

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
The ear can be divided into three parts: the external, middle and inner ear. The ears are an organ of hearing and balance, converting information from our external environment into electrical signals that can be processed by the brain.
This article will explore the three anatomical sections of the ear, highlighting their individual anatomy and function, as well as explaining how all three parts work to achieve balance and the ability to hear.
External ear
The external ear is the part of the ear we can see with the naked eye. It is attached to the lateral aspect of the head and is characteristically divided into two parts: the auricle or pinna and the external acoustic meatus (more commonly referred to as the ear canal).1,2,3
The auricle
Apart from the lobule, which contains fat and connective tissue, the auricle is a cartilaginous structure covered by skin.
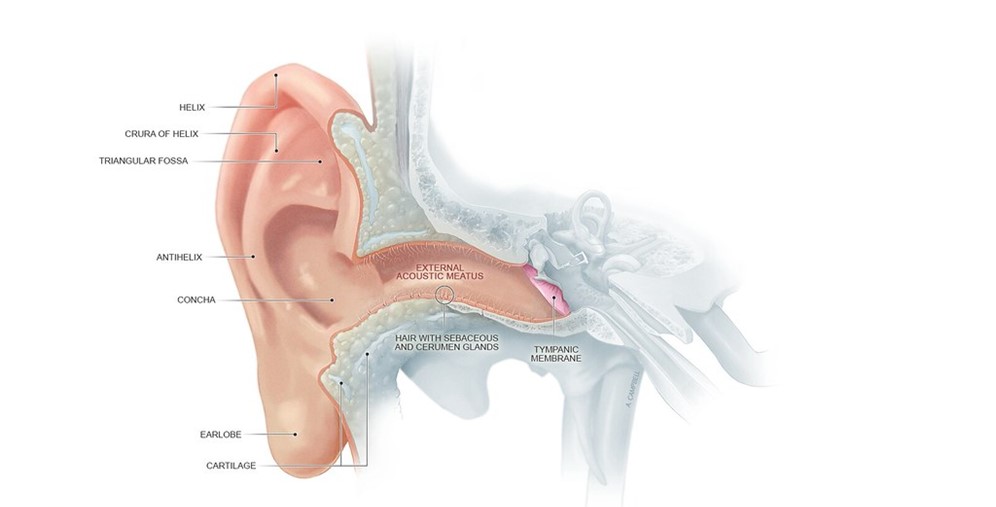
Surface anatomy of the auricle
The outer curve of the auricle is called the helix, which connects with the lobule of the ear. Parallel and anterior to the helix is a smaller curve, aptly called the antihelix.
In the centre of the auricle, there is a depression called the concha of the auricle, which gives rise to the external acoustic meatus.
Anterior to the opening of the external acoustic meatus is an elevation of cartilage called the tragus.
The tragus forms a protective barrier to the external acoustic meatus, partially covering it to prevent the passage of large foreign objects down the external acoustic meatus. Opposite the tragus is the antitragus.
Innervation of the auricle
The auricle has several sources of sensory innervation:
- The superficial surface is supplied by the great auricular nerve and lesser occipital nerve, both of which are branches of the cervical plexus (C2 & C3), and the auriculotemporal branch of the mandibular nerve, which is a branch of the trigeminal nerve (cranial nerve V)
- The deep part of the auricle is supplied by the vagus nerve (cranial nerve X) and facial nerve (cranial nerve VII)
Vascular supply and lymphatic drainage
The auricle is supplied by three main arteries:
- The external carotid artery gives rise to the posterior auricular artery, which supplies the posterior aspect of the auricle
- The superficial temporal artery gives rise to the anterior auricular arteries, which supplies the anterior aspect of the auricle
- Occipital artery
Lymphatic drainage from the auricle passes into the parotid and mastoid lymph nodes and eventually into the upper deep cervical nodes.
Function of the auricle
The shape of the auricle helps to capture sound waves and direct them into the external acoustic meatus and assist in determining where the sound is coming from.
