

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Thyrotoxicosis is the clinical manifestation of excess thyroid hormone action at the tissue level due to inappropriately high circulating thyroid hormone concentrations.
Hyperthyroidism is a subset of thyrotoxicosis, referring specifically to excess thyroid hormone synthesis and secretion by the thyroid gland.
The most common cause of thyrotoxicosis is Graves’ disease, an autoimmune condition that results in excess endogenous production of thyroid hormones.1
Aetiology
Anatomy
The thyroid gland is located within the neck at the level of the C5-T1 vertebrae.
It consists of a central isthmus and two lobes, to the left and the right. The gland sits anterior to the trachea with the four parathyroid glands, which sit on the posterior surface of the thyroid gland.2
Physiology
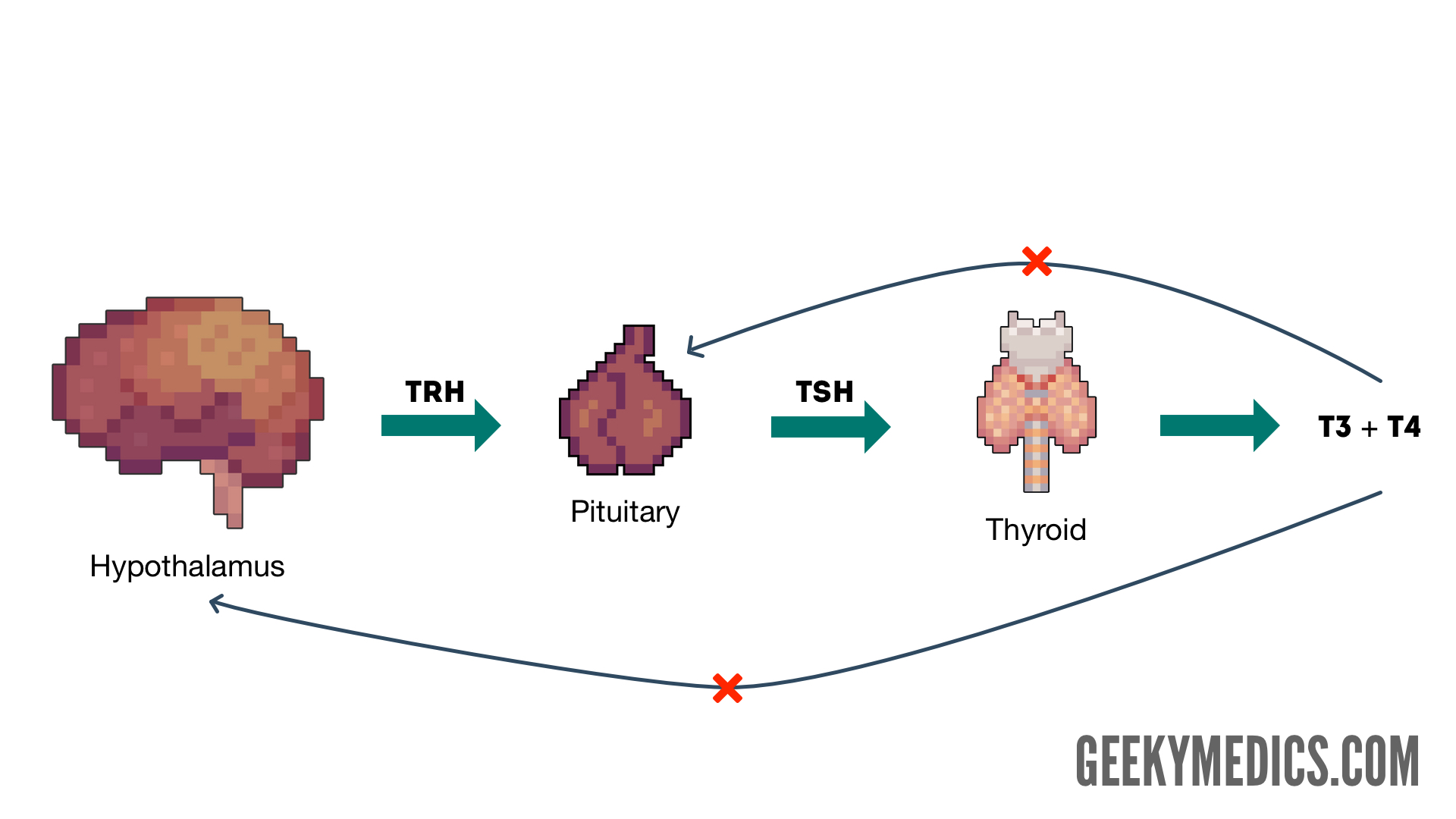
Thyroid hormones are produced from follicular cells of the thyroid gland. Production of these hormones is regulated via the hypothalamic-pituitary-thyroid (HPT) axis (Figure 1).
