

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
The intrinsic muscles of the shoulder form the scapulohumeral group, mainly originating from the scapula and inserting onto the humerus.1
The intrinsic muscles can be further divided into the deltoid muscle, teres major and the rotator cuff muscles; supraspinatus, infraspinatus, subscapularis and teres minor.2
This article will primarily highlight the origin, insertion, innervation and function of the intrinsic muscles of the shoulder.
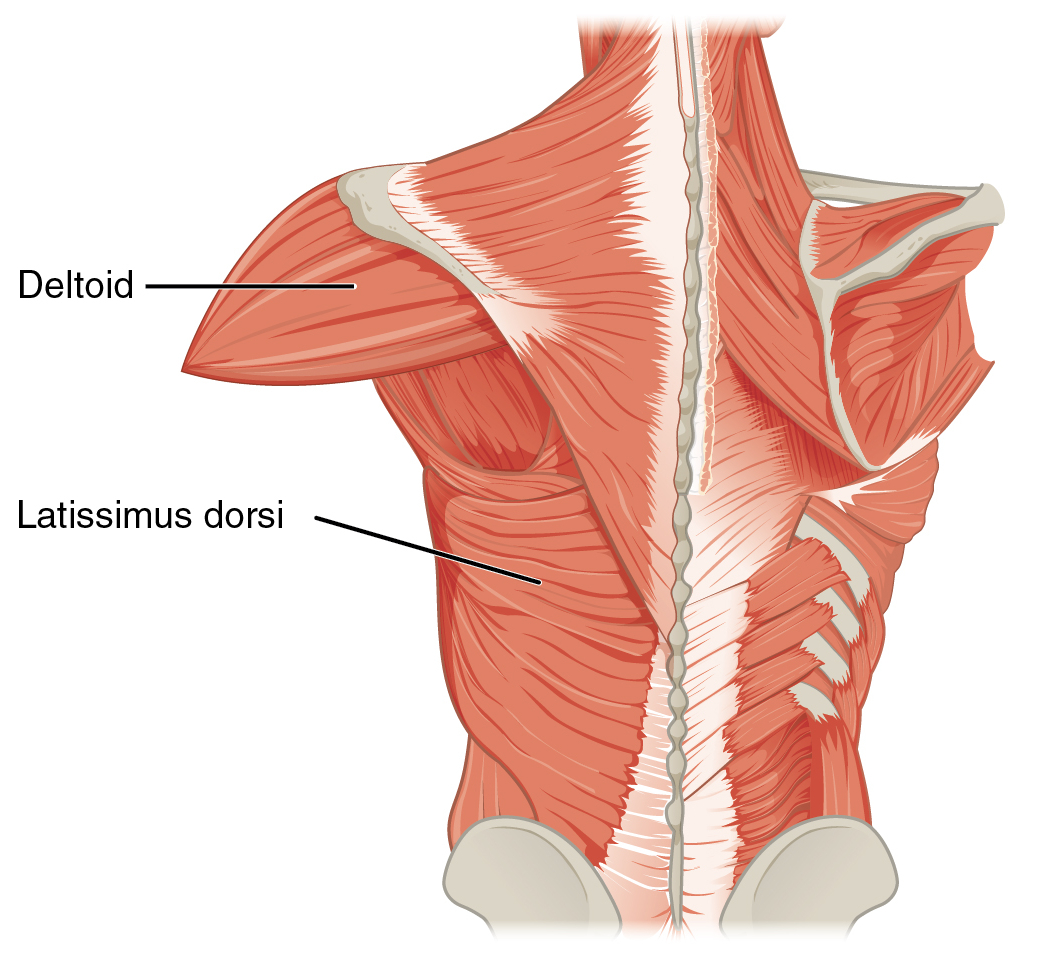
Deltoid
The deltoid forms the rounded contour of the shoulder and is comprised anterior, intermediate and posterior fibres.1
Origin and insertion
The anterior (or clavicular) fibres originate from the lateral third of the clavicle. The intermediate (or acromial) fibres originate from the acromion process of the scapula. The posterior (or spinal) fibres originate from the spine of the scapula.
All fibres converge toward their insertion on the deltoid tuberosity on the middle of the shaft of the humerus.
Innervation
The deltoid is innervated by the axillary nerve (C5-6).
