

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
The wrist joint connects the distal end of the radius to the carpal bones in the hand. It is a synovial joint, meaning the bones are separated by a narrow cavity filled with synovial fluid.
The wrist joint is an articulation of the distal head of the radius, the articular disc that overlies the distal ulna, and the proximal carpal bones of the hand (scaphoid, lunate and triquetrum). The carpal bones are arranged in a convex formation, whereas the other articular surface is concave.
The main movements of the wrist are flexion and extension and to a lesser degree abduction and adduction of the hand. Due to the radial styloid process extending more distal than the ulnar styloid, the hand can be adducted more than it can be abducted.
Bony structure
The wrist joint involves the distal head of the radius, scaphoid, lunate and triquetrum. The ulna is not directly involved as it is covered by a layer of cartilage which acts as the articulating surface.
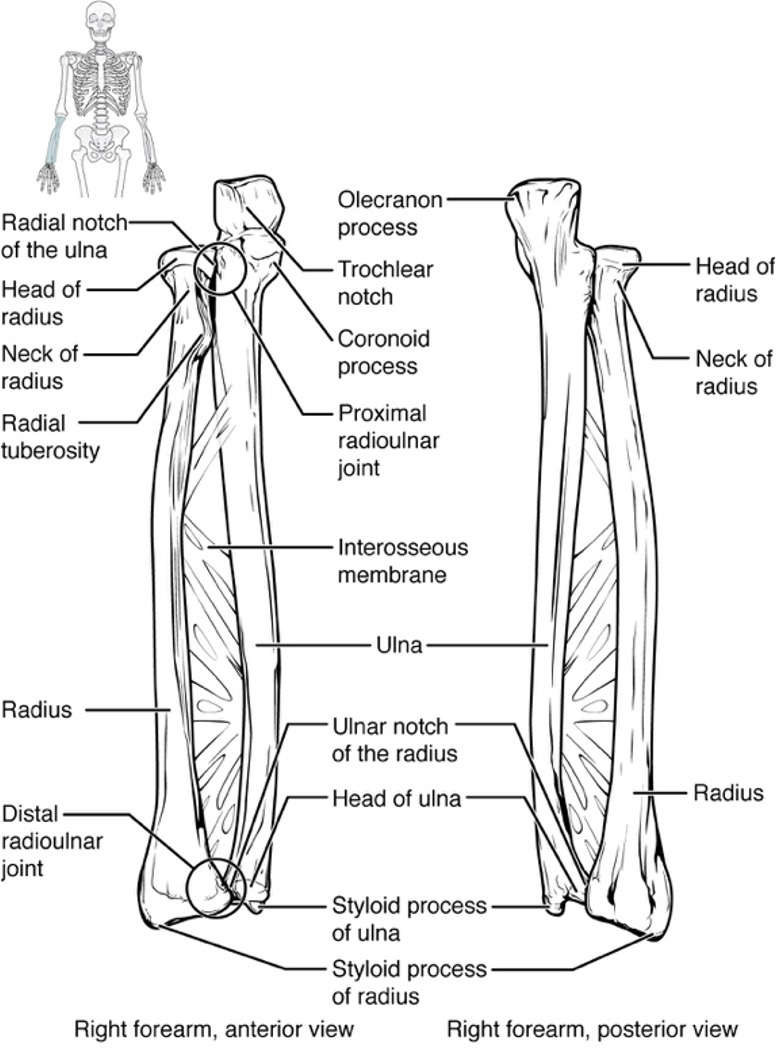
Radius
Proximal articulation: capitulum of humerus
Distal articulation: scaphoid and lunate (carpal bones)
The radius is the site of insertion for several muscles of the forearm, which act to move the hand and wrist.
Ulna
Proximal articulation: trochlea of the humerus
Distally, the ulna is covered by a layer of articular cartilage which then articulates with the carpal bones.
The ulna is not directly involved in the wrist joint but forms the distal radioulnar joint.
