports)
- Encourage smoking cessation for proper wound healing
Complications
Potential complications include the following:1,10
- Infections
- Nasal deformities (e.g. saddle nose)
- Deviated septum
- Septal perforation
- Chronic nasal obstruction
- Hyposmia/anosmia
- Avascular necrosis
- Orbital fractures
- CSF leak
Key points
- Nasal trauma is a common ED presentation that ranges from minor injuries to complex fractures with functional and aesthetic issues.
- Common causes include blunt trauma (most common), road traffic collisions, falls (especially in older adults and children), penetrating trauma, and assault.
- CT should be performed for complex fractures; X-rays are generally not required.
- Types of injuries include contusions (minor, resolves with conservative management), lacerations (clean, suture, antibiotics), fractures (simple vs. complex), epistaxis (manage with pressure, packing, cautery), septal haematoma (immediate drainage) and nasal dislocation (manual reduction).
- Initial management: follow (C)ABCDE approach, control bleeding, apply icepack; specific management based on injury type.
- Complications: infections, nasal deformities, deviated septum, septal perforation, chronic obstruction, hyposmia/anosmia, avascular necrosis, orbital fractures, CSF leak.
Reviewer
Dr Ruzaimi Ramza Ramli
ENT Registrar
Editor
Dr Chris Jefferies
References
- Pham, T.T., Lester, E., Grigorian, A., Roditi, R.E. and Nahmias, J.T., 2019. National analysis of risk factors for nasal fractures and associated injuries in trauma. Craniomaxillofacial trauma & reconstruction, 12(3), pp.221-227
- Dawood, M.R., 2015. Epidemiological analysis of the nasal trauma. Int J Sci Res, 5, pp.774-777
- Kelley, B.P., Downey, C.R. and Stal, S., 2010, November. Evaluation and reduction of nasal trauma. In Seminars in plastic surgery (Vol. 24, No. 04, pp. 339-347). © Thieme Medical Publishers.
- AlJulaih GH, Sharma P, Lasrado S. Anatomy, head and neck, nose bones. 2019.
- Cappello ZJ, Minutello K, Dublin AB. Anatomy, head and neck, nose paranasal sinuses. 2018.
- Tabassom A, Dahlstrom JJ. Epistaxis. 2022.
- MacArthur, F.J. and McGarry, G.W., 2017. The arterial supply of the nasal cavity. European Archives of Oto-Rhino-Laryngology, 274, pp.809-815
- Koh, J.H., Bhatti, O., Mahmood, A. and Agar, N., 2016. Traumatic nasal injuries in general practice. Australian family physician, 45(9), pp.650-653
- Hoffmann, J.F., 2015. An algorithm for the initial management of nasal trauma. Facial Plastic Surgery, 31(03), pp.183-193
- Nathan, J.M. and Ettinger, K.S., 2021. Management of Nasal Trauma. Oral and Maxillofacial Surgery Clinics, 33(3), pp.329-341
- Alvi S, Patel BC. Nasal fracture reduction. 2019.
- Kuo, C.L., 2019. Updates on the Management of Epistaxis. Clinical Medicine and Therapeutics (CMT)
- Gupta G, Mahajan K. Nasal Septal Hematoma. 2017.
Image references
- Figure 1: Henry Vandyke Carter, Cartilages of the nose, Side view. License: [Public domain]
- Figure 3: Nevit Dilmen, Medical X-ray, Navit nasal bone fracture. [CC BY-SA]
