
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Carpal tunnel syndrome (CTS) is a collection of symptoms and signs caused by compression of the median nerve in the carpal tunnel at the wrist.
CTS is the most common compression neuropathy of the upper limb and is three times more common in women than men. The prevalence of CTS identified in European population studies varies from 1 to 7%, with peak incidence occurring in people aged 45-64 years.1
Aetiology
Reduction in the dimensions of the carpal tunnel or an increase in the volume of its contents produces elevated pressure, which causes ischaemia of the median nerve and impairs nerve condition.1
If pressure on the nerve persists it can lead to segmental demyelination. Nerve dysfunction may become irreversible if axonal injury secondary to prolonged ischaemia occurs.
Anatomy of the carpal tunnel
The carpal tunnel is an anatomical compartment or narrow passageway within the wrist. It allows several tendons and the median nerve to travel into the hand from the forearm. The carpal tunnel boundaries are:
- Roof: the transverse carpal ligament (flexor retinaculum).
- Radial carpal bones: the scaphoid tubercle and trapezium.
- Ulnar carpal bones: the hook of hamate and pisiform.
- Floor: carpal groove formed by the palmar aspect of the proximal carpal row.
Because these boundaries are very rigid, the carpal tunnel has little capacity to “stretch” or increase in size.2
The carpal tunnel contains 9 flexor tendons and the median nerve. The 9 flexor tendons are:
- Flexor pollicis longus
- Flexor digitorum profundus (x4)
- Flexor digitorum superficialis (x4)
The tendons within the carpal tunnel are surrounded by synovial sheaths, one of which envelops the flexor digitorum superficialis and profundus together and a separate sheath for the flexor pollicis longus.3

Anatomy of the median nerve
The median nerve gives off two major branches within the forearm:
- Anterior interosseous nerve: supplies motor function to the deep layer of muscles within the anterior forearm.
- Palmar cutaneous nerve: supplies sensation to the palm and skin over the thenar eminence. As it does not pass through the carpal tunnel, sensation is spared in CTS.
After giving off these two branches, the median nerve then travels into the carpal tunnel to gain access to the hand. It then divides into two terminal branches:
- Recurrent motor branch: supplies the median innervated muscles of the hand.
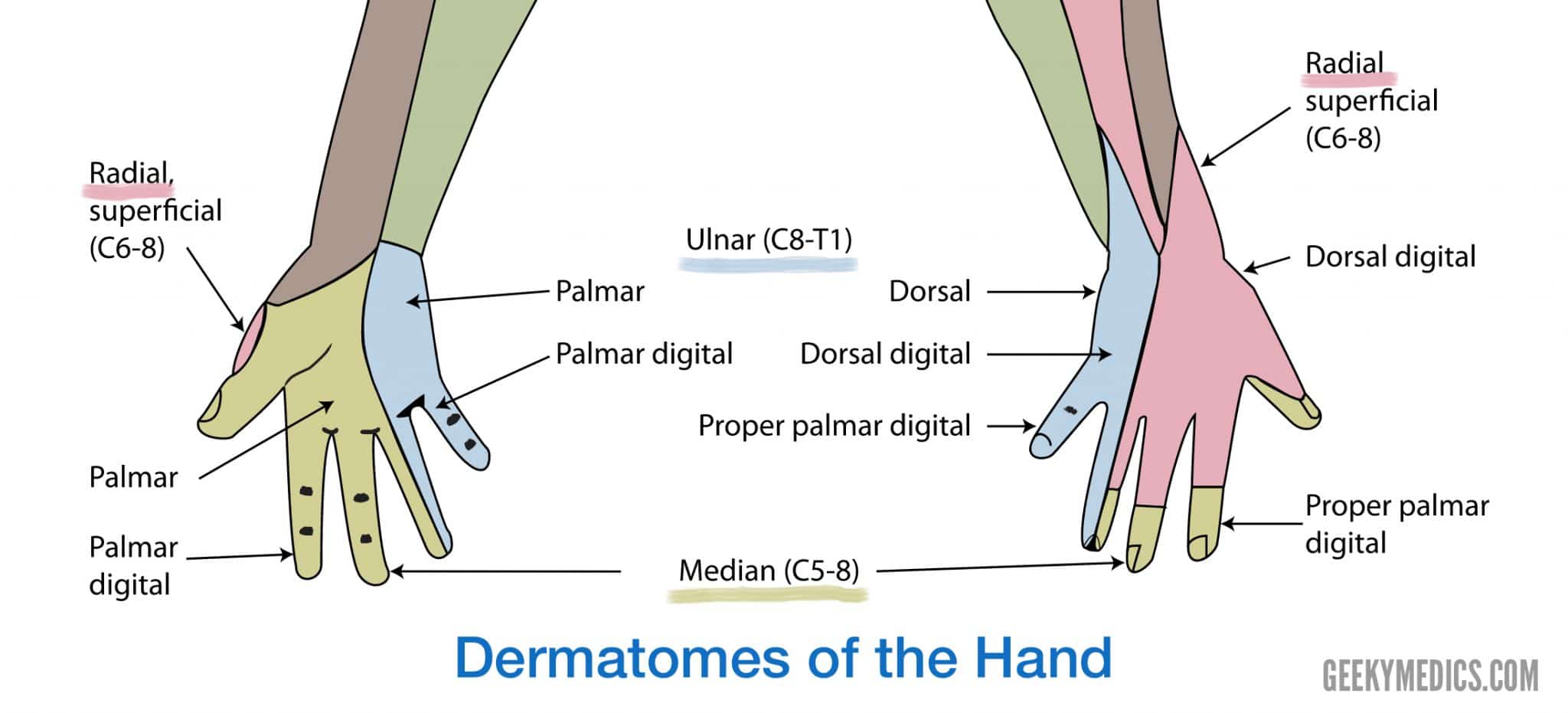
- Digital cutaneous branch: this supplies sensation to the lateral/radial three and a half digits (thumb, index, middle and radial half of the ring fingers).
Risk factors
In most cases, the cause of carpal tunnel syndrome is unknown (known as idiopathic CTS). However, anything that reduces the volume of the carpal tunnel or increases the pressure within it can potentially lead to symptoms of CTS.1
