
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
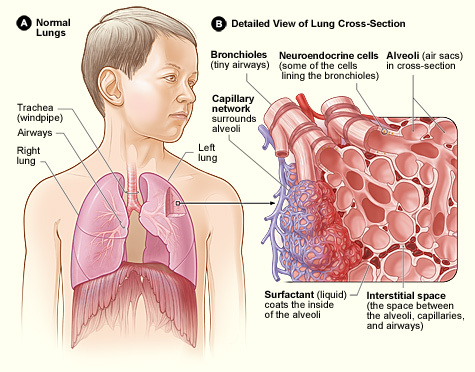
Interstitial lung disease (ILD) is an umbrella term for a broad spectrum of conditions affecting the lung interstitium, which is the space between an alveolus and its surrounding capillaries.1
In the UK, the prevalence of ILD is 50 per 100,000. The commonest type of ILD is idiopathic pulmonary fibrosis, which has an incidence of 6,000 new cases per year.2
Mortality varies across the different ILDs as they are a heterogeneous range of conditions. Mortality is particularly high in idiopathic pulmonary fibrosis, with a median survival of 4 years, which is worse than most types of cancer.3
Aetiology
Pathophysiology
In ILD, there is inflammation and fibrosis (scarring) in the lung interstitium (figure 1).5
Some ILDs (such as sarcoidosis) are predominantly inflammatory, with little fibrosis. This inflammation is mediated by innate and adaptive immune cells and may resolve.6
Other ILDs (such as idiopathic pulmonary fibrosis) are characterised by fibrosis in the lung interstitium, which is irreversible. Fibrosis is triggered by repeated injury to the lung tissue (e.g. from inhaled toxins).
Usually, fibroblasts respond to this lung injury by secreting extracellular matrix, which repairs the injuries. In ILD, genetic mutations lead to excess secretion of extracellular matrix, which accumulates in the lung interstitium, leading to fibrosis.7
The lung interstitium becomes thicker, increasing the diffusion distance for oxygen to travel from the air in the alveoli to the blood in the surrounding capillaries. Hence, gas exchange in the lungs is compromised.
Classification4
Primary (unknown cause)
- Idiopathic pulmonary fibrosis
- Acute interstitial pneumonia (can be acute or subacute)
- Desquamative interstitial pneumonia (associated with smoking)
Secondary (known cause)
Connective tissue and autoimmune disease:
- Sarcoidosis
- Rheumatoid arthritis
- Systemic lupus erythematosus (SLE)
Infective:
- Mycoplasma pneumonia
- Pneumocystis pneumonia
Environmental:
- Asbestosis
- Silicosis
Drugs:
- Methotrexate
- Amiodarone
- Bleomycin
Risk Factors
Risk factors for ILD include:
- Male sex
- Cigarette smoking
- Regular dust exposure (could be occupational)
Clinical features
History
Typical symptoms of ILD include:
- Progressive exertional dyspnoea (usually presents slowly, over many weeks and months)
- Dry cough
- Connective tissue disease symptoms, such as arthralgia, difficulty swallowing and dry eyes
- General malaise and fatigue (due to underlying connective tissue disease or vasculitis)9
Other important areas to cover in the history include:
- Drug history: ask about any exposure to medications which cause ILD (see “Classification” section).
- Smoking history: quantify in pack-years (1 pack-year = smoking 20 cigarettes a day for a year). Also ask about e-cigarettes and illicit inhaled substances, such as “crack” cocaine.10,11
- Occupation: may be exposed to inhaled toxins. Susceptible occupations include farmers (hay dust and Aspergillus mould), bakers (flour dust and additive enzymes) and plumbers/construction workers (asbestos).12
- Social history: ask about the presence of mould and pets at home, and if the patient has any hobbies which increase exposure to inhaled toxins (such as bird-keeping, which exposes the patient to avian proteins).
Clinical examination
A full respiratory examination should be performed in suspected cases of ILD. Also perform a brief examination of the patient’s joints, to assess for the presence of connective tissue disease.
Typical clinical findings in ILD include:
- Bilateral fine end-inspiratory crepitations (may sound like Velcro): due to the sudden opening of small airways during inspiration, which were held closed during the previous expiration.13
- Dullness to percussion: due to pleural effusion, which can occur in sarcoidosis and some connective tissue diseases.14
- Finger clubbing (figure 2): may be due to increased secretion of growth factors, leading to increased growth of extracellular matrix in the nails.15
- Skin signs: includes Raynaud’s phenomenon in systemic sclerosis (figure 3), erythema nodosum in sarcoidosis (figure 4).
