

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Describing the mechanism of labour is a common topic for OSCEs and MCQs. Although on the surface it can appear complicated, breaking the process down into individual steps makes it much easier to understand.
Normal labour involves the widest diameter of the fetus successfully negotiating the widest diameter of the bony pelvis of the mother via the most efficient route.
The mechanism of labour covers the passive movement the fetus undergoes in order to negotiate through the maternal bony pelvis. Labour can be broken down into several key steps.
Key stages of labour
- Descent
- Engagement
- Neck flexion
- Internal rotation
- Crowning
- Extension of the presenting part
- Restitution
- External rotation
- Lateral flexion
For the purposes of this guide, the fetal movements will be described in relation to a cephalic (vertex) presentation with a longitudinal lie. This is a common (low risk) presentation.
Pelvic anatomy
To understand the mechanism of labour, you need some basic understanding of pelvic anatomy.
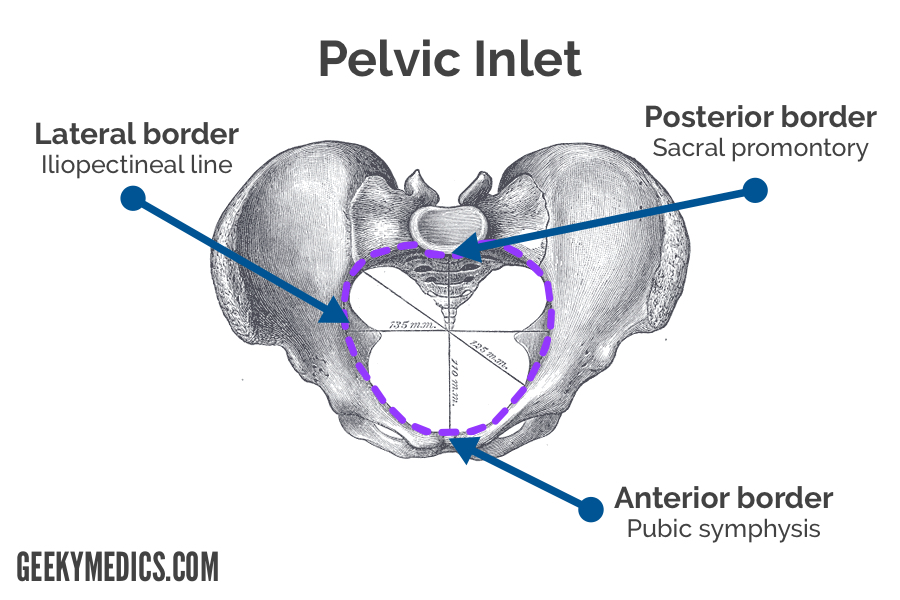
Borders of the pelvic inlet
- Posteriorly: Sacral promontory
- Laterally: Iliopectineal line
- Anteriorly: Pubic symphysis
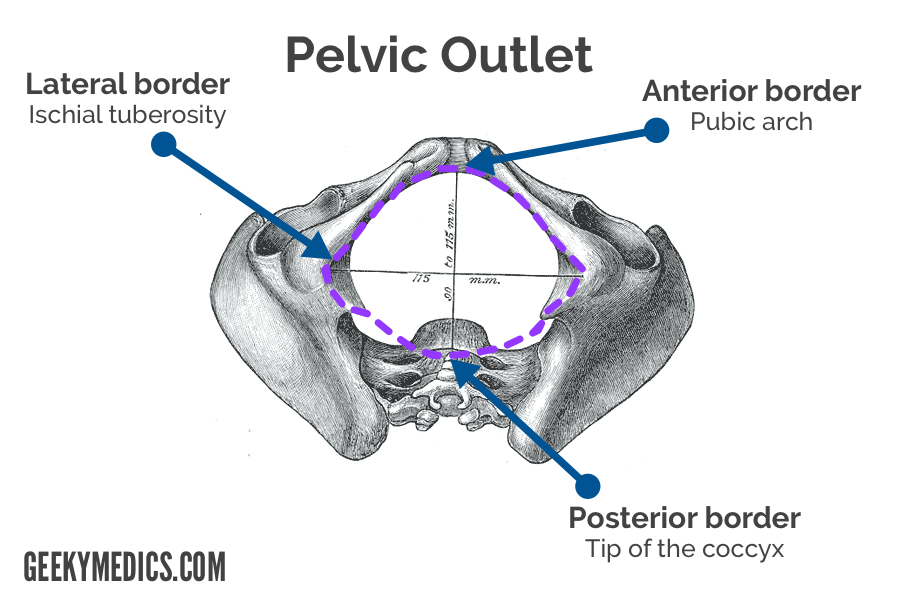
Borders of the pelvic outlet
- Posteriorly: Tip of the coccyx
- Laterally: Ischial tuberosity
- Anteriorly: Pubic arch
Pelvic dimensions
| Transverse diameter | Antero-posterior diameter | |
| Pelvic inlet | 13cm | 11cm |
| Mid-pelvis | 12cm | 12cm |
| Pelvic outlet | 11cm | 13cm |
Since the transverse diameter is greater than the antero-posterior (AP) diameter in the pelvic inlet, the widest circumference of the fetal head descends in a transverse position. However, when it gets closer to the pelvic outlet, the nature of the pelvic floor muscles encourages the fetal head to rotate from a transverse position to an anterior-posterior position, as the AP diameter is greater than the transverse diameter.