Function
The functions of the deltoid muscle can be categorised based on the groups of fibres involved:
- Anterior fibres: shoulder flexion and internal rotation.
- Intermediate fibres: abduction of the shoulder (these fibres take over from supraspinatus which initiates shoulder abduction).
- Posterior fibres: shoulder extension and external rotation.
Teres major
Teres major is a thick muscle which is positioned superiorly to latissimus dorsi.4
Origin and insertion
Teres major originates from the posterior aspect of the inferior angle of the scapula and inserts onto the medial lip of the bicipital groove (intertubercular sulcus) of the humerus.4
Innervation
The majority of teres major is innervated by the lower subscapular nerve and a small portion is innervated by the thoracodorsal nerve (C5-8).4
Function
Teres major acts to adduct the humerus as well as assisting in extension and internal rotation of the shoulder.4

Rotator cuff muscles
All four rotator cuff muscles originate from areas of the scapula and insert onto the humeral head.2
The glenohumeral (GH) joint is highly mobile, allowing a large range of movement, but this comes at the cost of stability. The resting tension of the rotator cuff muscles provides the primary stabilizing force on the GH joint.1,2
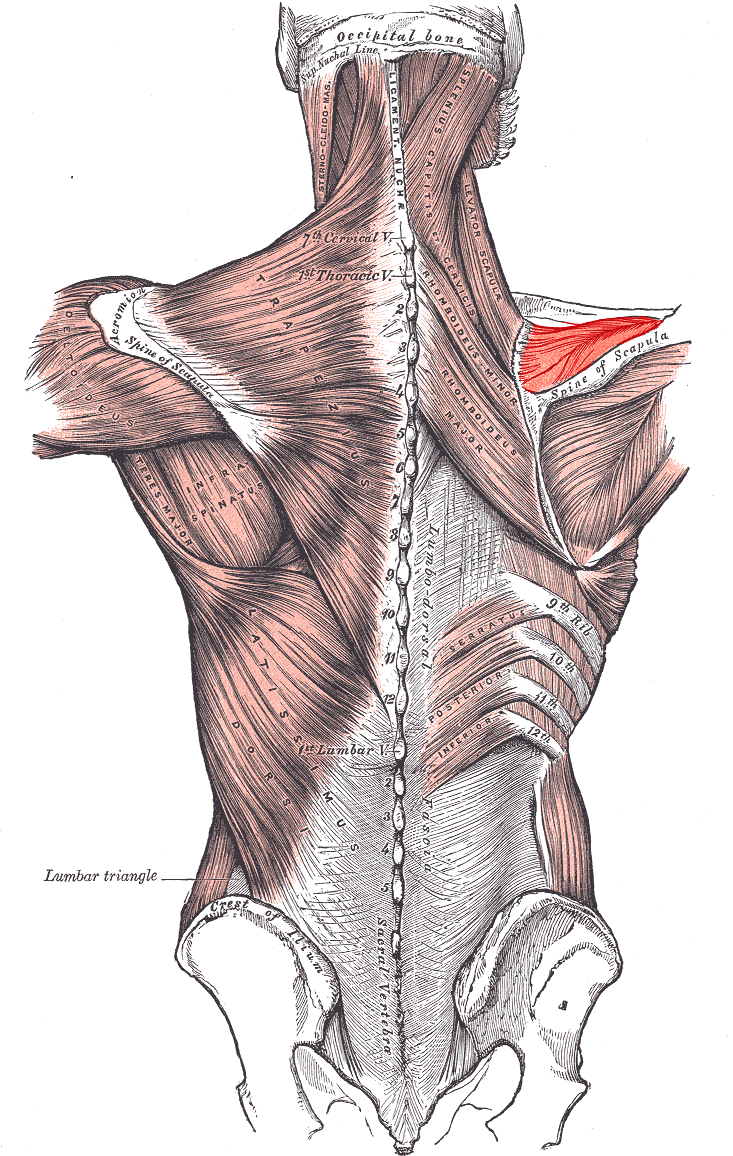
Supraspinatus
Supraspinatus arises from the scapula and runs beneath the cover of the acromion.5
Origin and insertion
Supraspinatus originates from the supraspinous fossa and the muscle’s tendon inserts onto the superior facet of the greater tubercle of the humerus.5
Innervation
Supraspinatus is innervated by the suprascapular nerve (C5).5
Function
Supraspinatus acts to initiate abduction of the arm (especially between the first 15 degrees of movement) and then acts to assist the deltoid muscle (15-90 degrees of movement).5
Clinical relevance: impingement syndrome
Impingement syndrome is caused by rotator cuff tendonitis as the tendons pass beneath the acromion. The supraspinatus muscle’s tendon is most commonly affected.
