

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Compartment syndrome is a surgical emergency characterised by increased pressure within a closed space.
It is usually encountered in limb injuries such as tibial or forearm fractures, crush injuries, reperfusion injury or restrictive casts and dressings. Compartment syndrome requires urgent intervention as delay can lead to necrosis within the affected myofascial compartment and permanent damage.
The upper and lower limbs are most commonly affected. However, compartment syndrome can also affect the abdomen or any other muscle compartment.
Aetiology
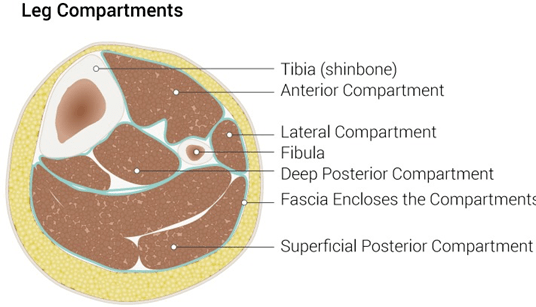
The limbs are divided into various compartments. Within each compartment, there are muscles, blood vessels and nerves. Each compartment is covered by a tough membrane called fascia which is resistant to expansion and stretching. The normal pressure within the limbs is between 12-18mmHg. 1
Blood flows from a high-pressure arterial system to a low-pressure venous system and a homeostatic pressure gradient is maintained. When there is injury, bleeding, swelling or overall disruption to the pressure gradient, the flow is disrupted and affects the capillary perfusion pressure.
This causes the build-up and subsequent extravasation of fluid out of the capillaries which further increases the pressure within a closed myofascial compartment.
Furthermore, the distribution of oxygen and nutrients and the removal of carbon dioxide is disrupted. This leads to muscle ischaemia and necrosis.
Risk factors
Risk factors for compartment syndrome include:
- Major surgical procedures (e.g. orthopaedic repair, post-embolectomy, post-laparotomy)
- Blunt trauma
- Burns
- Reperfusion injury
- Crush injury
- Fractures: closed or open
- Tight casts
- Ongoing intra-abdominal bleeding
- Penetrating trauma (e.g. vascular injury)
- Malignancy
Clinical features
History
Typical symptoms of compartment syndrome include:
- Disproportionate pain that increases with time
- Paraesthesia
- Paresis
At later stages, patients may also develop:4
- Muscle contracture
- Complete loss of sensation
- Limb pallor
Other important areas to cover in the history include:
- The timing of the injury and when the patient is assessed
- The extent of the pain
- Whether any analgesia has been given (as this can mask the onset of acute compartment syndrome)
Clinical examination
Typical clinical findings associated with compartment syndrome include:4,7
- Pain out of proportion to the clinical findings, particularly during passive stretching (passive dorsiflexion)
- The limb may be tense on palpation and difficult to mobilise
- Numbness and paralysis (later stages)
Investigations
While compartment syndrome is diagnosed clinically, intra-compartmental pressure monitoring using a needle connected to a transducer can be performed. This is especially useful in unconscious patients. 8
A difference between the diastolic blood pressure and the compartment pressure of less than 30 mmHg implies an increased risk of compartment syndrome.
An absolute intra-compartmental pressure of > 40 mmHg with clinical signs is diagnostic of acute compartment syndrome. 5
Management
Surgical decompression through an emergency fasciotomy is the mainstay of treatment. This involves opening the fascial compartment affected to relieve the pressure within the compartment. This should be done within one hour of diagnosis.
Initial management of compartment syndrome should also include:8
- Removal of any circumferential casts or bandages
- Maintenance of blood pressure
Abdominal compartment syndrome
Compartment syndrome can also occur in the abdomen, which has a normal pressure of 0-5mmHg. 3
The mechanism is the same; the abdominal wall can expand to a certain extent beyond which compliance is not possible. Abdominal compartment syndrome can lead to multi-organ failure and death. Causes include retroperitoneal bleeding, reperfusion injury and bowel obstruction.
Typical diagnostic criteria include an intra-abdominal pressure of >20mmHg with evidence of multi-organ failure. 3
The gold standard for monitoring intra-abdominal pressure is via a transducer connected to a urinary bladder catheter. 8
Abdominal compartment syndrome is treated by surgical decompression in the form of a laparotomy.
Complications
If prompt intervention is not performed, patients may develop irreversible neurovascular damage of the affected limb.
Other complications of compartment syndrome include:6
- Neurological dysfunction
- Muscle/joint contracture
- Infection
- Amputation
- Long term disability
Key points
- Compartment syndrome is a surgical emergency characterised by increased pressure within a closed space.
- Causes include limb injuries such as tibial or forearm fractures, crush injuries, reperfusion injuries or in the context of restrictive casts.
- Pain out of proportion to the clinical findings, particularly during passive movement of the affected limb is typical of compartment syndrome.
- Management involves urgent surgical intervention in the form of a fasciotomy to relieve the pressure within the compartment.
- Prognosis is generally good if fasciotomy is performed within one hour of development.
- Complications of compartment syndrome include neurovascular damage, muscle/joint contracture, infection, amputation and long term disability.
Reviewer
Ms Manal Ahmad
ST3 in Vascular/General Surgery
Editor
Dr Chris Jefferies
References
- McQueen MM, Duckworth AD. “The diagnosis of acute compartment syndrome: a review.” European Journal of Trauma and Emergency Surgery. 2012. Available from: [LINK]
- Palmer B. Leg compartments image. License: [CC BY]
- Morgan B. Intra-abdominal pressure monitoring. 1999. Available from: [LINK].
- Henry MM, Thompson JN. Clinical Surgery. Published in 2012.
- British Orthopaedic Association Standards for Trauma. Diagnosis and Management of Compartment Syndrome of the Limbs. 2014. Available from: [LINK]
- NICE Guidelines. Fractures (complex): assessment and management Complex fractures: assessment and management of complex fractures NICE Guideline NG37 Methods, evidence and recommendations 2016. Available from: [LINK]
- Offiah G, Hill A. Compartment Syndrome. RCSI Handbook of Clinical Surgery for Finals, fourth edition. 2020.
- Stehr W. The Mont Reid Surgical Handbook, sixth edition. 2008.
