

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Benign breast disease accounts for a large proportion of diagnoses in women seeking assessment for breast-related pathology, with malignancy accounting for only three to six per cent of cases.
The clinical presentation of benign breast disease includes changes in the skin or nipple-areolar complex, increased nipple discharge, bloody discharge and palpable lumps, with the latter being most common.1
The key to establishing diagnoses safely and effectively is the triple assessment method which will be described in this article.1
Risk factors
Specific risk factors for benign breast lumps are not well documented as most studies focus on risk factors for malignant breast disease. However, the risk factors below have been found to increase the prevalence of both types of lumps.2
These risk factors include but are not limited to:
- Early pubarche and late menarche: starting puberty before the age of 12 years and starting menopause after the age of 55 years
- Dense breast with a high proportion of breast tissue
- Personal history of breast cancer or other breast conditions
- Previous irradiation to the area
- Obesity
- Hormonal treatment
- Nullparity or first pregnancy after the age of 30
- Never breastfeeding
- Alcohol
- Smoking
Triple assessment algorithm
Clinical examination
Inspection and palpation of the lump establishing location with respect to quadrants.
Other characteristics of a breast lump to assess include size, shape, consistency, symmetry, fluctuance and any overlying skin changes.
For more information, see the Geeky Medics guide to breast examination.
Radiological analysis
Ultrasound is the investigation of choice for patients under 35 years, whilst mammography is preferred for those over 35 years.
Histological/cytological analysis
Ultrasound-guided fine needle aspiration or core biopsy according to local guidelines is diagnostic.
Cystic lumps
Fluid-filled lumps should be aspirated under ultrasound guidance and sent to the appropriate department for analysis. If a residual mass is present, this should be biopsied and sent for histological analysis. Clear fluid is reassuring.3
Solid lumps
Aspiration of solid lumps is not ideal, is usually unsuccessful and increases the risk of tumour seeding. These lumps should be biopsied and sent for histological analysis to exclude malignancy.3
Fibroadenoma
Fibroadenomas are the most common cause of benign breast lumps. These usually present in patients younger than 30 but can occur up to menopause.
Overgrowth of collagenous mesenchyme of breast lobules causes fibroadenomatous changes. On breast examination, these are described as firm, smooth and mobile under the skin (hence the name “breast mice”).4
These lumps are painless and tend to occur in multiples. Broadly, a third of fibroadenomas regress after an initial assessment, a third continue to enlarge, and a third stay the same size.
Management of a fibroadenoma includes observation and reassurance. If diagnostic uncertainty, refer for an ultrasound scan (usually conclusive) ± fine needle aspiration.
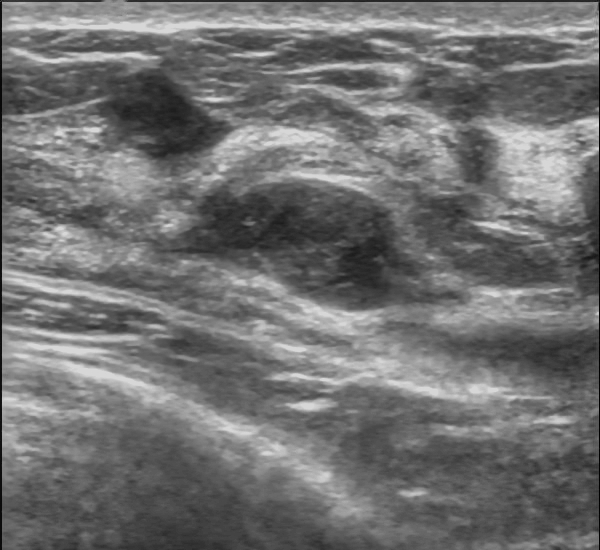
Imaging with ultrasound shows a well-circumscribed, round-to-ovoid, or macrolobulated mass with generally uniform hypoechogenicity (Figure 1). Surgical excision may be performed for large fibroadenomas.