The external acoustic meatus
The external acoustic meatus is a tube that travels from the deepest aspect of the concha to the tympanic membrane, which marks the divide of the external and middle ear.
The composition of the walls of the external acoustic meatus changes the deeper it travels:
- The lateral one-third of the external acoustic meatus is cartilaginous, which extends slightly deeper on the inferior portion external acoustic meatus
- The medial two-thirds of the external acoustic meatus is bony, derived from the temporal bone of the skull
- There is a slightly raised constriction located at the junction of the cartilaginous and bony portion
The entire length of the external acoustic meatus is covered with skin (keratinised squamous epithelium). The outer third (cartilaginous portion) contains hair and cerumen producing glands.
Innervation of the external acoustic meatus
Like the auricle, the external acoustic meatus has several sources of sensory innervation, including:
- The auriculotemporal nerve, which is a branch of the mandibular nerve, which branches from the trigeminal nerve (cranial nerve V)
- The auricular nerve, which is a branch of the vagus nerve (cranial nerve X)
Blood supply
The external acoustic meatus has the same blood supply as the auricle: the superficial temporal artery and the posterior auricular artery.5
Function of the external acoustic meatus1,2,3
The external acoustic meatus transmits sound to the middle ear.
The slight bend or constriction in the external acoustic meatus acts as a protective mechanism to prevent the passage of foreign objects. In addition, the cerumen produced by the glands acts as a disinfectant to kill any pathogenic organisms.
Clinical significance: Otitis externa7
Otitis externa is inflammation or infection of the external ear, commonly caused by Pseudomonas or Staphylococcus aureus bacteria.
Patients usually present with a rapid onset of otalgia, tenderness, itching, the sensation of aural fullness and sometimes conductive hearing loss. On examination, patients often complain of extreme pain on palpation of the auricle or tragus.
Treatment involves conservative measures, including water precautions for two weeks after the infection resolution. This can be achieved by plugging the ear with a Vaseline covered cotton ball when bathing. This is usually coupled with topical therapy depending on the causative organism.
This condition is more common in people with skin conditions and those who cause trauma to the ear canal with fingernails or cotton buds. Diabetes is also a risk factor.
Tympanic membrane
The tympanic membrane, or eardrum, marks the border between the external and middle ear.
It is formed of a middle layer of connective tissue with a layer of skin on its lateral surface (facing the external acoustic meatus) and mucous membrane on its medial surface (facing the middle ear).
The tympanic membrane lies at an oblique angle that helps maximise the efficiency in sound localisation. The external surface of the tympanic membrane is concave and the internal surface convex.
Surrounding the tympanic membrane is a fibrocartilaginous ring that attaches to the temporal bone, this is called the annulus.
At the centre of the tympanic membrane is the umbo, which is a concave depression that attaches to the handle of the malleus, one of the auditory ossicles in the middle ear. Located anterior-inferior to the umbo is the cone of light, which is created due to the conical shape of the tympanic membrane.
The tympanic membrane can be divided into two regions:
- The pars flaccida: where the membrane is thin and slack (small upper portion)
- The pars tensa: where the membrane is thick and taut (larger lower portion)
Innervation of the tympanic membrane
The medial surface of the tympanic membrane is supplied by the vagus (cranial nerve X) and glossopharyngeal nerve (IX).
The lateral surface of the tympanic nerve is supplied by the auriculotemporal nerve (a branch of the mandibular division of trigeminal nerve) and facial nerve.
Function of the tympanic membrane6
The tympanic membrane transmits sound waves from the external ear to the ossicles of the middle ear. The tympanic membrane and the middle ear amplify sound reaching the inner ear.
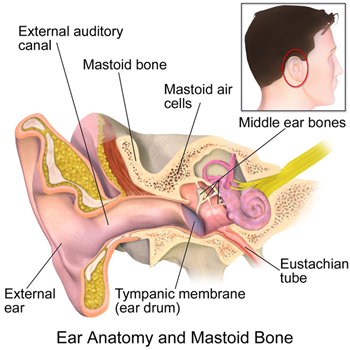
Middle ear
The middle ear, also referred to as the tympanic cavity, is an air-filled section in the temporal bone and is lined with a mucous membrane.1,2,3
It can be split into two main sections:
- The tympanic cavity proper: this is the space directly internal to the tympanic membrane
- The epitympanic recess: this is the space behind pars flaccida
Innervation of the middle ear
The medial surface of the tympanic membrane is supplied by the vagus (cranial nerve X) and glossopharyngeal nerve (IX).
