
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
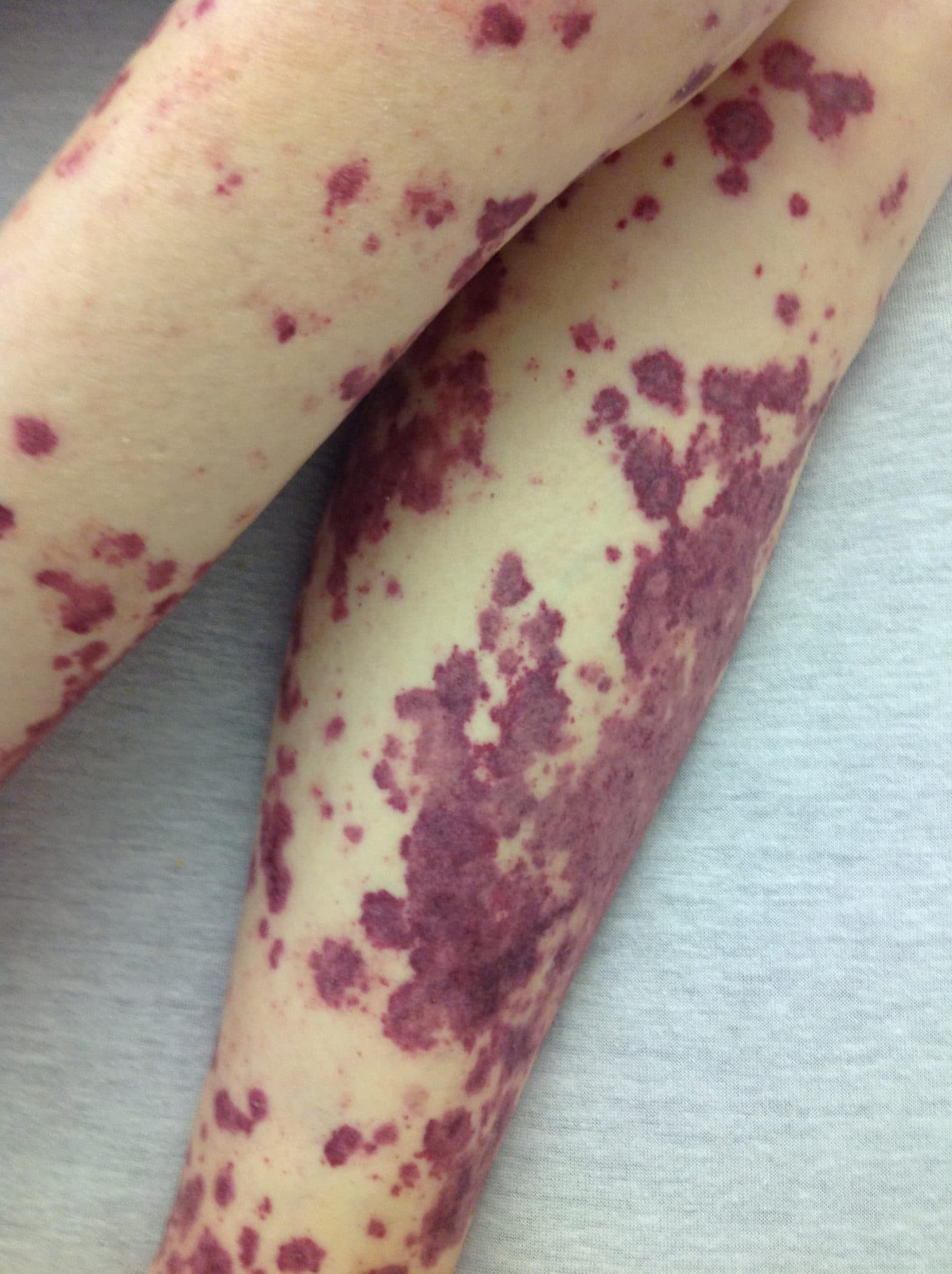
Non-blanching rashes are caused by small bleeds in the vessels beneath the skin, giving a purplish discolouration.
Depending on the size of the individual lesions they can be defined as:
- Petechiae: <5mm diameter (figure 1).
- Purpura: 5-10mm diameter (figure 2).
- Ecchymoses: >1cm diameter (figure 3).


This article will cover common causes of non-blanching rashes, including:
- Meningococcal sepsis
- Henoch-Schönlein purpura
- Idiopathic thrombocytopaenic purpura
- Haemolytic uraemic syndrome
- Forceful coughing/vomiting
- Non-accidental injury
Meningococcal sepsis
Aetiology
Meningococcal meningitis is a central nervous system infection commonly caused by Neisseria meningitides, a gram-negative diplococcus and commensal of the nasopharynx.