Impingement syndrome typically presents with pain, weakness and restricted shoulder movement. Patients with impingement syndrome often complain of pain when their arms are raised (this is particularly common in mechanics and manual labourers who work with their arms overhead). When the arm is raised, the subacromial space narrows, which can result in impingement of the supraspinatus muscle tendon leading to an inflammatory response.
Clinical examination
Typical findings on clinical examination in supraspinatus impingement syndrome include:
- Pain experienced between 60-120° of shoulder abduction (known as a ‘painful arc’).
- Weakness and pain experienced when the supraspinatus muscle is isolated using the ‘Empty can/Jobe’s test
For more information, see the Geeky Medics shoulder examination guide.
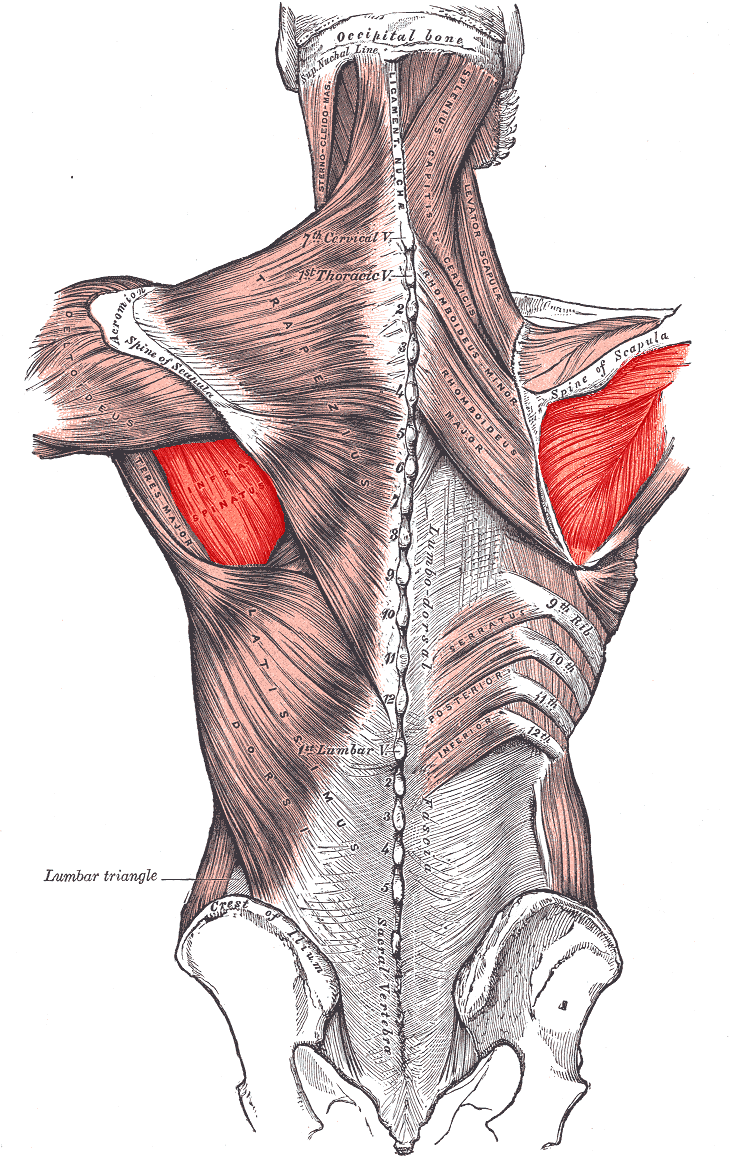
Infraspinatus
Infraspinatus is a thick triangular muscle. The spine of the scapula acts to separate the origin of the supraspinatus muscle from the infraspinatus muscle.6
Origin and insertion
The infraspinatus muscle originates from the infraspinous fossa of the scapula, passing over the lateral border of the spine of the scapula before inserting onto the middle facet of the greater tuberosity on the humerus.6
Innervation
Infraspinatus has the same innervation as supraspinatus – the suprascapular nerve (C5).6
Function
Infraspinatus acts to externally rotate the arm.6