Autonomic innervation to the tympanic cavity is via the tympanic nerve (a branch of CN IX) and sympathetic fibres from the carotid plexus, forming the tympanic plexus located on the surface of the cochlear promontory.
The auditory ossicles
The auditory ossicles consist of three separate bones: the malleus, incus and stapes. These connect to form a mobile chain to join the tympanic membrane of the external ear to the oval window of the inner ear.
The handle of the malleus is attached to the tympanic membrane, whilst its head links with the body of the incus in the epitympanic recess.
The incus consists of three parts: the body links with the head of the malleus, the short limb attaches to the posterior wall of the tympanic cavity and the long limb links with the stapes.
The stapes is the smallest bone in the human body and its footplate attaches to the oval window of the inner ear.
The function of the auditory ossicles is to transmit and amplify the sound vibrations from the external ear to the endolymph and perilymph of the inner ear.9
The muscles of the middle ear
Tensor tympani
Arising from the superior surface of the eustachian tube and the petrous part of the temporal bone, the tensor tympani muscle is an important muscle:1,2,3
- Insertion: the neck of the malleus
- Innervation: mandibular branch of the trigeminal nerve (cranial nerve V)
- Function: when contracting, it pulls the handle of the malleus medially to tense the tympanic membrane and reduces the amplitude of sound vibrations. This prevents damage to the internal ear when there are loud sounds.
Stapedius
This is the smallest muscle in the human body and is located in the pyramidal eminence; a hollow prominence on the posterior wall of the tympanic cavity:
- Insertion: the neck of stapes
- Innervation: stapedius is supplied by the facial nerve (cranial nerve VII)
- Function: when stapedius contracts it pulls stapes posteriorly and changes the shape of the oval window. This is to reduce the amplitude of sound vibrations reaching the internal ear, as a form of protection.
Eustachian tube
The eustachian tube, also called the pharyngotympanic tube, connects the middle ear to the nasopharynx. Like these two areas, it is also lined with a mucous membrane.
This tube is shorter and straighter in children, so it is easier for pathogenic organisms to travel between the ear and nasopharynx. This is one factor contributing to infections of the middle ear in children.
Innervation
Branches of the tympanic plexus, which is formed by fibres of the glossopharyngeal nerve (cranial nerve IX) and sympathetic fibres from the carotid plexus.
Blood supply
Arterial blood supply to the eustachian tube consists of the:
- Ascending pharyngeal artery, a branch of the external carotid artery
- Middle meningeal artery and the artery of the pterygoid canal, both branches of the maxillary artery
Blood from the eustachian tube drains into the pterygoid venous plexus.
Function of the eustachian tube10
The function of the eustachian tube is to aerate the middle ear to equalise pressure for optimum movement of the tympanic membrane.
It also equalises pressure in the middle ear to that of the atmospheric pressure. This allows for optimal transmission of sound waves from the atmosphere to the inner ear.
In addition, it allows for air exchange within the middle ear.
Clinical significance: Otitis media with effusion11
Otitis media with effusion (OME), commonly known as glue ear, involves effusion in the middle ear, without any acute signs or symptoms of infection.
Glue ear is more common in children because the eustachian tube is shorter and straighter.
Typical symptoms of OME include:
- Conductive hearing loss
- A feeling of fullness in the ear
- Tinnitus
- Balance issues
Diagnosis is usually made by direct visualisation using otoscopy; typical findings include an air-fluid level and/or dullness of the tympanic membrane due to the brownish colour of the effusion.
Glue ear is usually managed by active observation for three months, as most cases will resolve spontaneously. If it persists, treatment options include hearing aids and grommet insertion.