- Arthritis: due to connective tissue disease.



Differential Diagnoses
Exertional dyspnoea and cough have important differential diagnoses. Table 1 outlines these differential diagnoses, and the features which differentiate them from ILD.
Table 1. Differential diagnoses of ILD.
| Differential diagnosis | Features differentiating from ILD |
| COPD |
Cough is more productive of sputum Lung function tests: obstructive pattern (FEV1/FVC < 70%) Examination and chest X-Ray: chest hyperinflation |
| Asthma |
Diurnal variation in symptoms and peak flow History of atopy Lung function tests: bronchodilator reversibility |
| Congestive cardiac failure |
Orthopnoea (dyspnoea while lying down) Paroxysmal nocturnal dyspnoea (sudden dyspnoea which wakes the patient up from sleep) Blood tests: elevated BNP Echocardiogram: reduced ejection fraction |
| Lung cancer |
Significant weight loss Haemoptysis Imaging: visible tumour |
| Bronchiectasis |
Cough is more productive of sputum More frequent lower respiratory tract infections, often starting in childhood Lung function tests: obstructive pattern (FEV1/FVC < 70%) |
Investigations
Bedside investigations
- Pulse oximetry: aim for 94-98% initially, but the target saturations may be reduced in progressive disease (this is a decision made by a senior clinician).
- Urine dipstick: haematuria and proteinuria may suggest underlying vasculitis.19
- Lung function tests: typically show a restrictive pattern (reduced FVC and reduced FEV1), but may also be normal.
Laboratory investigations
- FBC: may show anaemia of chronic disease.
- CRP and ESR: may be elevated.
- U&Es: may be deranged if there is an underlying vasculitis.
- Autoimmune antibodies: anti-CCP suggests rheumatoid arthritis, ANA suggests SLE. Autoimmune antibodies may also be raised in idiopathic pulmonary fibrosis.20
Imaging
- Chest X-ray (figure 5): typically shows reticular (fine) opacities. The location of fibrosis may suggest particular causes (table 2).
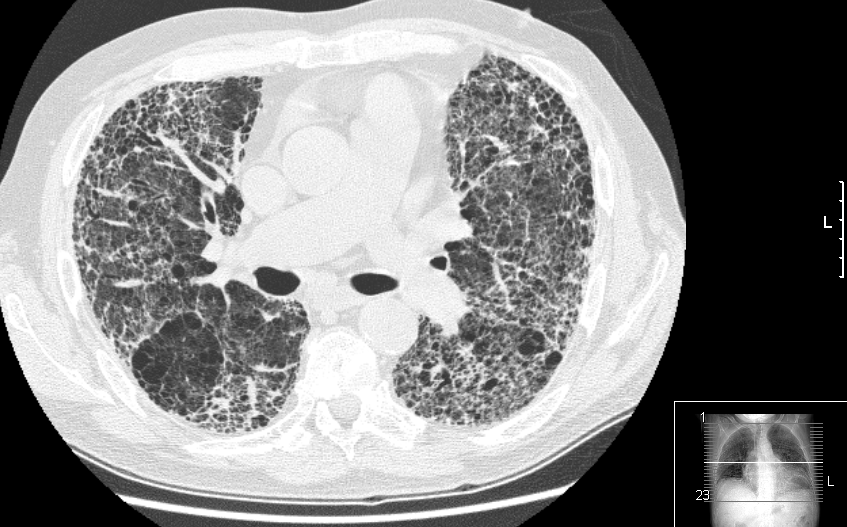
- High-resolution CT (HRCT) (figure 6): HRCT is preferred to volume CT as it provides higher quality images of the lung parenchyma, which is the area affected in ILD. Some ILDs, especially idiopathic pulmonary fibrosis, show a “usual interstitial pneumonia” pattern, which includes:
- Honeycombing (clusters of cystic airspaces)
- Traction bronchiectasis (dilated airways, which are pulled apart by areas of surrounding fibrosis)
- Reticular opacities (thickening of the lung interstitium)
Table 2. The causes of upper zone and lower zone fibrosis.