Table 1. Risk factors and causes of CTS
| Fluid retention | Inflammation of structures within/around the carpal tunnel | Space occupying lesions | Other conditions |
|
Pregnancy Menopause Obesity
|
Repetitive strain injury causing tendinopathy (overuse in jobs such as gardening, assembly line work and use of vibrational power tools) Inflammatory arthropathy (e.g. rheumatoid arthritis)
|
Ganglion cysts Osteophytes (in osteoarthritis)
Previous wrist fractures/ trauma may also mechanically reduce the space within the carpal tunnel
|
Diabetes mellitus Hypothyroidism Smoking
|
Clinical features
History
In cases of suspected CTS, a thorough history is required to differentiate CTS from other neuropathies.
Early diagnosis and treatment are important to avoid permanent damage to the median nerve.5
Patients with CTS typically present to primary care providers with a gradual onset of intermittent CTS symptoms. However, as the condition worsens, symptoms may occur more frequently or persist for longer periods of time.2
Typical symptoms of CTS include:
- Tingling, numbness or pain in the distribution of the median nerve (the thumb, index, middle finger and medial half of the ring finger on the palmar aspect)
- Loss of grip strength
- Clumsiness
The pain of CTS is usually described as being:
- Worse at night
- Gradual onset
- Intermittent
- Relieved by shaking/flicking the hand
Other important areas to cover in the history include:
- Social history (e.g. how is it affecting their daily activities)
- Screen for red flags for serious conditions such as fractures (e.g. onset of symptoms after injury)
- Past medical history which may suggest a cause of the CTS (e.g. diabetes mellitus, hypothyroidism, rheumatoid arthritis or osteoarthritis)
Clinical examination
For suspected CTS, a thorough examination of both hands and wrists is necessary. See the Geeky Medics guide here for further information.
The dominant hand is affected more frequently, but bilateral involvement has been reported to occur in ~30% of cases.8
Typical clinical findings in CTS include:1
- Sensory changes or loss in the distribution of the median nerve (the thumb, index finger, middle finger and radial half of the ring finger)
- The sensation is usually preserved over the palm and thenar eminence due to the palmar cutaneous branch of the median nerve not passing through the carpal tunnel
- Wasting of thenar eminence muscles
- Reduced strength of thumb abduction (lifting the thumb off the palm)
- Dry skin on the thumb, index and middle fingers (due to loss of autonomic innervation)
There are three special tests which can be performed to support a diagnosis of CTS:
- Phalen’s test: positive if flexing the wrist for 60 seconds causes pain or paraesthesia in the median nerve distribution.
