
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
A flap is a section of soft tissue outlined by a surgical incision. It carries its own blood supply, permits surgical access, and when replaced and sutured is expected to heal by primary intention. A full-thickness mucoperiosteal flap includes the surface mucosa, submucosa and the periosteum. Flap design in dentoalveolar procedures varies depending on the procedure, access, aesthetics and, operator preference. Despite the variation, common principles apply to all flap designs regardless of clinical indication, namely good access and vision, maintenance of a rich vascular supply and a good aesthetic outcome.
As the oral mucosa is highly vascular, a variety of flap designs are used, but lack of proper planning can result in difficulty, therefore it is paramount that the operator has an appropriate plan prior to initiating treatment.1Careful flap design is important to avoid complications including flap necrosis, dehiscence, bruising and tearing damage to adjacent vital structures, and to promote tissue healing.
Common surgical principles
Flap size has a limited influence on flap healing. Generally, flap designs for dento-alveolar surgery must be of adequate size to permit maximal access with minimal trauma to the tissues and surgical area. They should be wider than the underlying bony defect.2
For most oral surgical procedures, a 15 blade is utilised to create the wide-based incision. It should be made at 90-degrees (perpendicular) to the wound surface in order to avoid a chamfered edge – this maximises the healing potential of the area.2 The incision should be made with a firm, continuous stroke, from the attached to free gingiva, through the aforementioned layers, clean to the bone. The design should be such that damage to vital blood vessels and nerves are avoided.
The base of the flap should be wider than the free margin. This will preserve flap blood supply, and in turn, prevent flap ischaemia and necrosis. Ideally, the height of the flap must never be greater than the base. Relieving incisions should be made at an obtuse angle, to create an ‘L-shape’; this will permit visualisation of the surgical area and maintain a vascular supply to the base of the flap.3 They should extend to the interdental papilla to avoid contraction healing resulting in exposure of the cervical area of the tooth and gingival recession.
Flap margins must lie on sound bone to avoid unnecessary dehiscence post-operatively. Likewise, incisions over bony prominences must be avoided to avoid the flap being closed under tension resulting in pressure on the wound. A suture line that lies over healthy bone will promote healing by primary intention.
Mucoperiosteal flaps should be reflected clean to bone to avoid unnecessary trauma to the underlying tissues which would delay healing.2 Importance should be placed on minimising trauma to the interdental papillae. Surgical technique should avoid crushing or tearing of the mucosa, and the tissues should be kept moist throughout the procedure. When retracting the flap, the instrument (e.g. Bowdler-Henry/Minnesota retractor) must rest on healthy bone to avoid the flap being held under tension. This avoids further trauma, reduces pain, scarring and inflammation.
Type of mucoperiosteal flap
Envelope flap
The envelope flap (Figure 1), or ‘sulcular flap’, is a one-sided extended crevicular incision freeing the interdental papillae. As a result, it requires sufficient length to permit adequate reflection and visualisation of the surgical area.1 This flap is utilised both buccally and palatally, especially for surgery involving incisors, canines and pre-molars. Palatal incisions and flap reflection can be more technically challenging due to the taut nature of the mucosa; a larger reflection is often required in these cases.
Advantages:
- Lower risk of damage to vital structures
- Easy approximation
- Reduced scarring
- A wide base assures vascularity
Disadvantages:
- Periodontal damage and recession due to sulcular incision
- Reduced access, challenging to reflect
- Tearing