Meningococcal sepsis is a complication of meningitis which occurs when the infection moves beyond the central nervous system into the blood.
Risk factors
Meningococcal meningitis is most common in children under 5 years of age. A second smaller peak has been recognised in 14-19-year-olds.
Clinical features
History
Typical symptoms of meningococcal sepsis include:
- Fever
- Neck stiffness
- Confusion and/or seizures
Clinical examination
If meningitis/meningococcal sepsis is suspected, patients should undergo a thorough examination and the skin should be assessed for any rashes.
Important findings on examination include:
- Kernig’s sign (pain and resistance on passive knee extension with hips fully flexed)
- Brudzinski’s sign (knees and hips flex on bending the head forward)
- Non-blanching rash
- Photophobia
- Hypovolaemic shock: low blood pressure, high heart rate, capillary refill time >2s, the skin may look mottled
Investigations
Investigations must not delay treatment. They may include:
- Baseline blood tests (FBC, CRP, U&E, clotting): inflammatory markers may be raised.
- Blood cultures: may identify a causative organism.
- Pharyngeal swab: to screen for the presence of Neisseria meningitides in the pharynx.
- Lumbar puncture: the definitive investigation to diagnose meningococcal meningitis.
Management
This is an emergency and the patient will need immediate transfer to hospital.
Antibiotics need to be given immediately. If the patient is seen in primary care intramuscular benzylpenicillin can be given whilst awaiting transfer to hospital.
Local microbiology guidelines should be followed. Generally, initial empirical therapy is:
- Intravenous cefotaxime and amoxicillin in patients under 3 months.
- Intravenous ceftriaxone in patients over 3 months old.
In addition, corticosteroids (e.g: intravenous dexamethasone) is given in those over 3 months old to reduce neurological complications.
Complications
If not diagnosed and treated swiftly complications can include:¹
- Seizures
- Raised intracranial pressure and hydrocephalus
- Disseminated intravascular coagulation leading to multi-organ failure and even death
For more information on meningitis, see the Geeky Medics article here.
Henoch-Schönlein purpura (HSP)
Aetiology
Henoch-Schönlein purpura (HSP) is an IgA mediated vasculitis of unknown aetiology. It tends to occur post-infection with the most common trigger being group A streptococci.²
Risk factors
Risk factors for HSP include:
- Age: most cases occur in children under 10 years of age with a peak of cases between 4-6 years old.
- Season: usually occurs in autumn/winter months.
Clinical features
History
Typical symptoms of HSP include:
- A prodromal mild upper respiratory tract illness or gastrointestinal infection
- Generalised abdominal pain
- Bloody diarrhoea
- Nausea and vomiting
- Joint pain
Clinical examination
Patients with suspected HSP require an abdominal examination and examination of the affected skin.
Typical clinical findings in HSP include:
- Low-grade fever
- Symmetrical rash on the back of the legs, buttocks and arms (Figure 1)
The macular rash begins as erythematous and then becomes purpuric and raised.

Differential diagnoses
In young children, consider intussusception which also presents as bloody diarrhoea and abdominal pain. Intussusception can also be a complication secondary to HSP.
Investigations
The diagnosis of HSP is mainly clinical, however, the following investigations should be performed.
- Urinalysis: to test for the presence of haematuria or proteinuria.
- Baseline blood tests (FBC, CRP, U&E, LFT): may be helpful in aiding diagnosis.
- Skin biopsy: can be considered if there is doubt surrounding the origin of the rash.
If there is concern regarding intussusception, an abdominal ultrasound should be arranged.
Management
Most cases resolve with no intervention. However, hospital admission may be necessary for patients with renal or abdominal complications.
Complications
It is common for HSP to recur. This can happen in one-third of patients.²
Complications of HSP include:
- Nephrotic or nephritic syndrome
- Renal failure
- Intussusception
Immune thrombocytopenic purpura (ITP)
Immune thrombocytopaenic purpura (ITP) involves the development of a purpuric rash in those with low circulating platelets (<100 x 10⁹/L) in the absence of any clear cause.3
Risk factors
ITP usually follows a viral illness in children however, there are no known specific risk factors in adults.
Clinical features
History
Typical symptoms of ITP include:
- Prodromal viral illness in children
- Epistaxis
Many patients may be asymptomatic.
Clinical examination
Typical clinical findings in ITP include:
- Petechiae and/or bruising
Differential diagnoses
- Meningococcal sepsis
- Aplastic anaemia
- Leukaemia
- Non-accidental injury
- Disseminated intravascular coagulation
Investigations
Investigations may include:
- Baseline blood tests (FBC) and blood film: will show thrombocytopenia.
- Bloodborne virus screen (HIV, hepatitis C): to exclude secondary cause of ITP.