Clinical relevance: Colles’ fracture4
Colles’ fracture is the most common type of distal radius fracture and is commonly caused by a fall on an outstretched hand (FOOSH). This type of fracture is common in patients with osteoporosis. Young patients sustain Colles’ fractures in high-impact trauma, such as contact sports.
On plain X-ray, Colles’ fracture can be diagnosed if there is a fracture of the distal radius with posterior displacement of fragments. In up to 50% of cases, there is also a fracture of the ulnar styloid process.
Management of Colles’ fracture involves closed reduction and cast immobilisation, as well as pharmacological bone protection for those at risk of osteoporosis. For more information, see the Geeky Medics guide to wrist fractures.
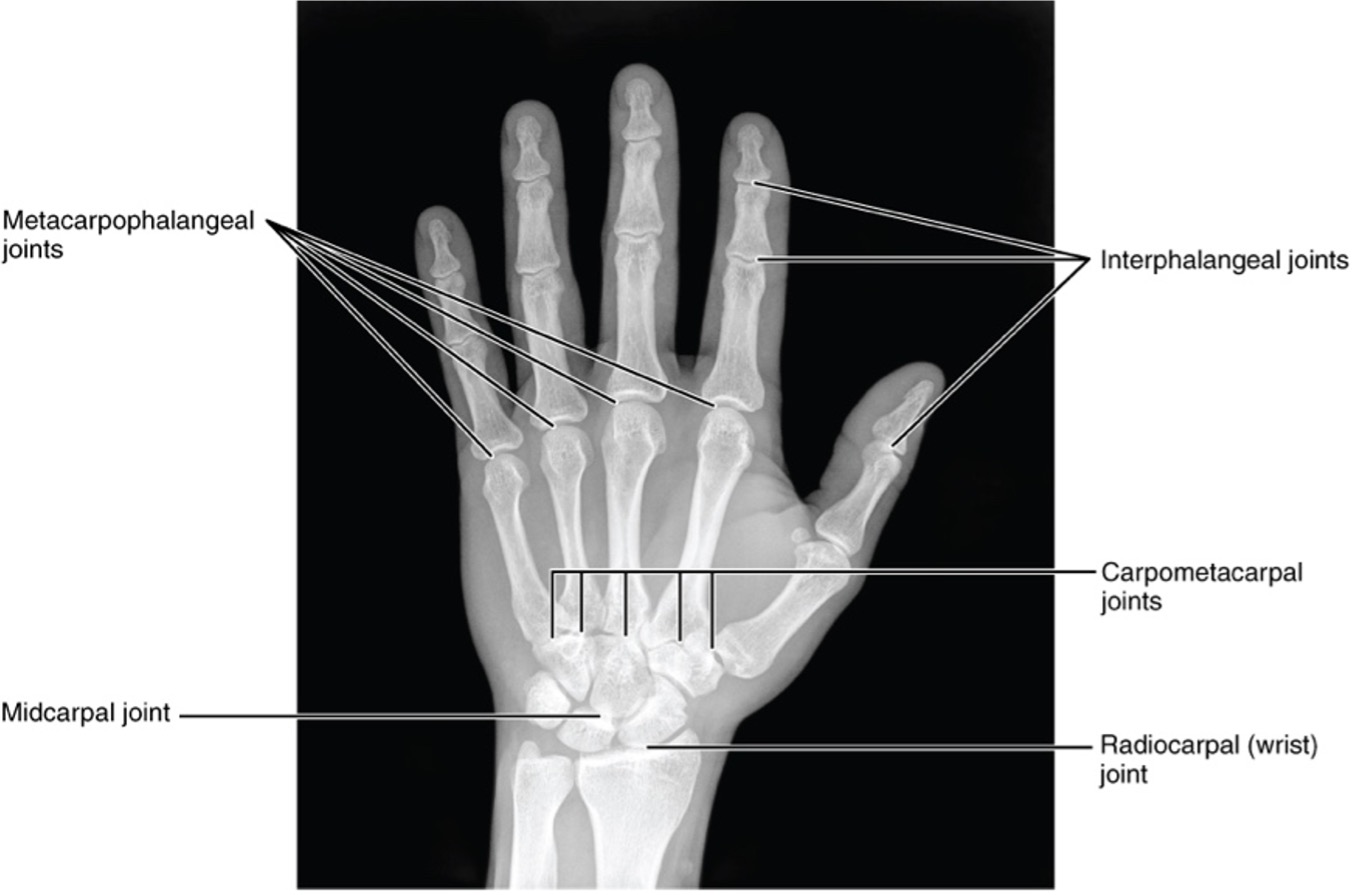
Carpal bones
The scaphoid and lunate articulate with the radius. The triquetrum articulates with the layer of cartilage that overlies the distal end of the ulna.