Fetal head diameter varies depending upon the degree of neck flexion
It is also important to know how the circumference of the fetal head varies with different degrees of neck flexion:
- Suboccipitobregmatic (vertex, flexed) is 9.5cm
- Occipitofrontal (vertex, neutral flexion) is 11.0cm
- Submentobregmatic (face) is 9.5cm
- Verticomental (brow) is 13.5cm
Descent & engagement
It should be noted that descent and engagement occur together, rather than as completely separate/distinct stages, so consider them as 2 parts of the same process/stage.
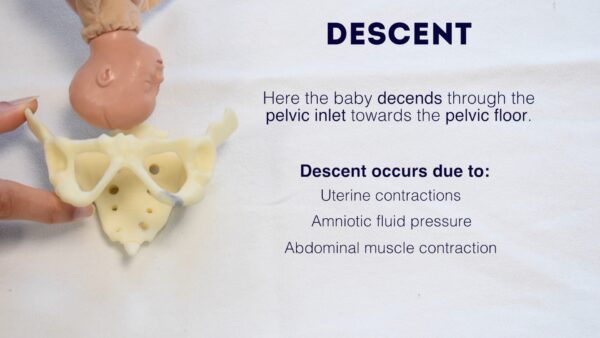
Descent
The fetus descends into the pelvis.
In the primigravida this is likely to occur from 38 weeks gestation onwards, in a multigravida woman, this may not occur until labour is established.
Descent is encouraged by:
- Increased abdominal muscle tone
- Braxton hicks in the late stages of pregnancy
- Fundal dominance of the uterine contractions during labour
- Increased frequency and strength of contractions during labour
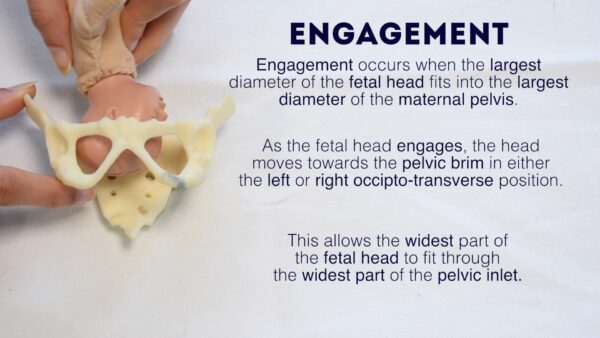
As the head descends, it moves towards the pelvic brim in either the left or right occipito-transverse position (this means the occiput can be facing the left side or right side of the mother’s pelvis).
Engagement
This is when the largest diameter of the fetal head descends into the maternal pelvis.
The term engagement is referring to the widest part of the fetal head successfully negotiating its way down deep into the maternal pelvis. Engagement is identified by abdominal palpation, where the fetal head is 3/5th palpable or less.
