

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Autism spectrum disorder (ASD) is a neuro-developmental disorder characterised by abnormal social interaction, communication and restricted, repetitive behaviours. ASD is four times more prevalent in boys than girls.1 In the UK, 1 in 100 people are considered to be on the autistic spectrum.2
There are other names used for ASD such as childhood autism or Asperger syndrome. Asperger syndrome is now referred to as autism spectrum disorder; however, it is characterised by the absence of intellectual impairment and/or impairment of functional language.
Aetiology
In most cases, there is no identifiable cause for ASD however there are a few known, predisposing medical conditions. These include:
- Infantile spasms
- Congenital rubella
- Tuberous sclerosis
- Fragile X syndrome
Risk factors
Risk factors for ASD include:
- Male sex
- Family history
- Genetic variants such as PTEN, MeCP and several submicroscopic copy number variants (CNV)
- Chromosomal abnormalities
Clinical features
Typical features of ASD can be classed into three categories: social interaction, communication and restricted, repetitive behaviours.
Social interaction
Patient’s may exhibit the following social features:
- Lack of response to other people’s emotions
- Unable to interpret social cues
- Inability to form social attachments
Communication
Patient’s may exhibit the following communication features:
- Usually delayed or minimal expressive speech
- Impairment in make-believe or fantasy play
- Lack of social gestures
- Conversational skills tend to be one-way (monologues, endless questions etc…)
Restricted, repetitive behaviours
Patient’s may exhibit the following behaviours:
- The tendency to resist change with a rigid daily routine
- Preoccupations with specific interests like dates or timetables
- Inability to adapt to new environments
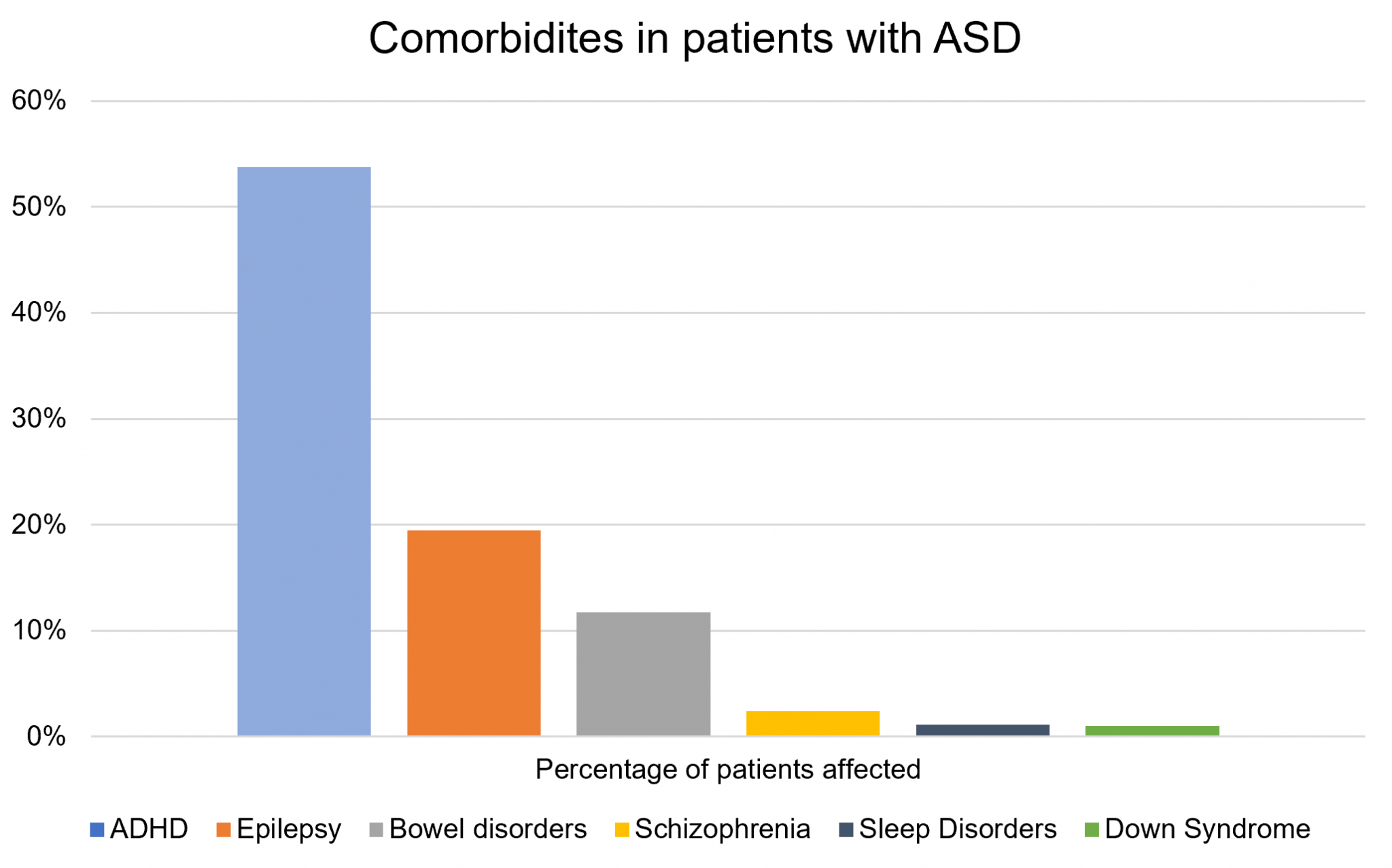
In addition to ASD, there are many conditions which have increased prevalence in people with ASD (Figure 1). For example, 20-30% of patients will also have epilepsy and around half will have a concomitant diagnosis of attention deficit hyperactivity disorder (ADHD).3,4
Differential diagnoses
Differential diagnoses for ASD may include:
- Global developmental delay: delay occurring in all areas of development, not just social/communication
- ADHD: difficulties with hyperactivity, attention, and impulse control.