Thyrotropin-releasing hormone (TRH) is released from the paraventricular nucleus of the hypothalamus. TRH binds to pituitary receptors and causes the production of thyroid-stimulating hormone (TSH) from pituitary cells known as thyrotrophs.
TSH subsequently binds to receptors on the thyroid gland and causes the production of thyroid hormones from the thyroid follicular cells. These hormones are triiodothyronine (T3) and thyroxine (T4).
The HPT axis is regulated via negative feedback, at the level of the hypothalamus and the pituitary.
Excess concentrations of thyroid hormones feedback to both the hypothalamus and the pituitary to cause a reduction in both TRH and TSH production. This decreases the rate of thyroid hormone production via the HPT axis. This physiological regulation of the HPT axis is lost in thyrotoxicosis.3
T4 is the main hormone produced from the thyroid gland, alongside smaller amounts of T3. The majority of T4 is then converted to T3 when it reaches the target tissue (this is the most active form of the hormone).4
Thyroid hormones have a wide range of functions including influencing the basal metabolic rate (the rate of cellular oxidative phosphorylation).
Increased thyroid hormone concentration (seen in thyrotoxicosis) increases the basal metabolic rate. Thyroid hormones also have a key role in physiological growth, including fetal growth (thyroid hormones mediate the growth of neuronal and dendritic cells within the fetal central nervous system) and paediatric growth (thyroid hormones stimulate the expression of the pituitary growth hormone).5
Causes of thyrotoxicosis
Graves’ disease
Graves’ disease is the most common cause of thyrotoxicosis and hyperthyroidism. This is an autoimmune condition mediated via anti-TSH-Receptor (anti-TSHR) autoantibodies.
These autoantibodies bind to TSH-receptors on the thyroid gland and stimulate increased production of T3 and T4 from the thyroid gland, resulting in thyrotoxicosis.
Thyroxine receptors in the pituitary gland are activated by the excess hormone, resulting in the suppression of TSH release due to negative feedback. The result is very high levels of circulating thyroid hormones and a low TSH level.
The prevalence of Graves’ disease in the UK is 0.5%, typically presenting in patients between the ages of 40 and 60, and is much more common in female patients. Graves’ disease is also strongly associated with other auto-immune conditions including type 1 diabetes mellitus, Addison’s disease and vitiligo.4
Toxic multinodular goitre
Toxic multinodular goitre (TMG) is caused by the development of physiologically active nodules on the thyroid gland, which are capable of secreting thyroid hormones. These nodules are not responsive to circulating TSH concentrations and so, eventually cause thyrotoxicosis.
TMG is the second commonest cause of hyperthyroidism and most commonly affects older patients. Thyrotoxicosis due to a toxic multinodular goitre typically has a more insidious onset, in comparison to Graves’ disease.6
Iodine excess
Excess serum iodine concentrations can also cause thyrotoxicosis. This is because thyroid hormone production is dependent upon iodine, so increased serum iodine concentrations allow increased production of the hormones.
Iodine excess can occur following the use of contrast media for imaging modalities or via the contamination of food.1
Iatrogenic
Iatrogenic causes of thyrotoxicosis include the drugs amiodarone and levothyroxine.
Amiodarone contains iodine and increases iodine levels, increasing follicular thyroid hormone production. Levothyroxine is used in the management of hypothyroidism where there is a deficit. Overuse of this drug can cause an inappropriately increased serum hormone concentration.1
Viral infection
Viral infections can predispose to a phenomenon known as ‘subacute De Quervain’s thyroiditis’. This can cause a transient rise in thyroid hormone production due to inflammation of the thyroid gland and subsequent excessive excretion of thyroid hormones into the circulation. subacute De Quervain’s thyroiditis presents with a painful lump in the neck, most commonly between the ages of 20-50.4
Patients may subsequently develop hypothyroidism if the thyroid gland tissue is damaged by the inflammation.
Postpartum thyroiditis
Postpartum thyroiditis presents with a transient acute phase of thyrotoxicosis, followed by a period of hypothyroidism. This can occur 2 – 6 months following birth or miscarriage.7
Clinical features
Thyrotoxicosis presents with a wide range of clinical features due to the overall increased basal metabolic rate.
History
Typical symptoms of thyrotoxicosis include:
- Recent unintended weight loss
- Increased appetite
- Diarrhoea
- Heat intolerance (patients may appear underdressed for the weather)
- Over-activity and restlessness
- Tremor
- Palpitations
- Irritability
- Muscle weakness
- Loss of libido
- Oligomenorrhoea
Other important areas to cover in the history include:
- Past medical history: autoimmune conditions (Graves’ disease) or recent viral infection (De Quervain’s thyroiditis)
- Family history: family history of Graves’ disease
- Medication history: use of amiodarone, levothyroxine, or recent use of contrast media
- Obstetric history: recent pregnancy or miscarriage
Clinical examination
A thyroid status examination should be performed in all patients presenting with symptoms suggestive of thyrotoxicosis.