Inner ear
The inner ear is the home of the vestibulocochlear organs, the organs that are responsible for receiving sound waves and converting them into electrical signals to be interpreted by the brain and maintaining balance by recognising the position and movement of the body.
Within the inner ear, there are two types of labyrinth. The membranous labyrinth is a series of membranous ducts and sacs that contains the endolymph of the inner ear.1,2,3 This is found within the bony labyrinth, a series of bony cavities, which is filled with perilymph.
The endolymph and perilymph contain different concentrations of ions, which allows for the transmission of action potentials to the brain to allow for the interpretation of sound and balance. A detailed discussion of this process is beyond the scope of this article.
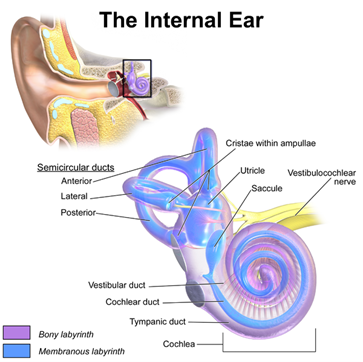
Bony labyrinth
The bony labyrinth is formed from the vestibule, the three semi-circular canals and the cochlea.
The vestibule is the central part of the bony labyrinth and communicates anteriorly with the cochlea, postero-superiorly with the semi-circular canals and with the oval window. Within the vestibule are the saccule and utricle, the organs of balance. The saccule and utricle detect linear motion.
Within each ear, there are three semi-circular canals: anterior, posterior and lateral, which are organised so that each canal is at a right angle to the others. Within the semi-circular canals are the semi-circular ducts, which, along with the utricle and saccule, form the organs of balance. At the end of each canal, there is a swelling called the ampulla.
The cochlea is located anterior to the vestibule. This structure twists on itself around a central column of bone called the modiolus, to become cone-shaped with a base (essentially like a snail shell) which is located near the internal acoustic meatus, where there are branches of the vestibulocochlear nerve (cranial nerve VIII).
Within the cochlea is the cochlear duct, the organ of hearing. The cochlear duct forms two perilymph filled canals that extend throughout the cochlea:
- The scala vestibuli: this is continuous with the vestibule
- The scala tympani: this is ends at the round window
Membranous labyrinth
This is a continuous system of ducts and sacs within the bony labyrinth. It contains endolymph and is surrounded by perilymph.
Within the membranous labyrinth are four ducts (three semicircular ducts and the cochlear duct) and two sacs (utricle and saccule). These semicircular ducts and utricle and saccule work together to form the organs of balance, whilst the cochlear duct is the organ of hearing.
Utricle and saccule
The utricle is the larger of the two sacs and is located in the posterior-superior part of the vestibule. It has an ovular irregular shape and receives drainage from the semicircular ducts. The utricle is responsible for detecting linear acceleration in the horizontal plane (e.g. moving the head forwards and backwards without tilting).
The saccule is a smaller, more rounded sac that is located on the anterior-inferior side of the vestibule. It receives its drainage from the cochlear duct. The saccule is responsible for detecting linear acceleration in the vertical plane (e.g. moving the head up and down without tilting)
Connecting both the utricle and saccule is the utriculosaccular duct, ensuring equilibrium between the two sacs. A branch of this duct is the endolymphatic duct, which allows for the drainage and reabsorption of endolymph in the posterior cranial fossa.
The utricle and saccule can detect linear movement due to sensory receptors that are organised into the macule of both organs.
Semicircular ducts
As mentioned above, the semicircular ducts are found within the semicircular canals of the bony labyrinth and share the same orientation as their canal. These ducts detect rotational movement in any direction (e.g. tilting the head sideways or flexing/extending the neck).
The semicircular ducts can detect these rotatory movements due to sensory receptors located in the crista of the ampulla of each duct. When we rotate our head, the endolymph within these ducts changes in speed and/or direction. This change is detected by these sensory receptors, which transmits this information to the brain.