Investigations
A diagnosis of ASD is based on clinical assessment with deficits occurring across all three aforementioned domains.
These features must be observable in all environments that are sufficient to cause impairment in functional capacity.
They should have been present from early childhood but may not be fully evident until later when social demands exceed capabilities.
There are several formal diagnostic tools for ASD, including Diagnostic Interview for Social and Communication Disorders (DISCO) and Autism Diagnostic Observation Schedule (ADOS).
Management
There is no cure for ASD, but the goal of treatment is to improve day-to-day functional ability and optimise the quality of life. Interventions may need to evolve over time as the needs of the patient evolve with age.
Early intervention in pre-school years is preferable as it can help children learn critical social, communication, functional and behavioural skills. Behavioural problems may become particularly challenging during the teenage years.
Non-pharmacological therapy
There is a wide range of non-pharmacological support that may be helpful depending on the patient’s needs:
- Specialist education
- Occupational therapy
- Speech therapy
- Clinical psychology
- Sleep hygiene
- Care agencies
Pharmacological therapy
There are no specific medications for ASD; however, patients with symptoms of depression and/or anxiety may benefit from behavioural and pharmacological intervention (e.g. SSRIs).
In addition, children with sleep difficulties which may benefit from a trial of melatonin if behavioural management/sleep hygiene proved to be unsuccessful.
Practical tips for approaching autistic patients in hospital/appointments
Managing patients with ASD clinic/hospital can seem a daunting task however the most important thing you can do is to try to put the patient at ease and engage them in their care.
Firstly, try not to have too many people in the room as this may be overwhelming, having a member of staff they know present may be helpful.
Try to find out in advance how the patient communicates, because there can be variation in functional language ability- one patient may be non-verbal whereas another may be able to hold a full conversation. Some patients may use pictures/symbols to communicate so it may be useful to ask a parent/carer to bring some with them. Use clear, direct literal language without any turns of phrase or sarcasm that may be misconstrued.
Another important thing to remember is autistic children grow up into autistic adults. Being in the hospital may be a very stressful time for anyone but particularly patients with ASD. The sudden change to an unfamiliar chaotic environment can trigger high levels of stress and anxiety which may convert into challenging behaviour. Having a highly structured clear routine can help ease some of this, it may help to follow a now and next pattern i.e. now it’s breakfast, next you will see the doctor. Also, enabling company of people they trust is vital to help reduce stress and calm behaviours.
For more information on approaching patients with ASD particularly in general practice, NHS Education for Scotland produced this guide.
Complications
There are several ‘complications’ or challenges that patients with ASD may face personally and interpersonally, including:
- Social isolation
- Bullying and victimisation
- Problems in education
- Problems with employment
- Inability to live independently
Key points
- ASD is a neurodevelopmental disorder which affects 1 in 100 people; it is more common in boys than girls.
- ASD consists of deficits in three main domains: social interaction, communication, and restricted, repetitive behaviours.
- Management may involve combined input from specialist education, occupational therapy, speech therapy and clinical psychology depending on an individual’s level of difficulties.
- Try to communicate with patients with ASD in a way that they can engage with (i.e. simple sentences/symbolic aids).
- Hospital wards are very stressful environments for people with ASD, which may trigger an escalation in behaviour.
References
- ICD-11. Published in 2020. Available from: [LINK]
- National Autistic Society. What is Autism? Published in 2020. Available from: [LINK]
- BMJ Best Practice. Autism Spectrum Disorder. Published in 2018. Available from: [LINK]
- The Lancet Psychiatry. ADHD in children and young people: prevalence, care pathways, and service provision. Published in Available from: [LINK]
- Kohane et al. The Co-Morbidity Burden of Children and Young Adults with Autism Spectrum Disorders. Published in 2012. Available from: [LINK]
- Ganizadeh, A. Co-morbidity and factor analysis on attention deficit hyperactivity disorder and autism spectrum disorder DSM-IV-derived items. Published in 2012. Available from: [LINK]
Reviewer
Dr Lesley Henderson
Consultant Community Paediatrician
Editor
Hannah Thomas
