
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
The upper airway, above the beginning of the trachea, can be divided into the supraglottic, glottic and subglottic regions:1
- The supraglottic region is between the tip of the epiglottis and the start of the glottis
- The glottic region is at the level of the two vocal cords
- The subglottis is located below the vocal cords to the inferior aspect of the cricoid cartilage
The subglottic region can narrow (subglottic stenosis), causing airway compromise in children and adults.
Subglottic stenosis has a wide range of patient groups and presentations. This could be anything from a neonate with stridor to a trauma patient in ED to a medical patient with chronic reflux.
Aetiology
There are a variety of causes of subglottic stenosis. The aetiology can broadly be divided into acquired, idiopathic and congenital.
Acquired subglottic stenosis occurs most frequently following trauma, which can be split into external and internal:
- External trauma: road traffic collisions, clothesline injury
- Internal trauma: endotracheal intubation (the most common cause in children)
Other acquired causes include iatrogenic (e.g. cricothyroidotomy, an emergency procedure to establish an airway), infection, neoplasm and granulomatous conditions (e.g. sarcoidosis, granulomatosis with polyangiitis).
Congenital subglottic stenosis is rare (e.g. secondary to Pallister-Killian syndrome).
Pathophysiology
The pathophysiology of subglottic stenosis depends on the underlying cause.
For example, in endotracheal intubation (a traumatic cause of subglottic stenosis), the inflated endotracheal tube balloon causes pressure necrosis, ischaemia and ulceration of the mucosa. Subsequent scarring then causes circumferential stenosis of the subglottis.
In idiopathic subglottic stenosis, there is usually a circumferential narrowing within the cricoid cartilage, and oestrogen has been implicated in its causation.2
Clinical features
History
In congenital subglottic stenosis, the symptoms that would typically manifest themselves at birth include:
- Accessory muscles of respiration
- Demonstrative air hunger
- Difficulty in breathing (dyspnoea)
- Biphasic stridor
- Involvement of vocal cords will produce hoarseness, aphonia and an abnormal cry
In acquired subglottic stenosis, there is progressively worsening shortness of breath, which could become biphasic stridor as narrowing progresses.
Clinical examination
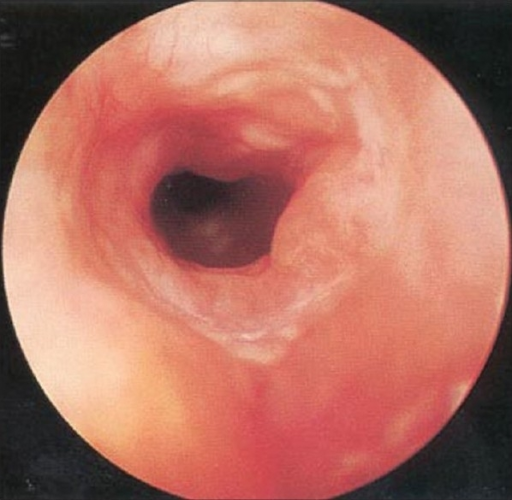
In the first instance, flexible fibreoptic endoscopy can visualise the upper airway, sometimes giving a view of the subglottis.
However, rigid airway endoscopy is the gold standard for visualising and sizing subglottic stenosis, as well as visualising synchronous airway pathology.
Myer-Cotton grading
The Myer-Cotton grading scale classifies subglottic stenosis depending on its’ severity.
It ranges from grade 1 (<50% stenosed), grade 2 (51-70%), grade 3 (71-99%) and grade 4 (complete obstruction).3
Investigations
Blood tests can be taken to exclude vasculitis as a cause (ANCA – granulomatosis with polyangiitis).
Cross-sectional imaging (CT/MRI) can help define the length of the stenosis and rule out alternative causes (e.g. external compression).
Rigid airway endoscopy is used for direct visualisation and biopsy of the stenosis.
Pulmonary function tests (PFTs) can be used to monitor a patient’s progress.
Management
Immediate management
Congenital stenosis causing airway compromise may be managed with a tracheostomy to provide a safe airway before definitive management.
Medical management
It is important to control any gastroesophageal reflux which can exacerbate subglottic stenosis.
Surgical management
Various surgical techniques are used in the management of subglottic stenosis. As mentioned previously, a tracheostomy may be required in the acute setting.
Endoscopic management can use a combination of radial incisions into the stenosis with dilatation (rigid or balloon) +/- intralesional steroid injection +/- stent placement.
Radiofrequency coblation is usually a single intervention enabling precise resection for subglottic stenosis and causing little thermal damage.4
Open neck surgery in the form of laryngotracheal reconstruction, possibly facilitated by balloon dilatation with stenting is another surgical option.5
Treatment is tailored to the individual, and many patients require repeat operations when the stenosis worsens.
Follow-up
Endoscopic dilatation requires frequent re-assessment to monitor re-stenosis. The frequency depends on the patient’s symptoms and disease progression.
Complications
Major surgery involving anaesthesia carries the general risks of bleeding, infection, thrombo-embolism and failure to improve the situation.
Specific complications include damage to surrounding structures at open surgery (e.g. recurrent laryngeal nerves, surgical emphysema, re-stenosis and injury to lips, gums, teeth and jaw with transoral endoscopic procedures).
Overall, a 25% rate of restenosis has been reported.6
Key points
- Narrowing of the subglottis can cause airway compromise
- The most frequent cause of subglottic stenosis is trauma secondary to intubation
- The Myer-Cotton grading scale is used to classify the severity
- Rigid airway endoscopy is the gold standard to visualise and size a subglottic stenosis
- Tracheostomy may be indicated in the acute setting if the airway is compromised
Reviewer
Mr Elliot Heward
ST6 ENT Surgeon
North West Region
Editor
Dr Chris Jefferies
References
- Antonio D’Andrilli, Federico Venuta, Erino Angelo Rendina. Subglottic tracheal stenosis. J Thorac Dis. 2016 Mar; 8(Suppl 2):S140-S147
- Aravena C, Almeida FA, Mukhopadhyay S, Ghosh S, Lorenz RR, Murthy SC, Mehta AC. Idiopathic subglottic stenosis: a review. J Thorac Dis. 2020 Mar;12(3):1100-1111
- Oshri Wasserzug, Ari DeRowe. Subglottic Stenosis: Current Concepts and Recent Advances. International Journal of Head and Neck Surgery. April-June 2016;7(2):97-103
- Huang J, Zhang Z, Zhang T. Tracheotomy-coblation for acquired subglottic tracheal stenosis: a case report. J Cardiothorac Surg. 2019 Jul 04;14(1):128
- Guarisco JL, Yang CJ. Balloon dilation in the management of severe airway stenosis in children and adolescents. J Pediatr Surg. 2013 Aug;48(8):1676-81
- Yamamoto K, Monnier P, Holtz F, Jaquet Y. Laryngotracheal reconstruction for pediatric glotto-subglottic stenosis. Int J Pediatr Otorhinolaryngol. 2014 Sep;78(9):1476-9
Image references
- Figure 1. Essam A Eid. Subglottic stenosis 04. License: [CC BY]