For more information, see the Geeky Medics guide to the bones of the hand.
Clinical relevance: Scaphoid fractures3
The scaphoid is the most commonly fractured carpal bone, and fractures most commonly occur at the waist of the scaphoid. This most commonly occurs following a fall onto an outstretched hand (FOOSH).
Scaphoid fractures are particularly common in the elderly, and those with osteoporosis. Symptoms include pain and tenderness just below the base of the thumb and loss of pinch and grip strength.
Scaphoid fractures may be complicated by avascular necrosis, as the majority of its blood supply comes from the radial artery. The artery enters the distal part of the bone to supply the proximal portion, and therefore in fractures the blood supply to the proximal bone can become cut off, causing necrosis.
Movements of the wrist
Movement of the wrist is brought about by muscles in the forearm. For more information, see the Geeky Medics guide to the muscles of the anterior forearm and muscles of the posterior forearm.
Table 1. An overview of the movements of the wrist.
| Compartment | Layer | Muscle | Action |
|
Anterior |
Superficial |
Flexor carpi ulnaris |
Flexion and adduction |
|
Palmaris longus* |
Flexion |
||
|
Flexor carpi radialis |
Flexion and abduction |
||
|
Pronator teres |
Pronation |
||
|
Intermediate |
Flexor digitorum superficialis |
Flexion |
|
|
Deep |
Flexor digitorum profundus |
Flexion |
|
|
Pronator quadratus |
Pronation |
||
|
Posterior |
Superficial |
Extensor carpi radialis longus |
Extension and abduction |
|
Extensor carpi radialis brevis |
Extension and abduction |
||
|
Extensor digitorum |
Extension |
||
|
Extensor carpi ulnaris |
Extension and adduction |
||
|
Deep |
Supinator |
Supination |
*This muscle is absent in approximately 15% of the population.
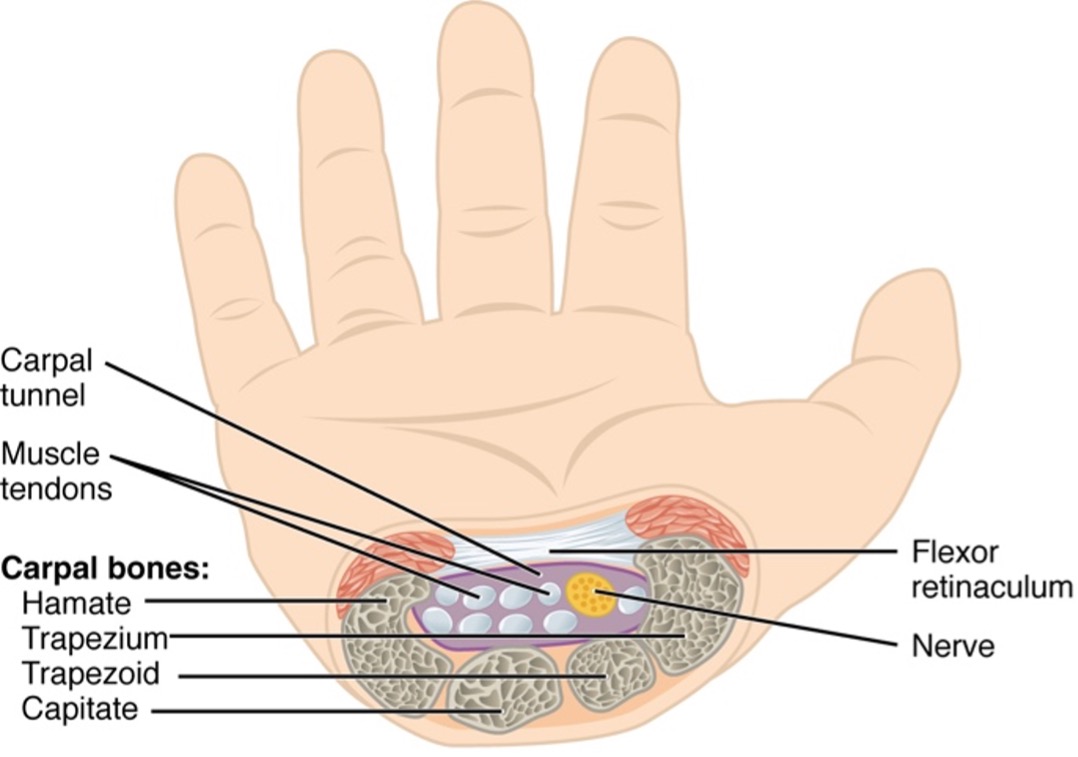
The carpal tunnel
One of the most clinically important aspects of the wrist joint is the carpal tunnel. This is formed on the anterior aspect of the wrist, by the flexor retinaculum superiorly and the deep arch of the carpal bones inferiorly.
The bones that make up the deep arch include the hamate, capitate, trapezoid and trapezium.
The flexor retinaculum is a thick ligament made of connective tissue.
The carpal tunnel contains tendons of flexor digitorum superficialis (4), flexor digitorum profundus (4) and flexor pollicus longus, which act to move the digits. The carpal tunnel also contains the median nerve.