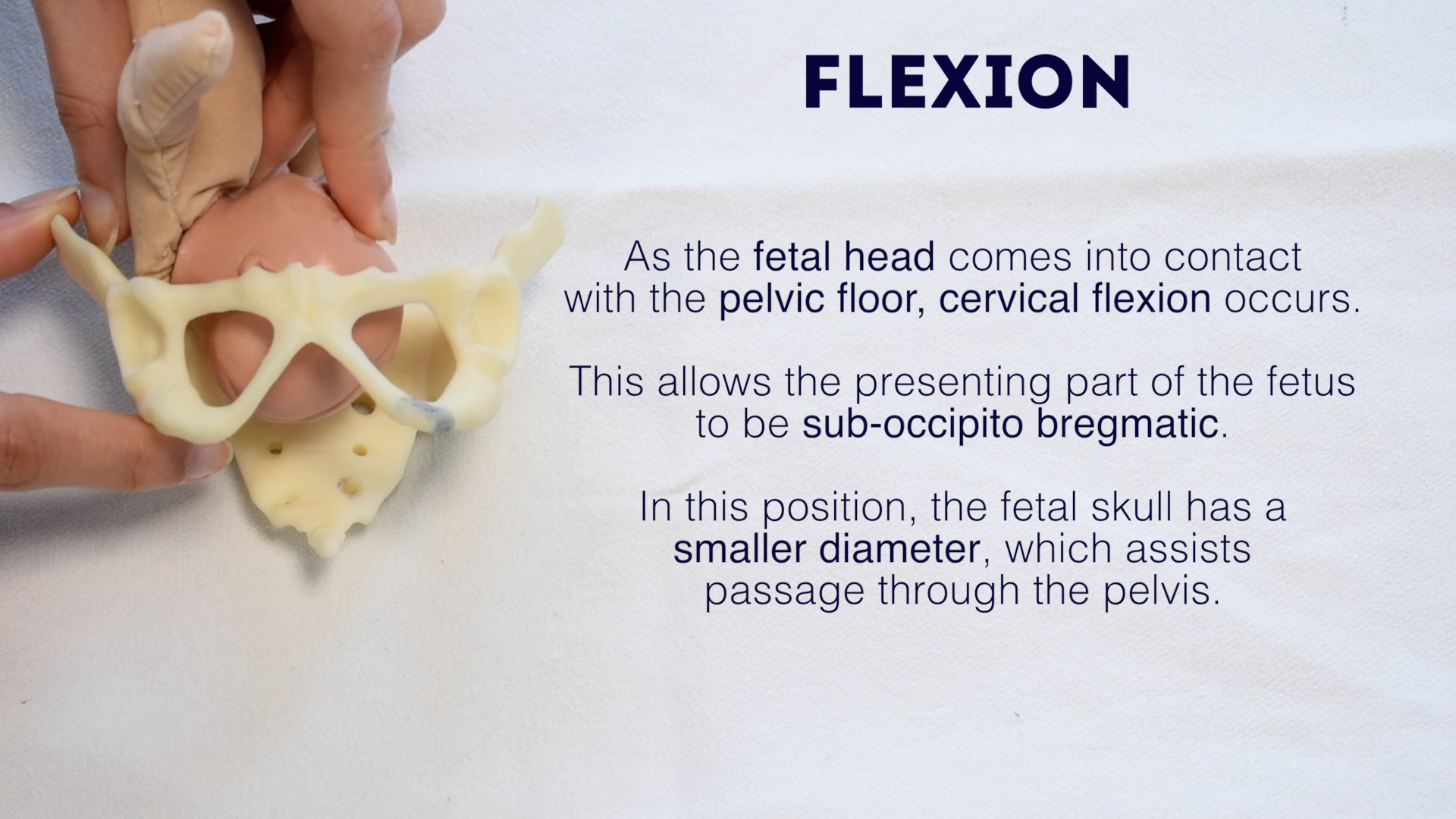
Flexion
As the fetus descends through the pelvis, fundal dominance of uterine contraction exerts pressure down the fetal spine towards the occiput, forcing the occiput to come into contact with the pelvic floor. When this occurs the fetal neck flexes (chin to chest) allowing the circumference of the fetal head to reduce to sub-occipitobregmatic (9.5cm).
In this position, the fetal skull has a smaller diameter which assists passage through the pelvis.
