
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Intravenous cannulation and venepuncture are two of the most commonly performed clinical procedures for doctors and are performed daily in many medical and surgical rotations.
Despite the frequency in which you will perform these tasks, undertaking these procedures in patients with ‘difficult venous access’ can pose a significant challenge and area a much-feared task amongst foundation doctors (and their seniors!).
This handy guide will cover some top tips for gaining venous access in more challenging situations.
Before you begin
Before starting, make sure you are clear about the indication for the blood tests and which tests are required, or why intravenous access is needed. Specific infusions may require a particular rate and, therefore cannula size, (if in doubt, check with the nursing staff). One notable example is that to send a patient for a CT pulmonary angiogram (CTPA), they must have at least a 20G (pink) cannula.
Certain patient groups can be notoriously difficult to gain venous access from. These include those undergoing chemotherapy or renal replacement therapy and current or previous intravenous drug users.
Those who have undergone frequent venepuncture become sequentially more difficult due to calcification during the healing of the venous wall, which is a common issue in patients requiring prolonged hospitalisation.
With age, veins become more fragile due to the loss of collagen integrity. Those on blood thinners or with clotting disorders will bruise more easily, making further attempts to surrounding veins more difficult.
Needle phobia is common, particularly in younger patients and can also increase clinician anxiety! Ensure everyone is feeling as relaxed as possible. Ask relatives to step outside if this would be more appropriate, particularly if they are needle-phobic themselves.
Equipment
Venepuncture and cannulation equipment can vary across different hospitals, so when starting in a new hospital it is well worth becoming familiar with the equipment before approaching the patient’s bedside. Vacutainer bottles have the advantage of drawing liquid in through low pressure.
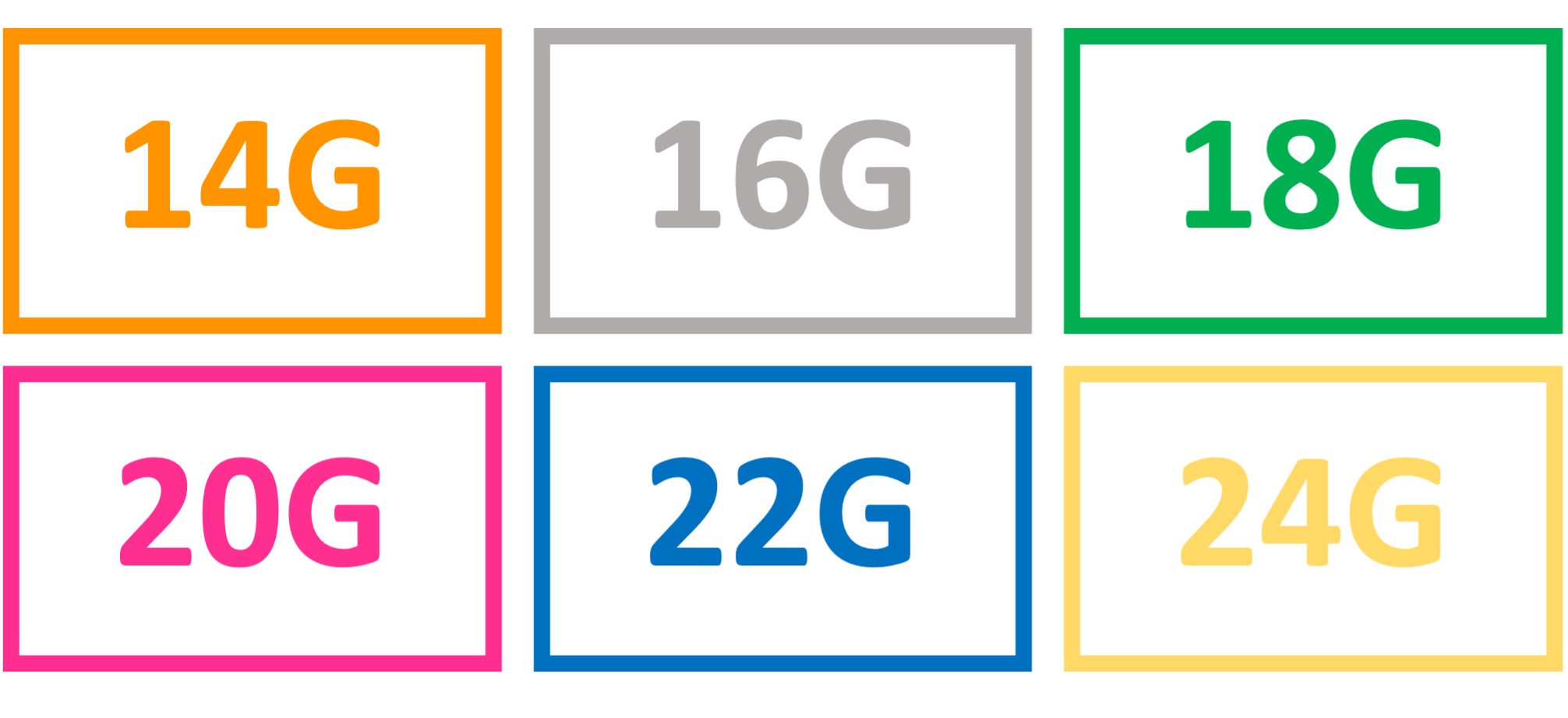
Cannulas come in a range of sizes from 14 – 24G for use in adults (remember, large gauge equals finer bore) and can be identified by the colour.
Larger gauge cannulas are more suitable for smaller veins. For venepuncture, opt for finer bore needles and butterfly needles.
Remember to check that the cannula will be large enough for the infusion (if in doubt, speak to the nursing staff). Smaller gauge cannulas enable more rapid fluid infusion, so they are preferable in acute situations such as trauma or when managing more unwell patients. Smaller bore cannula are preferable for delivering chemotherapy.