Clinical features of thyrotoxicosis may include:1
- Thin and brittle hair
- Warm and moist skin
- Irregular or fast heart rate
- Fine tremor
- Brisk reflexes
- Palmar erythema
- Lid lag and lid retraction
- Goitre (enlargement of the neck due to an enlarged thyroid gland)
Graves’ disease
There are some clinical features of thyrotoxicosis which are specific to Graves’ disease, due to the presence of the anti-TSHR autoantibodies.
Clinical features of Graves’ disease may include:4,8
- Thyroid eye disease (Graves’ ophthalmopathy): conjunctival injection, aching at the back of the eye, diplopia, gradual proptosis (exophthalmos), lid retraction, lid lag, chemosis (oedema of the eye)
- Thyroid acropachy: clubbing or swelling of the digits
- Pretibial myxoedema: oedema of the pretibial portion of the leg (just above the lateral malleolus)



Investigations
Thyroid function tests
The key laboratory investigation for the diagnosis of any thyroid condition is thyroid function tests (TFTs) which include serum levels of TSH, T3 and T4.
In most cases of thyrotoxicosis, the pattern of TFTs will reflect an increased production of thyroid hormones from the thyroid gland and a decreased production of pituitary TSH.
This is because the HPT axis will attempt to correct the excess thyroid hormone production via negative feedback:
- Increased T3 and T4
- Decreased TSH
If thyrotoxicosis is due to a rarer pituitary cause, then there will be an increased production of pituitary TSH, causing the increased production of thyroid hormones. The pattern of TFT results will be as follows:9
- Increased T3 and T4
- Increased TSH
See the Geeky Medics guide for a more detailed overview of thyroid function test interpretation.
Autoantibodies
The presence of thyroid autoantibodies suggests there is an underlying autoimmune disease causing thyrotoxicosis. The presence of anti-TSHR antibodies is highly suggestive of Graves’ disease.10
Other autoantibodies suggestive of autoimmune thyroid disease include anti-thyroid-peroxidase (anti-TPO) antibodies and anti-thyroglobulin (anti-Tg) antibodies. These are non-specific and can be present in autoimmune causes of both hyperthyroidism (Graves’ disease) and hypothyroidism (Hashimotos’ disease).4
Imaging
Doppler ultrasound may be used to image the thyroid gland, to confirm the presence of goitre and identify nodules.11
Management
Beta-blockers
Beta-blockers (commonly propranolol) are indicated in the management of thyrotoxicosis to provide symptomatic relief from the typical adrenergic symptoms (palpitations, tachycardia, tremor).4,12
Block and replace
The block and replace management regime is commonly used for the management of hyperthyroidism in adults and is the first-line management option for hyperthyroidism in children.
Block and replace involves blocking the excess thyroid hormone production from the thyroid gland and replacing this with the correct concentration of exogenous thyroid hormones.
Carbimazole is used to block thyroid hormone production and levothyroxine is used to replace thyroid hormones (these medications are administered simultaneously). Patients require ongoing monitoring of their TFTs and their FBC (due to the risk of agranulocytosis associated with carbimazole).
In most patients with Graves’ disease, a block and replace management regime can induce remission.12
Radioiodine
Radioiodine is a definitive management option for Graves’ disease and toxic multinodular goitre.
If radioiodine is deemed unsuitable for patients with Graves’ disease (e.g. due to pregnancy or malignancy), block and replace therapy is typically used as a second-line management option.
If radioiodine is deemed unsuitable for patients with a toxic multinodular goitre, thyroid surgery is used as a second-line management option.
Radioiodine can also be used second-line in patients with hyperthyroidism in whom block and replace has been unsuccessful.2
With radioactive iodine, measures must be taken following treatment to prevent any harm coming to those in close contact with the patient. Patients must be advised against prolonged contact with children (including their own) and pregnant women.
Female patients must also be advised against becoming pregnant within the next six months following treatment and male patients must be advised against fathering children for the next four months following treatment.12
Surgery
Thyroidectomy (complete removal of the thyroid gland) may be considered for the management of hyperthyroidism.
Thyroidectomy is indicated in cases of thyroid malignancy, or where a thyroid goitre is causing compression of surrounding structures. Thyroidectomy may also be considered if other treatment options are unsuitable or unsuccessful.12
Removal of the thyroid gland will result in a lack of circulating thyroid hormones in these patients. Therefore, they will need to be started on long term thyroid hormone replacement, most commonly levothyroxine.4
Complications
Thyroid storm
A serious complication of thyrotoxicosis is the onset of a thyroid storm, which involves excessive adrenergic activity secondary to thyrotoxicosis.