- Bone marrow biopsy: if the diagnosis is uncertain.
Management
In children, ITP is usually self-limiting. Treatment is based upon symptoms, rather than the absolute platelet count. In practice, active treatment is rarely needed for platelet counts of >50×10⁹/L.
Patients should be referred to haematology.
Medical management
Medical management of ITP may include:⁴
- Stopping any medications which may affect platelets (e.g: nonsteroidal anti-inflammatories)
- Oral prednisolone is regarded as the first-line treatment
- Other treatments that may be offered include intravenous immunoglobulins (IVIG) or monoclonal antibodies such as rituximab.
Surgical management in the form of a splenectomy can be considered once all medical treatment options have been exhausted.⁴
Haemolytic uraemic syndrome (HUS)
Haemolytic uraemic syndrome (HUS) is defined as a triad of: 5
- Microangiopathic haemolytic uraemia
- Acute kidney injury
- Thrombocytopaenia
Aetiology
HUS occurs after infection with Escherichia coli O157; this pathogen is commonly found in the faeces of sheep, cows and goats.
A potential source of infection is petting zoos, improper hand hygiene during these visits can lead to infection with E.Coli O157.
Risk factors
Common risk factors for HUS include:
- Age: young children are by far the most commonly affected by HUS particularly between the ages of 6 months to 5 years.
- Immunocompromised adults and the elderly population are also at increased risk.
- The number of infections tends to peak in the summer months.
Clinical features
History
Typical symptoms of HUS include:
- Diarrhoea, which typically turns bloody around day three
- Abdominal pain
- Fever
- Vomiting
During history taking it is also important that you cover any recent exposure to farm animals and if the child attends school or playgroup.
Clinical examination
Patients with suspected HUS require an abdominal examination and examination of the affected skin.
Typical clinical findings in HUS include:
- Abdominal tenderness
- Hypertension secondary to acute kidney injury
- Small petechiae on the skin can occur due to low platelet count
Differential diagnoses
HUS can appear similar to several conditions including:
- Acute gastroenteritis
- Intussusception
- Disseminated intravascular coagulation
Investigations
Investigations may include:
- Baseline blood tests (FBC, U&E, CRP, clotting): may show thrombocytopenia, raised WCC, anaemia and acute kidney injury.
- Urinalysis: to screen for haematuria and proteinuria.
- Stool cultures: to screen for the presence of E.Coli O157.
Management
The treatment of HUS is mainly supportive, the mainstay of treatment is the maintenance of fluid balance and correction of electrolyte abnormalities. Severe cases may lead to the development of renal failure requiring dialysis.
HUS is a notifiable disease to Public Health England, and should be reported to them within 3 days.⁶
Forceful coughing and/or vomiting
Forceful coughing or vomiting can cause petechiae to appear on the skin in the superior vena cava distribution, which is the head, neck and the top of the shoulders.
Other serious causes of petechiae should be excluded before they are attributed to forceful coughing or vomiting.
No management is needed and the petechiae should self-resolve.
Non-accidental injury
When assessing children with non-blanching rashes it is important to consider the possibility of a non-accidental injury (NAI).
Certain distributions of ‘rashes’ should be suspicious for this such as hand marks, linear markings and those on the face/ears. They usually occur with other signs of NAI so careful examination is necessary.⁷
For more information on NAI, see the Geeky Medics article here.
Reviewer
Dr Thomas King
Dermatology SpR
Editor
Dr Chris Jefferies
References
Text references
- Patient Professional. Meningitis. Last updated July 2019. Available from: [LINK]
- Patient Professional. Henoch-Schonlein Purpura. Last updated June 2019. Available from: [LINK]
- Patient Professional. Immune Thrombocytopaenia. Last updated February 2015. Available from: [LINK]
- NICE. Immune (idiopathic) thrombocytopenic purpura: rituximab – Evidence Summary. Last updated October 2014. Available from: [LINK]
- Patient Professional. Haemolytic Uraemic Syndrome. Last updated February 2016. Available from: [LINK]
- Public Health England. List of Notifiable Diseases. Last updated March 2020. Available from: [LINK]
- DermNet. Skin signs of Non-Accidental Injury. Last updated in 2010. Available from: [LINK]
Image references
- Figure 1. Hektor. Purpura. License: [CC-BY-SA]. Available from: [LINK]
- Figure 2. DrFO.Jr.Tn. Petechial rash. License: [CC-BY-SA]. Available from: [LINK]
- Figure 3. Rosetheboston. Post gallbladder surgery bruise. License: [CC-BY-SA]. Available from: [LINK]
- Figure 4. Madhero88. Henoch-Schonlein purpura. License: [CC-BY-SA]. Available from: [LINK]