Smaller cannulas will also have shorter lengths, which can be helpful in patients with tortuous veins where there can be difficulty threading the cannula through.
If you anticipate the procedure will be difficult, prepare by taking adequate stocks of all the necessary equipment in your tray to avoid multiple runs back to the stock cupboard.
Consider the priority of the tests you wish to run and the order you will fill blood bottles.
Consider the minimum fill level required for the laboratory to process the sample (particularly for coagulation profile).
It can also be worth pre-empting other tests the patients might require during their admission, particularly if these require different colour blood bottles (ie. coagulation profile, group and save), to minimise the future need for venepuncture attempts. However, remember that biochemistry samples must always be taken before FBC samples as EDTA contamination can cause erroneous electrolyte readings: “U+Es before FBCs”
Combining cannulation with venepuncture
To minimise needle attempts, blood for analysis can be taken out of a cannula tube, but only immediately after insertion and not after being flushed (make sure you take either an adaptor or a syringe and needle).
Getting set up
Ensure you are in a comfortable position before starting. Make sure you have adequate lighting, particularly on night shifts. In many wards, mobile lamps at the head of the bed can be positioned to improve your lighting.
Use gravity as much as possible and ensure the vein you aim for is below the level of the patient’s heart. If the patient is unlikely to be able to comply with remaining still during the procedure, take a second pair of hands to help position the patient; remember to assess capacity if applicable
Choosing a vein
When locating a suitable vein, feeling is more informative than sight: a vein you can palpate is a better option than one you can see on the skin surface.
Veins should feel ‘bouncy’ to touch. Consider the anatomy of the vein and its path below the skin, straighter veins are preferable, especially for cannulation. Avoid obvious crossing points where veins coalesce. Avoid veins that feel hard and calcified or those recently used for venepuncture.
Ask the patient if a location has been more likely to yield success in the past, and consider using that site (this can be an amazingly effective yet simple approach).
Using veins in the lower limbs is associated with an increased risk of phlebitis and venous thrombosis, so should only be tried if all options in the upper limbs have been exhausted (especially for cannulation as this will limit the patient’s mobility during the infusion).
Top tips and handy hints
Good technique is fundamental in more difficult cases. For more information, see the Geeky Medics guides to venepuncture and cannulation.