| Upper zone fibrosis = CHARTS | Lower zone fibrosis = RASIO |
|
Coal-worker pneumoconiosis Histiocytosis-X Ankylosing spondylitis Radiation (e.g. for breast cancer) Tuberculosis Sarcoidosis and silicosis |
Rheumatoid arthritis Asbestosis SLE, scleroderma and Sjogren’s syndrome Idiopathic pulmonary fibrosis Others (including drugs) |

Invasive investigations
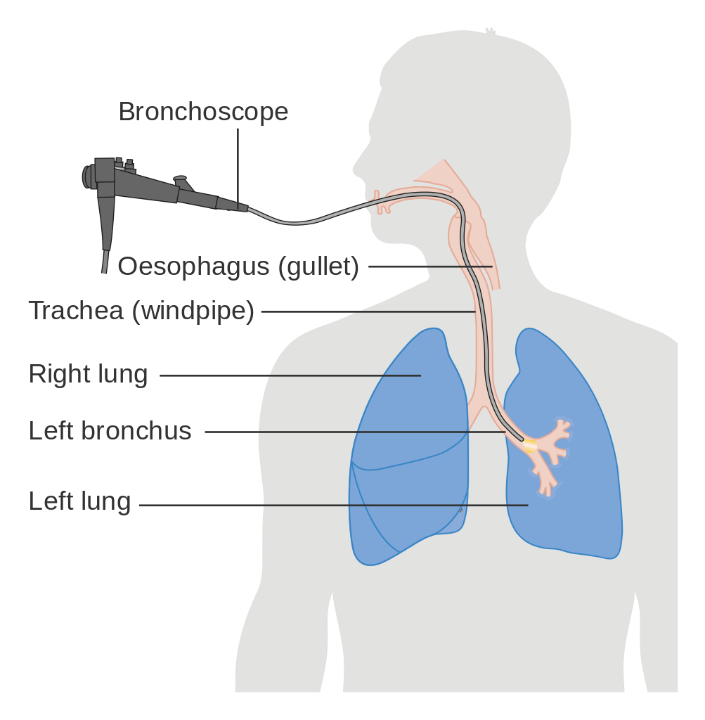
- Bronchoalveolar lavage (BAL) (figure 7): a bronchoscope (small camera) is inserted into the airways, and sterile saline is injected through the bronchoscope into the airways. The saline is then collected via suction and analysed. This helps to diagnose the underlying cause of the ILD, and to also exclude infection or malignancy.23
- Trans-bronchial biopsy/surgical lung biopsy: a small sample of lung is collected and then analysed by a pathologist. This may be needed if previous tests are inconclusive, or if a tissue sample is needed to make the diagnosis.
Management
Conservative management
- Avoid any underlying causes (e.g. drug or inhaled toxin)
- Smoking cessation
- Pulmonary rehabilitation
- Annual influenza vaccine and one-off pneumococcal vaccine
Medical management
Medical management varies for each type of ILD. Some important examples include:
- Idiopathic pulmonary fibrosis: antifibrotics (nintedanib or pirfenidone).
- Sarcoidosis: corticosteroids (prednisolone).
- Connective tissue disease: corticosteroids and steroid-sparing agents (azathioprine or mycophenolate).
- Extrinsic allergic alveolitis: corticosteroids.
Long-term oxygen therapy (LTOT)
Some patients with ILD may benefit from LTOT. Indications for LTOT are one of the following:
- Resting PaO2 ≤ 7.3kPa
- Resting PaO2 ≤ 8.0kPa with peripheral oedema/polycythaemia (haematocrit ≥ 55%)/pulmonary hypertension
LTOT is contraindicated in current smokers due to the risk of burns.
Surgical management
- Lung transplantation: for patients with severely impacted quality-of-life, despite optimum medical management.25
Complications
Disease-related complications
- Respiratory failure: due to failure of gas exchange in the lungs.
- Pulmonary hypertension: due to chronic hypoxic pulmonary vasoconstriction (constriction of blood vessels supplying fibrotic areas of the lung, to direct blood to healthier areas of the lung).26
- Anxiety and depression: due to impaired quality-of-life.
Treatment-related complications
- Due to long-term steroid use: osteoporosis, hypertension, Cushing’s syndrome.
- Due to antifibrotics: diarrhoea, nausea, anorexia.