Breast cysts
Breast cysts are common in patients over 35 years of age, especially if perimenopausal. These benign cysts are fluid-filled and round, being mobile on examination as they do not adhere to surrounding tissue. As opposed to fibroadenomas, these lumps are usually painful producing cyclical symptoms related to menses.4
The diagnosis of breast cysts is confirmed by aspiration (perform only if trained).
Infective mastitis/breast abscesses
Infection of the mammary ducts causes mastitis, which if left untreated leads to breast abscess formation. This is often associated with lactation, the most common causative organism being Staphylococcus aureus.
Breast abscesses are painful, immobile subcutaneous lumps, tethered to the overlying skin, demonstrating rubor (erythema) and calor (warm) of the involved area of skin compared to surrounding skin. Superficial erythema may not always be present. On palpation, tenderness is elicited, and the patient may also develop a fever.4
Antibiotics are the mainstay of treatment. Open incision and drainage or percutaneous drainage may be performed according to local guidelines if required.
Duct ectasia
Duct ectasia typically develops around menopause and is common in smokers. Mammary ducts become blocked by stagnant secretions.
Patients usually present with greenish nipple discharge, however, this may also be brown or bloody. Other signs include nipple retraction and a lump below or at the areolar complex. An ultrasound of the lump would confirm this diagnosis.
Usually, no treatment is needed apart from smoking cessation advice.5
Fat necrosis
Fat necrosis occurs after a traumatic injury to breast tissue. The trauma (which may be minor) leads to fibrosis and calcification which presents as immobile firm lumps at the area of injury. There may be associated bruising around the area.
No treatment is required once the diagnosis is confirmed following a triple assessment.5
Phyllodes tumour
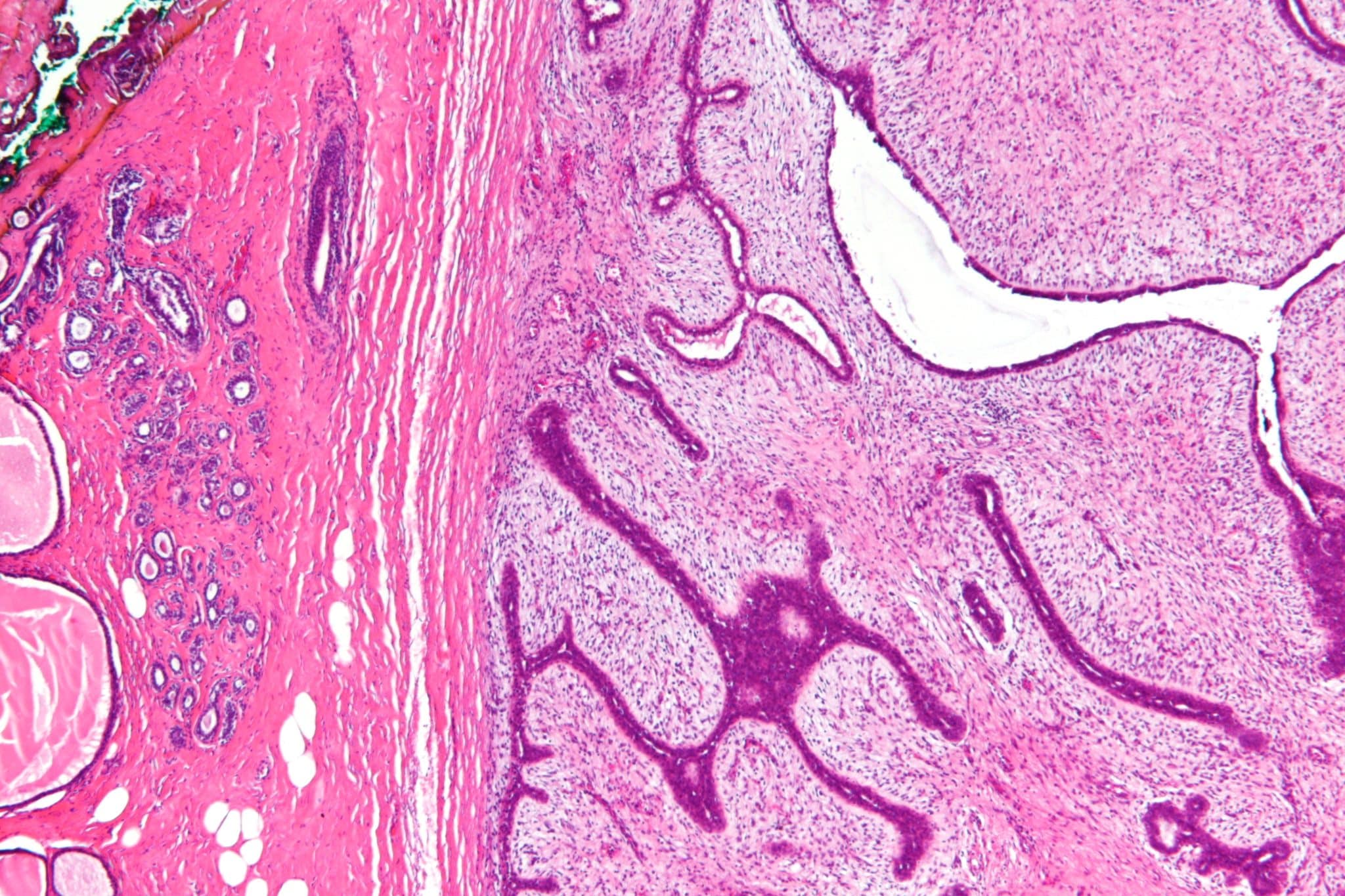
These are rare tumours that microscopically appear leaf-like in structure, with a high mitotic count. The majority of these tumours (70%) are benign and arise from the breast stroma.