Clinical features of a thyroid storm may include:13
- Palpitations
- Tachycardia (often greater than 140 beats per minute)
- Tremor
- Nausea and vomiting
- Abdominal pain
- Reduced level of consciousness
- Confusion/agitation
- Seizures
Thyroid storm is associated with high mortality.
Cardiac complications
Cardiac complications of thyrotoxicosis include:4
- Atrial fibrillation: can be seen in up to 10-25% of patients. These patients require management of their hyperthyroidism as previously described as well as rate control (e.g. beta-blocker) and anticoagulation (e.g. Warfarin or Apixaban).
- Heart failure: this is more prevalent in elderly patients with hyperthyroidism, secondary to cardiomyopathy occurring in long-term thyrotoxicosis.
- Angina: should be considered in hyperthyroid patients presenting with exertional chest pain.
Graves’ ophthalmopathy
It is important to inform patients of the complications of Graves’ ophthalmopathy. In some instances, this can also cause deterioration of visual acuity if the optic nerve is affected.14
Key points
- Thyrotoxicosis is the clinical manifestation of excess thyroid hormone action at the tissue level due to inappropriately high circulating thyroid hormone concentrations.
- Hyperthyroidism is a subset of thyrotoxicosis, referring specifically to excess thyroid hormone synthesis and secretion by the thyroid gland.
- Thyroid hormone production is regulated via the hypothalamic-pituitary-thyroid (HPT) axis.
- Common causes of thyrotoxicosis include Graves’ disease and toxic multinodular goitre.
- Clinical features of thyrotoxicosis occur due to an abnormally increased basal metabolic rate.
- Clinical features specific to Graves’ disease include thyroid eye disease, thyroid acropachy and pretibial myxoedema.
- Thyroid function tests and autoantibody status can allow the underlying cause of thyrotoxicosis to be established.
- Beta-blockers (e.g. propranolol) are used to manage the adrenergic clinical features of thyrotoxicosis (e.g. tachycardia, tremor).
- First-line pharmacological management of thyrotoxicosis involves the use of a block (carbimazole) and replace (levothyroxine) regime.
- Other management options include radioiodine and thyroidectomy.
Reviewer
Dr Peter King
Reader in Molecular Endocrinology
Editor
Dr Chris Jefferies
References
Text references
- Parveen K, Michael C. Kumar and Clark’s Clinical Medicine. 9 ed. London: Elsevier; 2017.
- Moore K, Dalley A, Agur A. Clinically Oriented Anatomy. 7 ed: Lippincott Williams and Wilkins 2013. 1168 p.
- Rhoades R, Bell D. Medical Physiology. 4 ed. Philadelphia: Lippincott Williams & Wilkins 2013. p. 621-8.
- Wilkinson I, Raine T, Wiles K, Goodhart A, Hall C, O’Neil H. Oxford Handbook of Clinical Medicine. 10 ed. Oxford: Oxford University Press; 2017.
- Kim HY, Mohan S. Role and Mechanisms of Actions of Thyroid Hormone on the Skeletal Development. Bone Res. 2013;1(2):146-61.
- BMJ Best Practice. Toxic multinodular goitre. 2019. Available from: [LINK].
- NICE CKS. Hyperthyroidism. 2020. Available from: [LINK].
- Jadidi J, Sigari M, Efendizade A, Grigorian A, Lehto SA, Kolla S. Thyroid acropachy: A rare skeletal manifestation of autoimmune thyroid disease. Radiol Case Rep. 2019;14(8):917-9.
- Starr O, Tidy C. Thyroid Function Tests. 2020. Available from: [LINK].
- BMJ Best Practice. Graves’ disease. 2020. Available from: [LINK].
- NICE. Hyperthyroidism: Diagnosis. 2020. Available from: [LINK].
- NICE. Hyperthyroidism: Management. 2020. Available from: [LINK].
- Newson L, Bonsall A. Hyperthyroid Crisis (Thyrotoxic storm). 2015. Available from: [LINK].
- Foundation BT. Thyroid Eye Disease. 2019. Available from: [LINK].
Image references
- Figure 1. Geeky Medics. The hypothalamic-pituitary-thyroid (HPT) axis.
- Figure 2. Jonathan Trobe, M.D. Thyroid eye disease. License: [CC-BY]. Available from: [LINK]
- Figure 3. Herbert L. Fred, MD and Hendrik A. van Dijk. Thyroid acropachy. License: [CC-BY]. Available from: [LINK]
- Figure 4. Herbert L. Fred, MD and Hendrik A. van Dijk. Pretibial myxoedema. License: [CC-BY]. Available from: [LINK]