- Tinel’s test: positive if tapping lightly over the median nerve at the wrist produces paraesthesia or pain in the median nerve distribution.
- Carpal tunnel compression test (Durkan’s test): is positive if pressure over the proximal edge of the carpal ligament (proximal wrist crease) with the thumbs produces or worsens paraesthesia in the distribution of the median nerve.
Other examinations to carry out include:
- Cervical spine (to rule out radiculopathy)
- Musculoskeletal examination of the upper limb
- Neurological examination of the upper limb
Differential diagnoses
Table 2. Differential diagnoses of CTS.9
| Differential diagnosis | Typical presentation (differences to CTS) |
| Proximal median neuropathies |
Numbness over the thenar eminence (involvement of palmar cutaneous branch) Weakness of forearm pronation (pronator teres) Weakness of wrist flexion (flexor carpi radialis) Usually unilateral |
|
Cervical radiculopathy (C6/7)
|
Sudden onset of severe unilateral neck pain, radiating to the shoulder or arm Associated weakness affects shoulder movements, elbow, wrist and fingers Numbness is predominantly the dorsal aspect of first and second fingers There will be decreased or absent biceps, triceps and brachioradialis reflexes |
|
Ulnar nerve compression
|
Sensory symptoms occur on the medial aspect of the hand and the 4th and 5th digits Abduction of digiti minimi is weak There is no weakness of the thumb More commonly the non-dominant hand is affected |
|
De Quervain’s tenosynovitis
|
Pain on movement of thumb and/or wrist Worsens on heavy lifting |
| Lateral epicondylitis |
Pain in the lateral elbow and lateral forearm Lateral epicondyle is tender to palpation |
| Motor neuron disease |
Muscle weakness and atrophy is widespread, progressive and involves more than just the median nerve Fasciculations are usually prominent |
| Stroke/transient ischaemic attack |
Often there is sensory and motor loss in a cortical-type pattern (e.g. whole hand or limb). Ipsilateral face and/or leg may also be affected. Unlike with CTS, the onset is sudden |
Investigations
In primary care, appropriate investigations (such as blood tests or ultrasound scan) should be arranged if a specific underlying cause (e.g. hypothyroidism or ganglion cyst) is suspected.1
Complex investigations are not necessary before starting conservative treatment in clinically obvious cases. However, in cases of diagnostic doubt or before surgery, nerve conduction studies should be considered.6
Electrodiagnostic tests
- Electromyography (EMG): a fine needle is inserted into a muscle. Electrical activity viewed on a screen can determine the severity of damage to the median nerve. EMG is the most sensitive and specific test and can rule out other diagnoses (e.g. C6 radiculopathy) or provide evidence of another co-existent disease (e.g. polyneuropathies).9
- Nerve conduction studies: electrodes are placed on the hands and wrist. Small electric shocks are applied and the speed with which the nerve transmits impulses is measured.
Imaging
- Ultrasound scan: ultrasound can be used to identify any structural abnormalities that might be impacting the nerve (such as ganglion cyst or tendinitis) and can also assist in the diagnosis of CTS, given the median nerve might swell and become enlarged when it is damaged. In addition, ultrasound can assist in guiding needle placement for steroid injection into the carpal tunnel.9
Management
Conservative management may be successful for early or mild disease or advanced disease with minimal symptoms.
If non-operative strategies fail, carpal tunnel decompression provides good results and high levels of reported satisfaction for most patients.6
Untreated, CTS can spontaneously improve in up to one-third of individuals, particularly in younger women. This may reflect the natural course of pregnancy-induced CTS.9
Conservative management1,6
- Splinting: a splint worn at night can keep the wrist in a neutral position.
- Activity changes: avoidance of repetitive movements and breaks from tasks which precipitate symptoms. If CTS is work-related, advise the person to arrange an assessment with their employer to discuss adaption of the workplace or temporarily changes to their duties.
- Simple analgesia: there is no data that non-steroidal anti-inflammatory drugs (NSAIDs) are superior to placebo in the treatment of CTS. However, in the absence of contraindications, a trial may be beneficial to the patient.