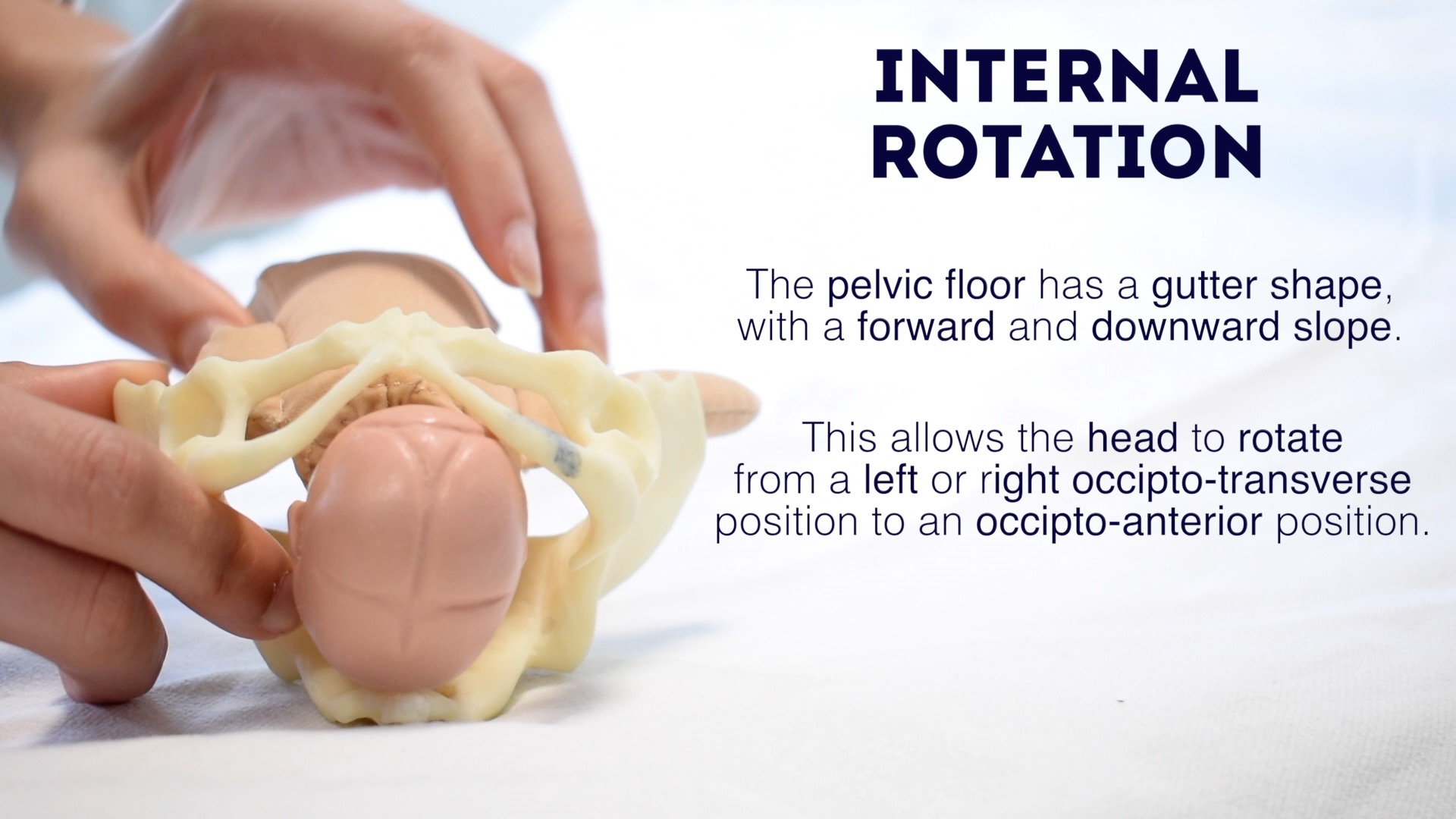
Internal rotation
The pelvic floor has a gutter shape with a forward and downward slope, encouraging the fetal head to rotate from the left or right occipito-transverse position a total of 90-degrees, to an occipital-anterior (occiput facing forward) position, to lie under the subpubic arch.
With each maternal contraction, the fetal head pushes down on the pelvic floor. Following each contraction, a rebound effect supports a small degree of rotation. Regular contractions eventually lead to the fetal head completing the 90-degree turn.
This rotation will occur during established labour and it is commonly completed by the start of the second stage. Further descent leads to the fetus moving into the vaginal canal and eventually, with each contraction, the vertex becomes increasingly visible at the vulva.
Crowning
When the widest diameter of the fetal head successfully negotiates through the narrowest part of the maternal bony pelvis, the fetal head is considered to be ‘crowning’. This is clinically evident when the head, visible at the vulva, no longer retreats between contractions. Complete delivery of the head is now imminent and often the woman, who has been pushing, is encouraged to pant so that the head is born with control.