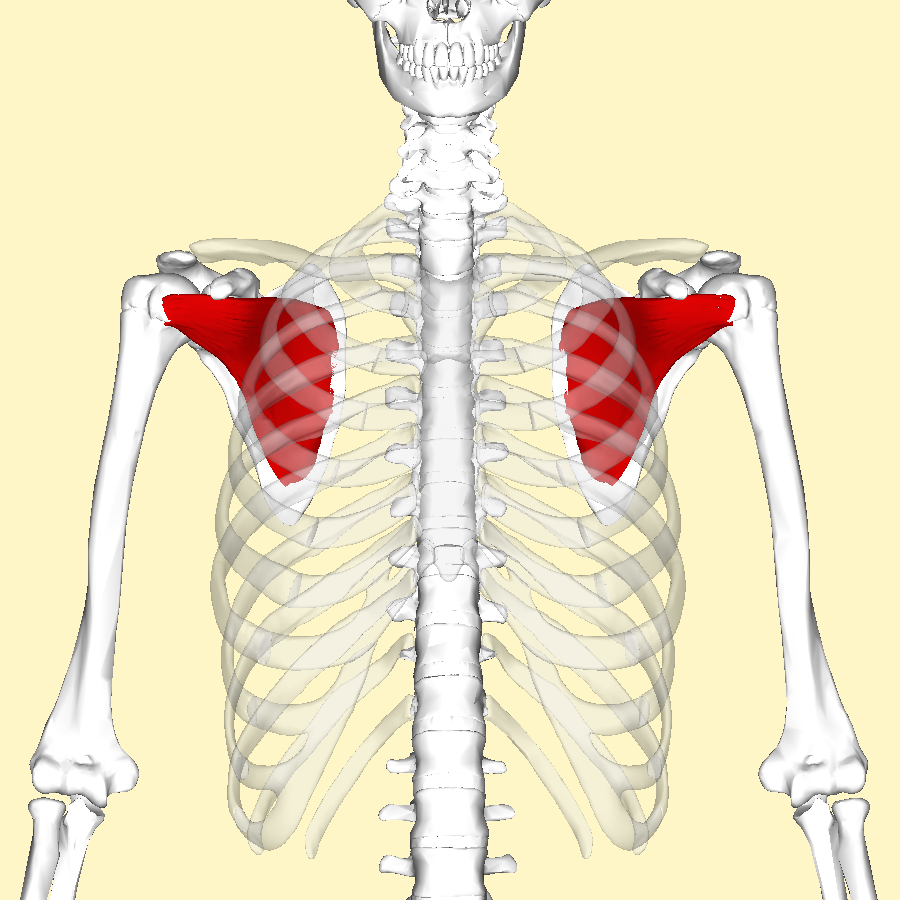
Subscapularis
Subscapularis is another large triangular-shaped muscle.7
Origin and insertion
It originates from the subscapular fossa (ventral surface) and inserts onto the lesser tuberosity of the humerus (this is the only rotator cuff muscle which doesn’t attach to the greater tuberosity).7
Innervation
Subscapularis is innervated by the upper and lower subscapular nerves (C5-6).7
Function
Subscapularis acts to internally rotate and adduct the arm.7
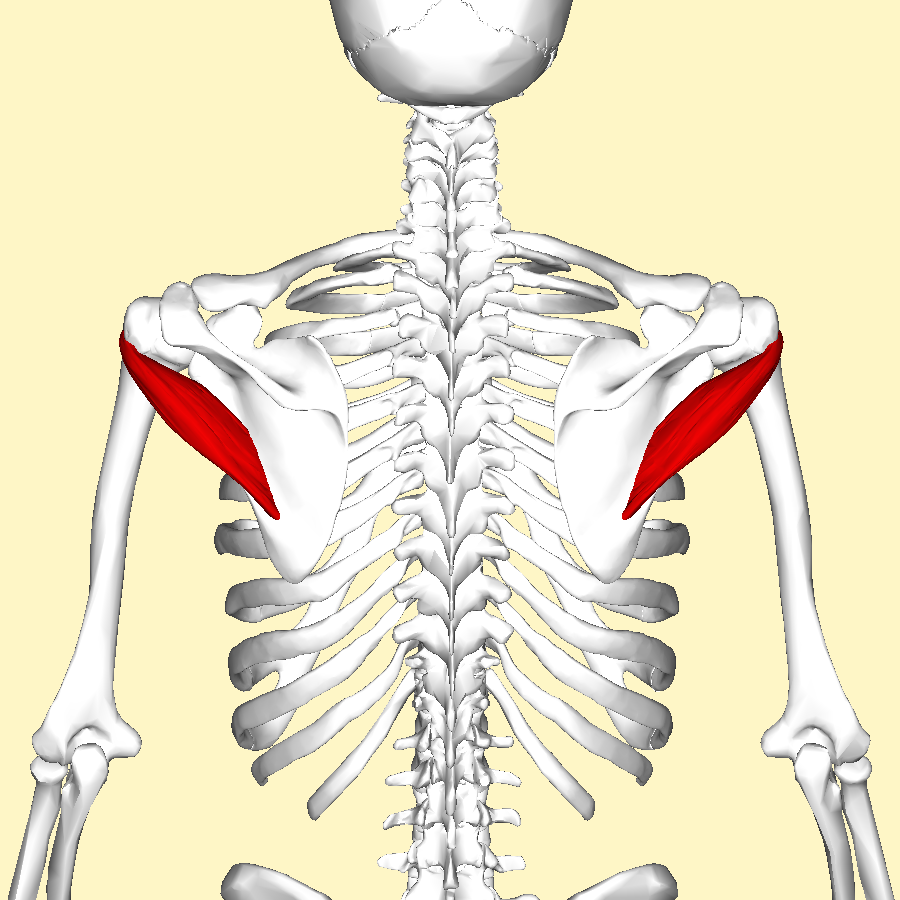
Teres minor
Teres minor is a narrow elongated muscle which is superior to teres major.8
Origin and insertion
Teres minor originates from the lateral border of the scapula, before inserting onto the inferior facet of the greater tubercle on the humerus.8
Innervation
Teres minor is innervated by the axillary nerve (C5-6).8
Function
Teres minor acts to externally rotate the arm.8
Mnemonic: SIT
SIT is a mnemonic to remember the superior to inferior attachments of the rotator cuff muscles onto the greater tubercle of the humerus.5
- Supraspinatus
- Infraspinatus
- Teres minor
Summary
| Muscle | Origin | Insertion | Innervation | Action |
| Deltoid | Lateral ⅓ clavicle + acromion & the spine of the scapula | Deltoid tuberosity | Axillary nerve |
Anterior fibres: Flexion & internal rotation Intermediate fibres: major abductor, takes over from supraspinatus Posterior fibres: |