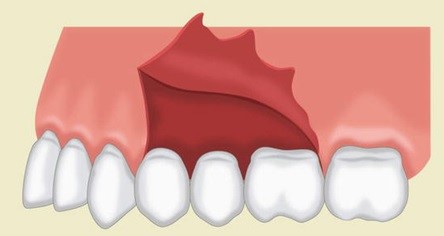
Triangular flap (2-sided flap)
The triangular flap, or two-sided flap (Figure 2), involves a horizontal incision along the gingival crevice with a single vertical relieving incision. The relieving incision should include the interdental papilla. Care should be taken to avoid vital structures when planning this type of flap.1This flap design is helpful for surgical removal of root tips and apicectomy procedures and is useful in cases where access may need to be extended.
Advantages:
- Satisfactory visualisation
- Flap stability
- Adequate blood supply
- Easy to adapt
- Decreases tension forces
Disadvantages:
- Easy to tear adjacent tissues if exposure inadequate
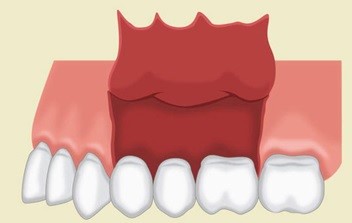
Trapezoidal flap (3-sided)
The trapezoidal or three-sided flap (Figure 3), involves a horizontal incision along the gingival crevice with two vertical relieving incisions at the medial and distal aspect. As with triangular flaps, the relieving incisions should include the interdental papillae. This flap design is helpful for third molar extractions. The approximation of this flap to its original position will increase the healing process.
Advantages:
- Excellent access
- Vascular supply maintained
- Potential for surgery to be performed on a number of teeth
- No tension on the tissues
Disadvantages:
- More challenging closure
Semi-lunar flap (including a Luebke-Ochsenbein flap)
A semi-lunar flap (Figure 4) results from a curved incision made at least 0.5cm apical to the gingival margin. It begins beneath the vestibular fold, following a bow-like curvature extending to a minimum of one tooth on either side of the surgical site. It is often utilised in apicectomies, cyst surgery or removal of root tips.1,4 These incisions are often utilised when there is potential for aesthetic compromise (e.g. fixed crown and bridgework).
Advantages:
- Useful in areas where aesthetics may be compromised by recession
Disadvantages:
- Tendency to tear
- Limited access and visualisation
- Can result in numbness due to nerve damage

Luebke-Ochsenbein flap
The Luekbke-Ochsenbein flap (Figure 5) is similar to that of the semilunar flap, in that it is best utilised in the anterior maxilla.4Again, a horizontal incision is made 3-4mm above the gingival margin, however, two vertical relieving incisions are made a minimum of one tooth either side to the surgical site. This flap provides excellent retraction as well as visibility and is best utilised for apical surgery. This type of flap is useful for patients with fixed prostheses.1
Advantages:
- Easy to raise
- Less aggressive to sulcular tissue
- Good in areas of aesthetic compromise (e.g. fixed prostheses)
Disadvantages:
- Scarring
- Numbness of overlying mucosa


Pedicle flaps
Pedicle flaps utilise an area of tissue to cover a defect (e.g. for the closure of an oral-antral communication). It is imperative that these areas are closed tension free to avoid further wound breakdown. They require a broad-based, well vascularised, soft tissue flap and involve the advancement of the local soft tissues. Many types of flap can be utilised, including a buccal advancement with or without a buccal fat pad, or palatal advancement.5 Flaps of this nature require both epithelium and connective tissue, periosteal release and scoring to release tension and mattress sutures for closure.
Advantages:
- Useful for the closure of larger defects
- Utilising adjacent anatomy rather than free gingival tissue with poorer vascular supply
Disadvantages:
- Can cause loss of the vestibular depth buccally making possible denture wear challenging5
References
- Alfotawi, Randa. Flap techniques in dentoalveolar surgery. Published in 2020. Licence: CC BY 3.0. Available from: [LINK].
- Stenhouse, D. Basic Oral Surgical Technique, Textbook of General and Oral Surgery. Chapter 23, pages 189-200. Churchill-Livingstone 2003.
- Yolcu, U. and Acar, A.H. Comparison of a new flap design with the routinely used triangular flap design in third molar surgery (2015) Available from: [LINK].
- Diago, M.P. and Ballester, J.C. Flap design: new perspectives in periapical surgery (2017). Available from: [LINK].
- Khandelwal, P. and Hajira, N.Management of oro-antral communication and fistula: various surgical options. (2017) Available from: [LINK].