Key points
- ILD is an umbrella term for a broad spectrum of conditions which affect the lung interstitium.
- ILD can be classified based on whether it has an unknown cause (primary) or a known cause (secondary).
- ILD typically presents with exertional dyspnoea and dry cough, but it may present with non-specific symptoms (such as malaise).
- A diagnosis is based on laboratory results (which may suggest an underlying autoimmune cause) and imaging.
- Management of ILD varies according to the underlying cause – steroids and antifibrotics are potential options.
- The main complications of ILD are respiratory failure and pulmonary hypertension.
Feedback
Please click here to fill out the feedback form, which should take less than 1 minute of your time. Feedback is vital as it allows authors to improve their articles, leading to even better content on Geeky Medics!
Reviewer
Dr Neeraj Shah
Respiratory Medicine Registrar
Editor
Dr Chris Jefferies
References
- Wallis A and Spinks K. The diagnosis and management of interstitial lung diseases. Published in 2015. Available from: [LINK]
- British Lung Foundation. The battle for breath: the impact of lung disease in the UK. Published in 2016. Available from: [LINK]
- British Thoracic Society. BTS ILD Registry Annual Report 2019. Published in 2019. Available from: [LINK]
- Bourke SJ. Interstitial lung disease: progress and problems. Postgraduate Medical Journal. Published in 2006. Available from: [LINK]
- Kalchiem-Dekel O et al. Interstitial lung disease and pulmonary fibrosis: a practical approach for general medicine physicians. Journal of Clinical Medicine. Published in 2018. Available from: [LINK]
- Paterson KC and Chen ES. The pathogenesis of pulmonary sarcoidosis and implications for treatment. Chest. Published in 2018. Available from: [LINK]
- Lederer DJ and Martinez FJ. Idiopathic Pulmonary Fibrosis. New England Journal of Medicine. Published in 2018. Available from: [LINK]
- National Heart Lung and Blood Institute. Lung Interstitial Space. License: [Public domain]. Available from: [LINK]
- Okazaki T et al. Vasculitis syndrome – diagnosis and therapy. Journal of General and Family Medicine. Published in 2017. Available from: [LINK]
- Layden JE et al. Pulmonary illness related to e-cigarette use in Illinois and Wisconsin – final report. New England Journal of Medicine. Published in 2020. Available from: [LINK]
- Vidyasankar G et al. A severe complication of crack cocaine use. Canadian Respiratory Journal. Published in 2015. Available from: [LINK]
- Cullinan P et al. Occupational lung diseases: from old and novel exposures to effective preventive strategies. Lancet Respiratory Medicine. Published in 2017. Available from: [LINK]
- Bohadana A et al. Fundamentals of lung auscultation. New England Journal of Medicine. Published in 2014. Available from: [LINK]
- Highland KB and Heffner JE. Pleural effusion in interstitial lung disease. Current Opinion in Pulmonary Medicine. Published in 2004. Available from: [LINK]
- Sarkar M et al. Digital Clubbing. Lung India. Published in 2012. Available from: [LINK]
- Desherinka D. Finger clubbing. Licence: [CC BY-SA]. Available from: [LINK]
- Raynaud’s Phenomenon. License: [CC BY-SA]. Available from: [LINK]
- Heilman J. Erythema Nodosum. License: [CC BY-SA]. Available from: [LINK]
- Suresh E. Diagnostic approach to patients with suspected vasculitis. Postgraduate Medical Journal. Published in 2006. Available from: [LINK]
- BMJ Best Practice. Idiopathic Pulmonary Fibrosis. Published in 2019. Available from: [LINK]
- IPFEditor. Pulmonary Fibrosis Chest X-Ray. License: [CC BY-SA]. Available from: [LINK]
- Drriad. Pulmonary Fibrosis CT. License: [CC BY-SA]. Available from: [LINK]
- Bradley B et al. BTS interstitial lung disease guidelines. Thorax. Published in 2008. Available from: [LINK]
- Cancer Research UK. Bronchoscopy. License: [Public domain]. Available from: [LINK]
- Abelson D and Glanville AR. Controversies and emerging topics in lung transplantation. Published in 2018. Available from: [LINK]
- Kosanovic D et al. Pulmonary Hypertension due to lung diseases and hypoxia: what do we actually know? Canadian Respiratory Journal. Published in 2017. Available from: [LINK]