| Teres major | Inferior angle of the scapula | Medial lip of bicipital groove | Lower subscapular nerve |
Adducts & extends at the shoulder Internally rotates the arm |
| Rotator cuff muscles | ||||
| Supraspinatus | Supraspinous fossa |
Greater tubercle |
Suprascapular nerve |
Initiates abduction (0-15 degrees) & assists deltoid for 15-90 degrees |
| Infraspinatus | Infraspinous fossa | Externally rotates | ||
| Subscapularis | Subscapular Fossa | Lesser tubercle | Upper and lower subscapular nerves |
Internally rotates arm |
| Teres minor | Lateral border of the scapula | Greater tubercle | Axillary nerve |
Externally rotates |
References
- Drake, R et al. (2010). Gray’s Anatomy for students. 2ndedition. Philadelphia, PA: Churchill Livingstone Elsevier
- Matava MJ, Purcell DB, Rudzki JR (2005). “Partial-thickness rotator cuff tears”. Am J Sports Med. 33 (9): 1405–17. Available from: [LINK].
- OpenStax College. Deltoid muscle. Licence: [CC BY]. Available from: [LINK].
- Mikael Häggström, used with permission. Teres Major. Available from: [LINK].
- Mikael Häggström, used with permission. Supraspinatus. Available from: [LINK].
- Mikael Häggström, used with permission. Infraspinatus. Available from: [LINK].
- Anatomography. Subscapularis muscle. License [CC BY-SA 2.1 JP]. Available from [LINK].
- Anatomography. Teres minor muscle. License [CC BY-SA 2.1 JP]. Available from [LINK].