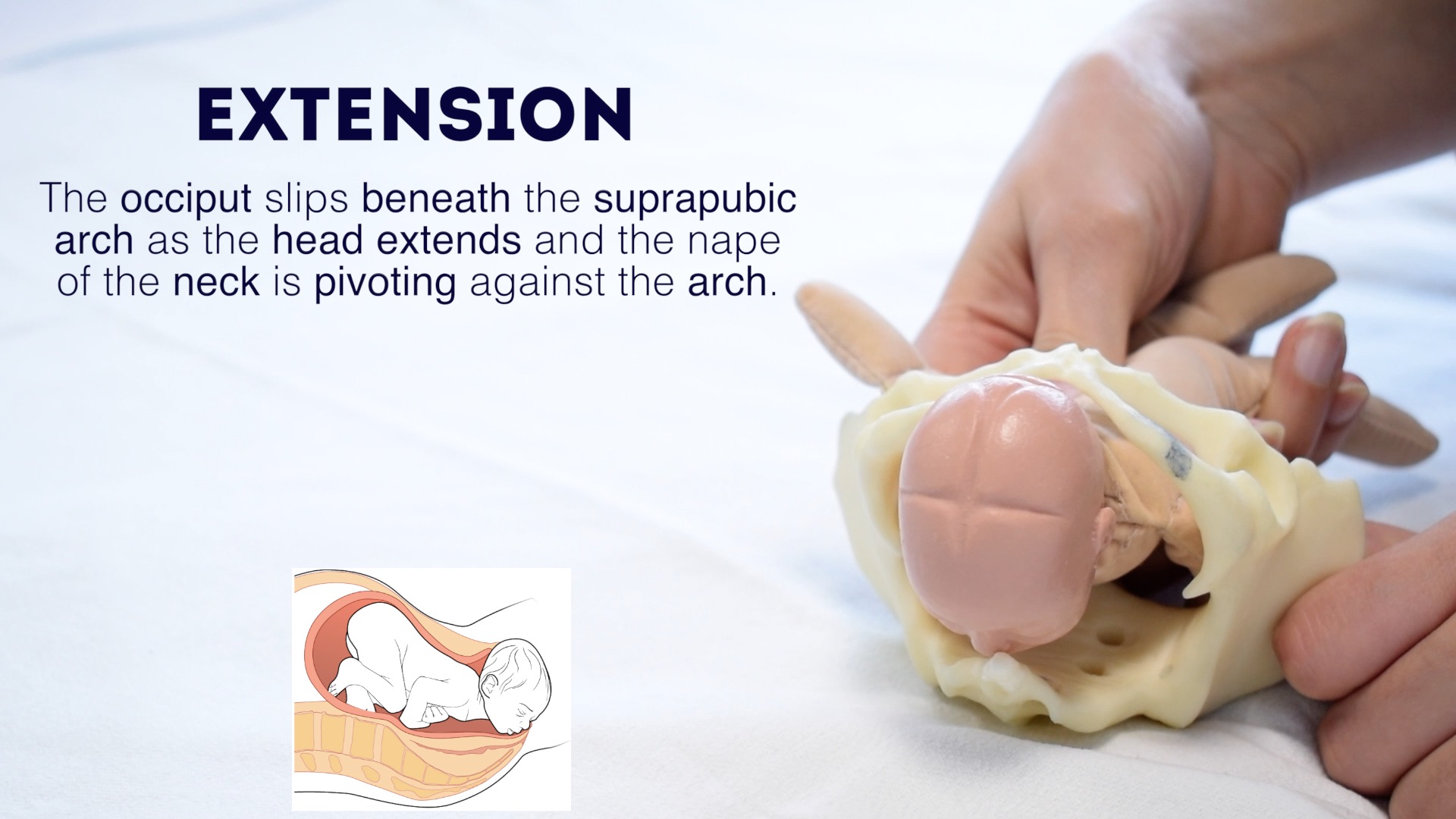
Extension of the presenting part
The occiput slips beneath the suprapubic arch allowing the head to extend. The fetal head is now born and will be facing the maternal back with its occiput anterior.