If malignant, phyllodes tumours are classified as soft tissue sarcomas and metastasise primarily to the lungs. These tumours tend to occur in patients 40-50 years old. There is often a history of rapid growth of a discrete, rubbery breast lump, sometimes with accompanying pain from compression of normal surrounding breast tissue.
Phyllodes tumours are diagnosed following triple assessment. Management involves surgical excision with a 5mm rim of normal breast tissue to minimise local recurrence.6
Key points
- Breast lumps are a common finding in women of any age after puberty
- Most causes of a breast lump are benign
- All breast lumps should be assessed using the triple assessment method (clinical examination, radiological investigation and histological/cytological assessment)
- Fibroadenomas are the most common type of benign breast lump and usually occur in patients under the age of 30
- Breast cysts are common in patients over 35 years of age, especially if perimenopausal
- Duct ectasia typically develops around menopause and is common in smokers
- Fat necrosis occurs after a traumatic injury to breast tissue and no treatment is required once the diagnosis is confirmed
Reviewer
Mr. Kurt Lee Chircop M.D. (Melit.) MRCSI MSc
Plastic and Reconstructive Surgery Registrar
Editor
Dr Chris Jefferies
References
- Sharma, G.N., Dave, R., Sanadya, J., Sharma, P. and Sharma, K., 2010. Various types and management of breast cancer: an overview. Journal of advanced pharmaceutical technology & research, 1(2), p.109.
- Brinton, L.A., Vessey, M.P., Flavel, R. and Yeates, D., 1981. Risk factors for benign breast disease. American journal of epidemiology, 113(3), pp.203-214.
- Foulkes, R. and Gateley, C.A., 2010. Management of benign diseases of the breast. Surgery (Oxford), 28(3), pp.125-129.
- Santen, R.J., 2018. Benign breast disease in women. Endotext [Internet]. Available from: [LINK]
- Santen, R.J. and Mansel, R., 2005. Benign breast disorders. New England Journal of Medicine, 353(3), pp.275-285.
- Shaaban, M. and Barthelmes, L., 2017. Benign phyllodes tumours of the breast:(Over) treatment of margins–A literature review. European Journal of Surgical Oncology (EJSO), 43(7), pp.1186-1190.
Image references
- Figure 1. Nevit Dilmen. Fibroadenoma of the breast. Ultrasound image. License: [CC BY-SA]
- Figure 2. Nephron. Phyllodes tumour – low mag. License: [CC BY-SA]