Cochlear duct
As mentioned above, the cochlear duct is located in the centre of the cochlea, dividing it into the scala vestibuli and scala tympani.
It is held in this central position by the lamina of the modiolus. This creates a triangular shape which consists of:
- Roof: Reissner’s membrane – this separates the endolymph in the cochlear duct from the perilymph of the scala vestibuli
- Floor: Basilar membrane – this separates the endolymph in the cochlear duct from the perilymph in the scala tympani
- Lateral wall: formed by the spiral ligament; a wall of thickened, epithelial-lined periosteum
Within the basilar membrane is the Organ of Corti, which contains the specialised epithelial cells that are responsible for converting the mechanical sound waves into electrical impulses that can be interpreted by the brain as sound.
Innervation of the inner ear
The inner ear is innervated by the vestibulocochlear nerve (cranial nerve VIII). This nerve originates from the lateral surface of the brainstem and travels through the temporal bone in the internal acoustic meatus to innervate the inner ear.
Once in the internal acoustic meatus, the nerve divides to form the:
- Vestibular nerve: this enlarges to form the vestibular ganglion before it divides into the superior and inferior vestibular nerve to innervate the three semi-circular ducts, the utricle and saccule.
- Cochlear nerve: this enters the base of the cochlea and passes through the modiolus to innervate the receptors of the Organ of Corti.
Blood supply of the inner ear
The blood supply of the inner ear can be split into the blood supply to the bony labyrinth and the bloody supply to the membranous labyrinth:
- The bony labyrinth is supplied by the anterior tympanic branch of the maxillary artery, the stylomastoid branch of the posterior auricular artery and the petrosal branch of the middle meningeal artery.
- The membranous labyrinth is supplied by the labyrinthine artery, a branch of either the basilar artery or anteroinferior cerebellar artery. This passes through the internal acoustic meatus where it divides into a cochlear branch and vestibular branch which supplies the cochlear duct and vestibular apparatus respectively.
The membranous labyrinth is drained by the labyrinthine vein, which drains into the inferior petrosal sinus or the sigmoid sinus.
Key points
- The ear can be divided into external, middle and inner parts.
- The external ear contains the auricle, external auditory meatus and tympanic membrane. These structures all work together to conduct and amplify sound waves into the middle ear.
- The middle ear contains the auditory ossicles, these transmit sound waves to the inner ear. The muscles that attach to these ossicles are important in controlling the amplitude of these sound waves in order to prevent damage.
- Also in the middle ear is the opening of the eustachian tube which serves as a connection between the middle ear and nasopharynx, to equalise pressure within the middle ear to atmospheric pressure.
- The inner ear is formed of the bony and membranous labyrinth. These contain the semicircular ducts, utricle and saccule, which are involved in maintaining balance. The cochlear duct, which is found within the cochlea, is responsible for converting sound waves into electrical signals, to be processed by the brain.
Reviewer
ENT consultant
Editor
Dr Chris Jefferies
References
- Gray’s Anatomy for Students, Fourth Edition.
- Moore’s essential clinical anatomy, Sixth Edition.
- Netter’s clinical anatomy, Fourth Edition
- University of Dundee. Anatomy of the external ear. Licence: [CC BY-NC-ND]
- Anatomy Next. External Acoustic Meatus. Available from: [LINK]
- Alice Szymanski et al. Anatomy, head and neck, ear tympanic membrane. Published in 2021. Available from: [ LINK]
- BMJ Best Practice. Otitis Externa. Published in 2021. Available from: [LINK]
- Wikimedia Commons. Anatomy of the middle ear. Licence: [CC BY-SA]
- Tom George et al. Anatomy, head and neck, ear ossicles. Published in 2021. Available from: [LINK
- Alice Szymaski et al. Anatomy, Head and Neck, Ear Eustachian Tube. Published in 2021. Available from: [LINK]
- Up to Date. Otitis media with effusion (serous otitis media) in children: clinical features and diagnosis. Published in 2021. Available from: [LINK]
- Wikimedia Commons. Anatomy of the inner ear. Licence: [CC BY]