External rotation & restitution
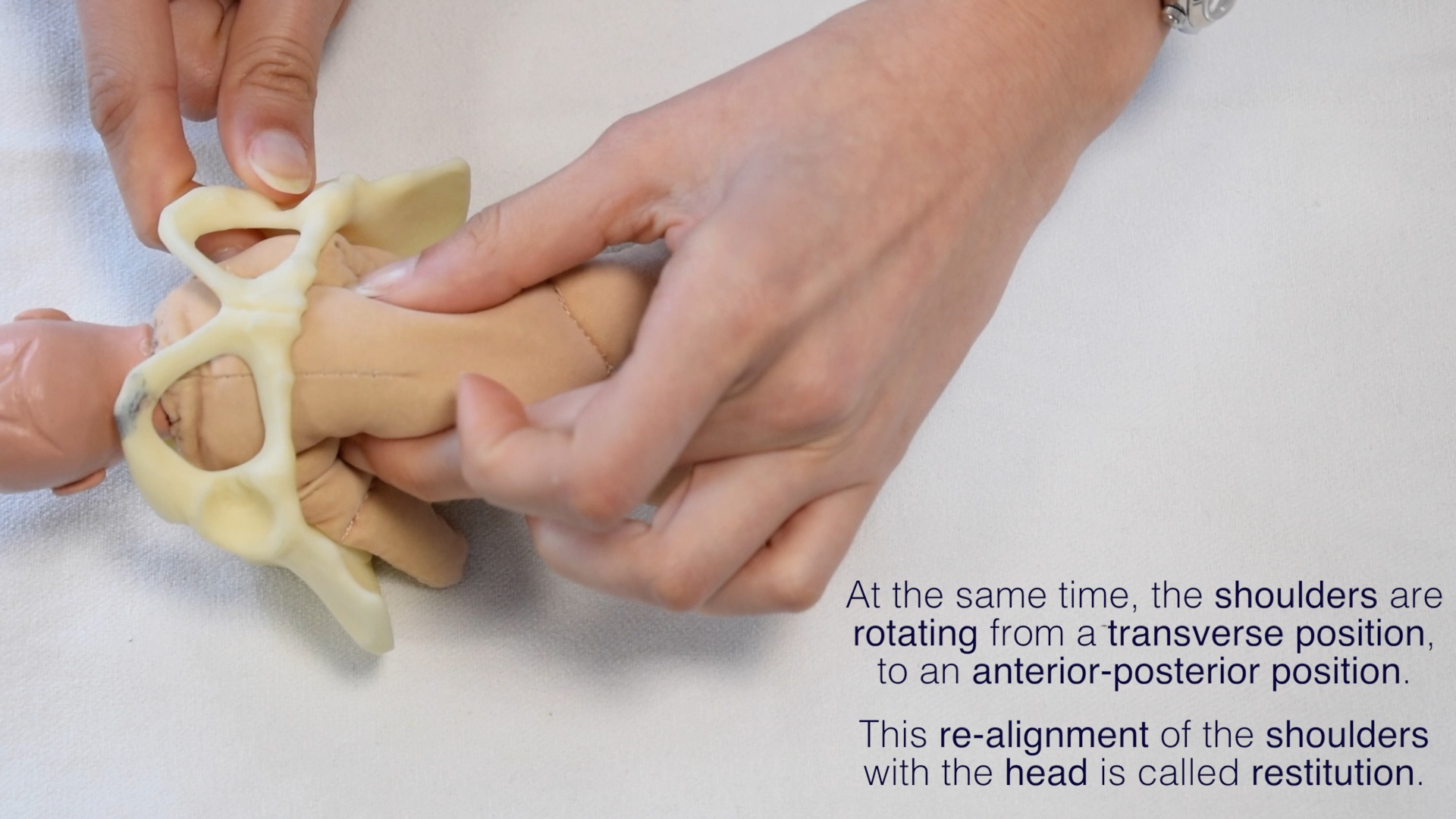
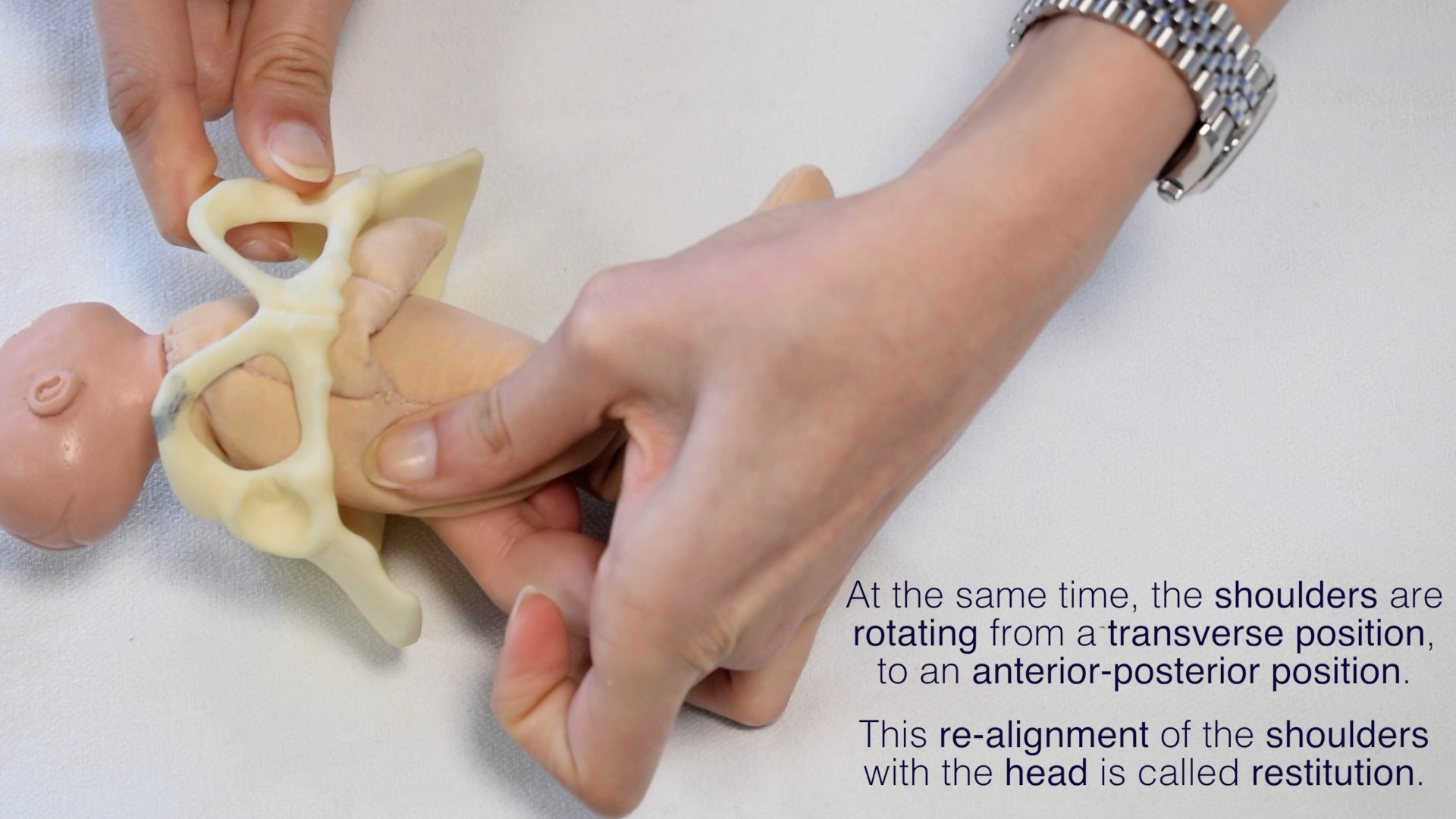
Because the shoulders at the point of the head being delivered are only just reaching the pelvic floor they are often still negotiating the pelvic outlet and the fetus may naturally align its head with the shoulders. This is called restitution and visually you may see the head externally rotate to face the right or left medial thigh of the mother.