Needle angle
Pay particular consideration to the angle of the cannula to the skin. Consider the course and trajectory of the vein and aim to follow it’s path with the needle under the skin surface.
Anchor mobile veins by applying light tension to the skin around the insertion site with your dominant hand, particularly for more peripheral veins (ie. dorsum of the hand) and in elderly patients.
Tourniquet
The tourniquet should be sufficiently tight to impede venous return (equally ensure it is not too tight to impede arterial flow and should not be left on for long durations- generally not more than ~2 minutes).
Other considerations
Ensure the patient is well hydrated and the target area is warm. Warm compresses and heat pads can be used if available. Light tapping or rubbing can help dilate veins, but avoid anything other than light pressure.
Movement, typically opening and clenching of the hand, increases blood flow to the arm. However, this can increase the risk of haemolysis, so advise the patient to do this gently.
Secure cannulas
Ensure cannulas are tightly secured with dressings and tape. A simple bandage can be wrapped around the cannula for extra safekeeping and can be particularly handy for avoiding loose bunges and wiring getting caught, particularly in patients with delirium or dementia.
Consider sticking the label with the date of cannula insertion over any dressings so it is visible.
Sharps
If there have been multiple attempts, remember to ensure all sharps have been correctly disposed of.
Alternatives
The general rule is for a maximum of three attempts at the procedure unless the patient agrees with further attempts or you realistically expect to be successful in trying again.
Senior support
Let your senior clinicians (and other juniors) know early if you are struggling. Nursing staff competent in cannulation can also be a great source of experience and expertise, particularly those in specialist areas (such as oncology).
Sometimes, another pair of eyes and a bit of luck is all that is required, and it is often appropriate to delegate to those of the same training grade as yourself.
For more difficult patients, your seniors may advise against too many attempts by junior team members as this can ultimately make their job harder when they come to try. Senior doctors will also have experience in ultrasound-guided venous access if you are unfamiliar with this technique. They will be grateful if you can save them time by locating the necessary equipment.
The most proficient and experienced doctors in the hospital for venous access are anaesthetists. However, they are likely to receive many requests for assistance from multiple specialities and may not be overwhelmingly compassionate or obliging to your requests for assistance.
Discuss with your seniors before contacting anaesthetics and make sure you are able to justify to them that this would make a significant difference to the patient’s management or how the blood test would provide vital clinical information.
Arterial stab
If gaining venous access is practically not feasible, arterial stab can provide an alternative method for obtaining a blood sample. Whilst this is less well tolerated and more painful for the patient, it may be necessary if there is an urgent clinical need and can be preferable to continuing unsuccessful repeat attempts at venipuncture.
In this situation, pre-warn the patient that arterial stab is more tender but explain the importance of the results the blood test will give or how it would alter clinical management.
Ultrasound guidance
Ultrasound can be used to identify and access veins for both cannulation and venepuncture in the most challenging situations, particularly where veins are too deep to feel. For more information, see the Geeky Medics beginners guide to ultrasound.
Lines and interosseous access
If peripheral venepuncture/cannulation is practically unfeasible or the patient requires regular intravenous therapy (e.g. chemotherapy), semi-permanent lines can be inserted, such as PICC lines.
These are usually arranged through the vascular access department; speak to your seniors first. In emergencies, intraosseous access (IO) can also be considered.
Planning venous access
If you are unsuccessful or a patient is particularly challenging to gain venous access from, it is worthwhile documenting this in the patient’s medical notes, particularly if they are likely to need repeat blood tests or intravenous treatments during the expected course of the admission.
Prolonged venepuncture draw can increase the risk of haemolysis and spurious results, so a record of this can help the results to be interpreted in the clinical context.
Highlight tricky patients to senior clinicians, so investigations can be planned to minimise venepuncture requirements where feasible and also to consider requesting lines.
References
- Royal United Hospitals Bath. Tube Guide and Recommended Order of Draw. Available from: [LINK]
- Gloucestershire Hospitals NHS Foundation Trust. Peripheral Venepuncture. Available from: [LINK]