Clinical relevance: Carpal tunnel syndrome
The carpal tunnel is a small space, meaning its contents can easily be compressed. Symptoms of carpal tunnel syndrome are produced due to compression of the median nerve.
Carpal tunnel syndrome may be idiopathic, meaning there is no obvious cause, or may result due to inflammation and swelling of the tendons and tendon sheaths. Common causes of carpal tunnel include rheumatoid arthritis, pregnancy and repetitive use of the tendons.
Symptoms of carpal tunnel syndrome include pain and pins and needles in the hand, as well as weakness of the thenar muscles. There are two important signs that help to identify carpal tunnel:
- Tinel’s sign: tapping over the area reproduces symptoms
- Phalen’s sign: symptoms are triggered by wrist flexion
Treatment of carpal tunnel syndrome includes wrist splinting, particularly at night, as well as corticosteroid injections into the space.
Severe cases may be treated with decompressive surgery involving division of the flexor retinaculum. For more information, see the Geeky Medics guide to carpal tunnel syndrome.
Other structures in the wrist
There are many other tendons, blood vessels and nerves that pass through the wrist into the hand.
Superficial to the flexor retinaculum, the ulnar nerve, ulnar artery, and palmaris longus tendon enter the hand. Posteriorly to the carpal bones, the remaining tendons enter, along with the radial artery.
Editor
Dr Chris Jefferies
References
- Richard Drake, A. Wayne Vogl, Adam Mitchell. Gray’s Anatomy for Students (4th Edition). Published in 2019. Available from: [LINK]
- OpenStax. Anatomy and Physiology. Published in 2013. Available from: [LINK]
- Bertrand Jones, Tamara D. Rozental. OrthoInfo. Scaphoid Fracture of the Wrist. Published in March 2016. Available from: [LINK]
- Bahman Rasuli, Paresh Desai. Radiopaedia. Colles’ fracture. Available from: [LINK]
- Katherine Faust, Charles D. Jennings. OrthoInfo. Carpal Tunnel Syndrome. Published in July 2016. Available from: [LINK]
Image references
- OpenStax. Anatomy and Physiology. Ulna and Radius. April 2013. License: [CC-BY-SA]
- OpenStax. Anatomy and Physiology. Bones of the Hand. April 2013. License: [CC-BY-SA]
- OpenStax. Anatomy and Physiology. Carpal Tunnel. April 2013. License: [CC-BY-SA]