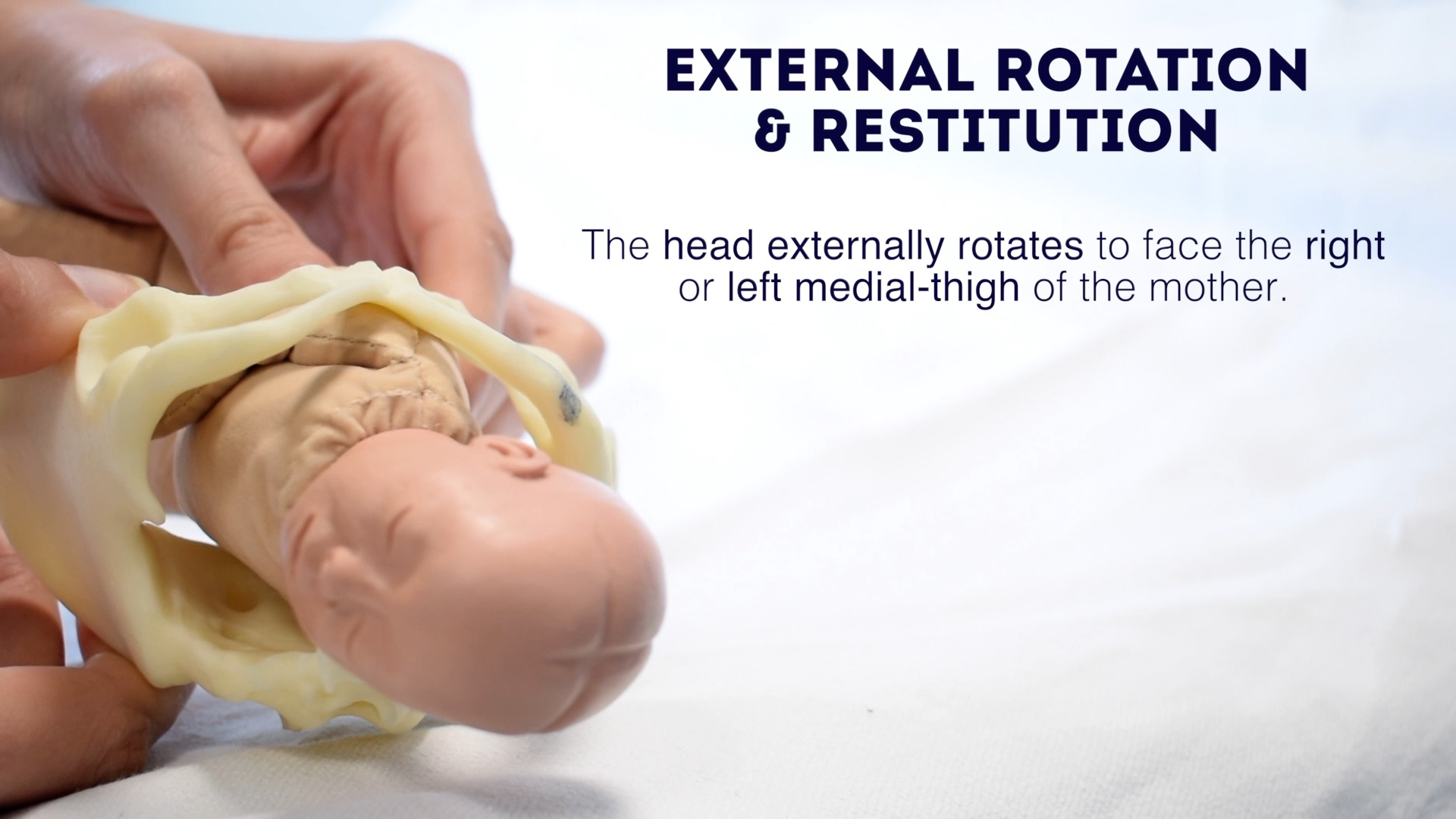
During the next contraction, the shoulders, having reached the pelvic floor, will complete their rotation from a transverse position to an anterior-posterior position. Evidence of this manoeuvre happening inside can be visualised by seeing the head externally rotating as the fetus keeps its spine aligned.
Delivery of the shoulders and body
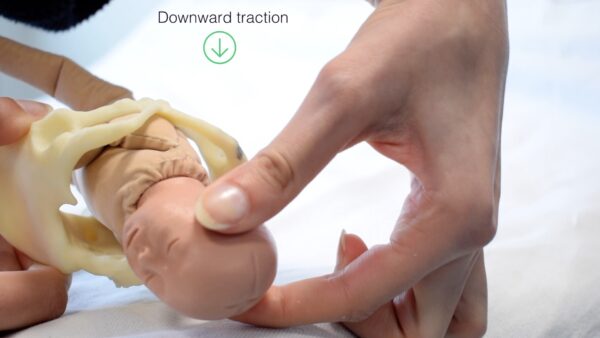
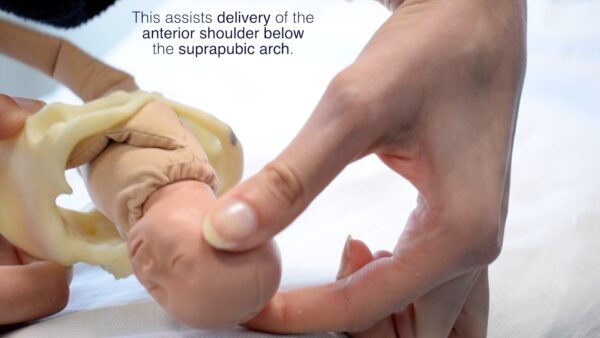
Downward traction by the healthcare professional will assist the delivery of the anterior shoulder below the suprapubic arch.
This is followed by upward traction assisting the delivery of the posterior shoulder.
The fetal body will be delivered by the contractions, the health professional’s role is only to assist safe negotiation of this last stage.


Authors
Faye Alabdulghafoor
Junior Doctor
Josh Chambers
Junior Doctor
Reviewer
Dr Margaret Bunting
Midwife and Senior Lecturer in Medical Education
