

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Triage is a key principle in prioritising the treatment of patients, especially in situations where resources are limited. This is especially important in a major incident or mass casualty situation when the number of patients is likely to significantly exceed the number of clinicians initially available.1
Triage tools designed for major incidents and mass casualty situations are well established in the NHS and emergency services. For many years, UK ambulance services have commonly utilised a Sieve and Sort triage model.2
However, research identified that it had shortcomings. A review by NHS England has resulted in the development of two new triage tools: Ten Second Triage and the NHS Major Incident Triage Tool.
These models classify patients into one of five groups:6
- Priority one (immediate): patients in need of life-saving interventions and requiring immediate treatment within the hour
- Priority two (urgent): patients who are unwell but with a degree of stability and comparatively normal physiology. Typically, they will require treatment/interventions within two to four hours
- Priority three (delayed): referred to as the ‘walking wounded’, these patients can ambulate to a treatment area and are deemed safe to have a treatment delay of four hours or more
- Dead: patients who have been assessed by a clinician and found not to be breathing
- Not breathing: patients who have been triaged by a non-clinician and found not to be breathing
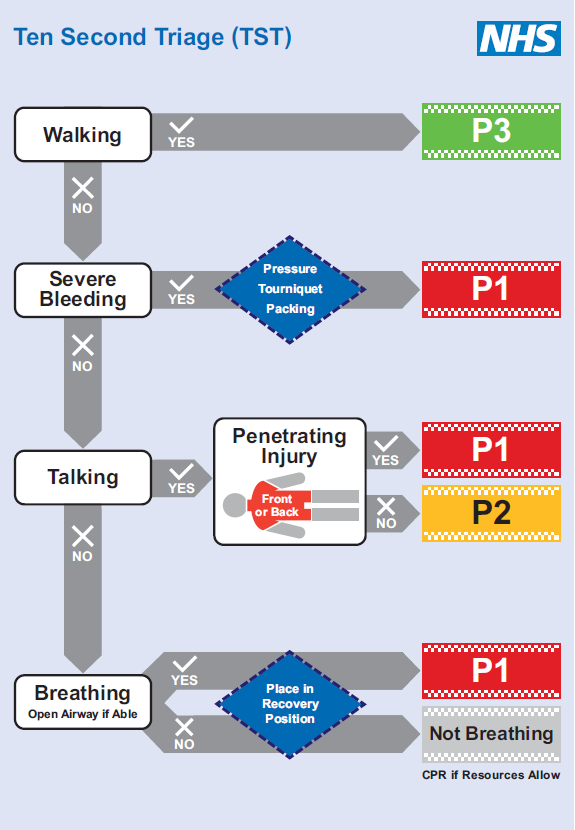
Ten Second Triage
The ability for responders from all emergency services to collaborate and prioritise patients, potentially before the arrival of NHS clinicians, is important to improve the timeliness and outcomes of care.3
Ten Second Triage (TST) has been designed as a preliminary triage tool to be used by any responder at a major incident, such as police officers or firefighters.
TST is designed as a quick and simple triage method, following a simple algorithm of whether the patient is walking, talking, breathing or not breathing, in addition to looking for the presence of any central penetrating injury.
These features enable a basic end-organ assessment of cardiovascular status, allowing non-clinicians to rapidly identify the highest acuity patients in the early stages of an incident.1
It also prompts which lifesaving interventions should be initiated. TST labels patients as not breathing rather than dead, allowing for CPR to be considered depending on the circumstances.3
TST can also be performed by the first clinicians on scene to provide the initial categorisation of patients, with more detailed triage being undertaken once sufficient clinical resources have arrived.
The tool’s simplicity minimises cognitive burden, freeing bandwidth to enable responders to treat casualties in challenging circumstances.
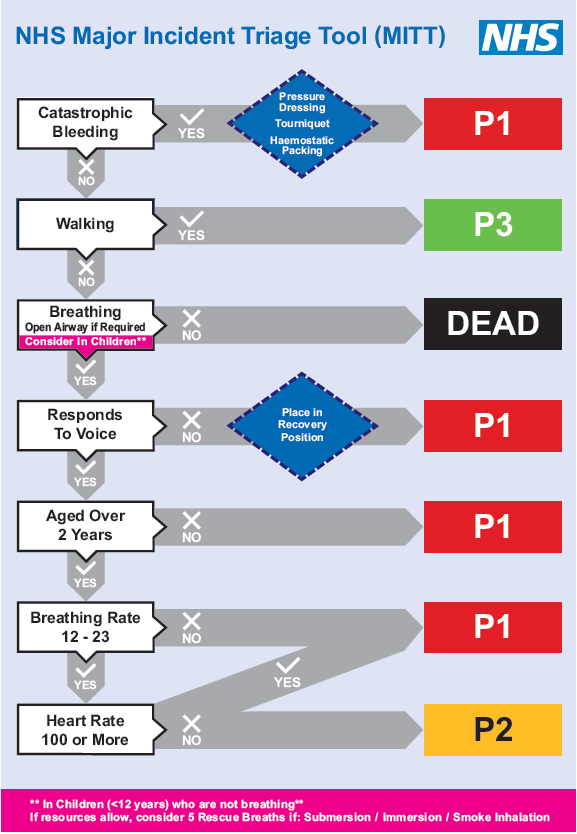
NHS Major Incident Triage Tool
Once sufficient clinical resources are present, a physiological clinical triage should be undertaken as soon as possible. The NHS Major Incident Triage Tool (MITT) has been designed to be used by clinicians as a comprehensive, reliable and reproducible triage of patients.
The MITT has an increased sensitivity and accuracy of high acuity patients compared to other triage tools. It is applicable for both adult and paediatric patients, with the addition of rescue breaths for paediatrics and the automatic categorisation of those under two years as priority one.3
Triaging patients
When undertaking triage, it can be best to complete this as a pair, with one assessing each patient and the other checking the findings against the tool and recording the category of the patient.
Progressing systematically and assessing one patient at a time is important to ensure all patients are included. A tally, and ideally the patients’ locations, should be maintained for reporting back to those managing the incident, allowing for subsequent clinical teams to be prioritised to the relevant patients.
The triage process should be undertaken swiftly, ideally limited to ten seconds for the preliminary assessment. Treatment should be restricted to brief attempts to control catastrophic haemorrhage, opening an airway or placement into the recovery position, as detailed in the triage tools.
Once the assessment has been undertaken and a triage category allocated, the patient should be provided with a visual indication of their category. Depending on the method used by your organisation and the resources available, this could include wristbands, tags, glowsticks or other improvised means.
References
- Vassallo, J., Cowburn, P., Park, C., Bull, D., Harris, S., Moran, C. G., & Smith, J. E. (2023). Ten second triage: A novel and pragmatic approach to major incident triage. Trauma, 14604086231156219.
- Vassallo, J., Moran, C. G., Cowburn, P., & Smith, J. (2022). New NHS prehospital major incident triage tool: from MIMMS to MITT. Emergency medicine journal.
- NHS England. Major incident triage tools. Available from: [LINK]
- NHS England. Ten Second Triage tool. [LINK]
- NHS England. NHS Major Incident Triage Tool. Available from: [LINK]
- RCEM Learning. Triage in mass casualty situations. Available from: [LINK]