- Optimisation of treatment for underlying causes (e.g. osteoarthritis, rheumatoid arthritis and hypothyroidism).
Medical management
- Corticosteroid injections: corticosteroid injections into the carpal tunnel, done under ultrasound guidance, can alleviate symptoms temporarily for about 4 weeks. Risks of corticosteroid injection include nerve damage from intrafascicular injection, tendon rupture and haemorrhage.8,9
Surgical management
The surgical treatment of CTS is widely available on the NHS. The operation usually takes less than 30 minutes, with patient’s having a local anaesthetic and being discharged immediately afterwards.10
The operation involves opening the roof of the carpal tunnel (the flexor retinaculum) to reduce the pressure on the nerve. There are 2 common methods:
- Open release: this is the most common method and involves an incision over the tunnel at the wrist, opening the roof under direct vision.
- Endoscopic release: the roof is opening with instruments inserted through one or two small incisions.
Night pain and tingling usually disappear within a few days. In severe cases, improvement of constant numbness and muscle weakness may be slow or incomplete. It generally takes about 3 months to regain full strength and a fully comfortable scar.11
Prognosis
Symptoms can spontaneously resolve within 6 months for about one-third of patients.6
For people with idiopathic CTS, good prognostic indicators include a short duration of symptoms, young age and carpal tunnel syndrome due to pregnancy. Poor prognostic indicators include bilateral symptoms and a positive Phalen’s test.1
Appropriate management of CTS is usually successful in relieving symptoms:9
- Wrist splints can result in a 70% improvement in symptoms
- Corticosteroid injections have a 60 – 70% success rate up to 6 months post-injection
- Surgical success rates are approximately 80 – 90%
Recurrence of symptoms after surgery occurs in about 5% of patients and repeat surgery carries lower success rates and higher complication rates.9
Complications
If untreated, carpal tunnel syndrome can lead to difficulties with activities of daily life (including work) and sleep due to symptoms of pain, sensory disturbance, weakness and impaired fine manipulation. Sustained high pressure can ultimately lead to axonal loss.1
Key points
- Carpal tunnel syndrome (CTS) occurs due to compression of the median nerve within the carpal tunnel at the wrist.
- There are many causes of CTS, such as pregnancy, rheumatoid arthritis, diabetes mellitus and ganglion cysts. However, in most cases, a single cause is not identified (idiopathic CTS).
- Typical findings in the history are a gradual onset, intermittent tingling over the area of the hand supplied by the median nerve, which is usually worse at night and relieved by shaking out the hand.
- The main findings on examination are isolated sensory changes in the median nerve distribution with sparing of the thenar eminence. There is a weakness of thumb abduction and in severe cases wasting of the thenar eminence.
- CTS is usually managed in primary care with conservative measures such as splinting and activity modification.
- Worsening or severe cases of CTS can be managed in secondary care with corticosteroid injections and carpal tunnel release surgery.
Reviewer
Miss Nicola Mackay
ST6 Trauma and Orthopaedics
Editor
Dr Chris Jefferies
References
- NICE Clinical Knowledge Summaries (CKS). Carpal Tunnel Syndrome. Last edited in September 2016. Available from: [Link]
- OrthoInfo. Carpal Tunnel Syndrome. Last reviewed July 2016. Available from: [Link]
- Radiopedia. Carpal Tunnel. Available from: [Link]
- OpenStax College. Wikimedia Commons File: The Carpal Tunnel. Cited April 2020 [CCBY] [Link]
- National Institute of Neurological Disorders and Stroke. Carpal Tunnel Syndrome Fact Sheet. Last edited in March 2020. Available from: [Link]
- Patient.info. Carpal Tunnel Syndrome and Median Nerve Lesions. Last reviewed May 2019. Available from: [Link]
- Geeky Medics. Created in March 2020.
- Carpal Tunnel Syndrome. Available from: [Link]
- BMJ Best Practice. Carpal Tunnel Syndrome. Available from: [Link]
- British Association of Plastic Reconstructive and Aesthetic Surgeons (BAPRAS). Carpal Tunnel Syndrome. Available from: [Link]
- The British Society for Surgery of the Hand (BSSH). Carpal Tunnel Syndrome. Available from: [Link]
