

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
An inguinal hernia is an abnormal protrusion of abdominopelvic contents through the superficial inguinal ring into the groin. The superficial inguinal ring lies above the pubic tubercle and marks the end-point of the inguinal canal.
Inguinal hernias are by far the most common type of hernia. Patients often present with a lump in the groin that comes and goes and has slowly increased in size over time.
Inguinal hernias can be direct or indirect:
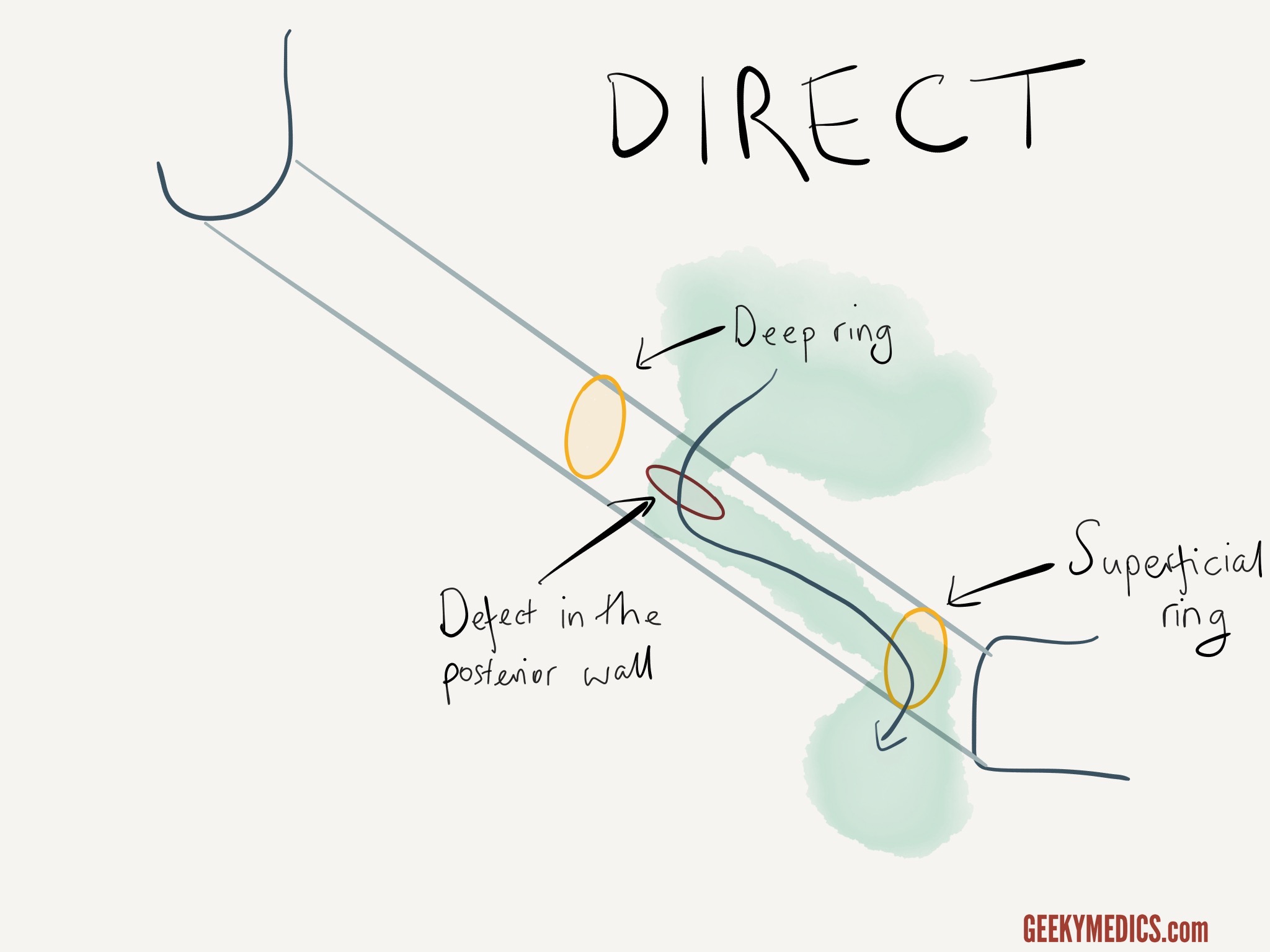
- Direct: abdominal contents are forced through a weakness in the posterior wall of the inguinal canal
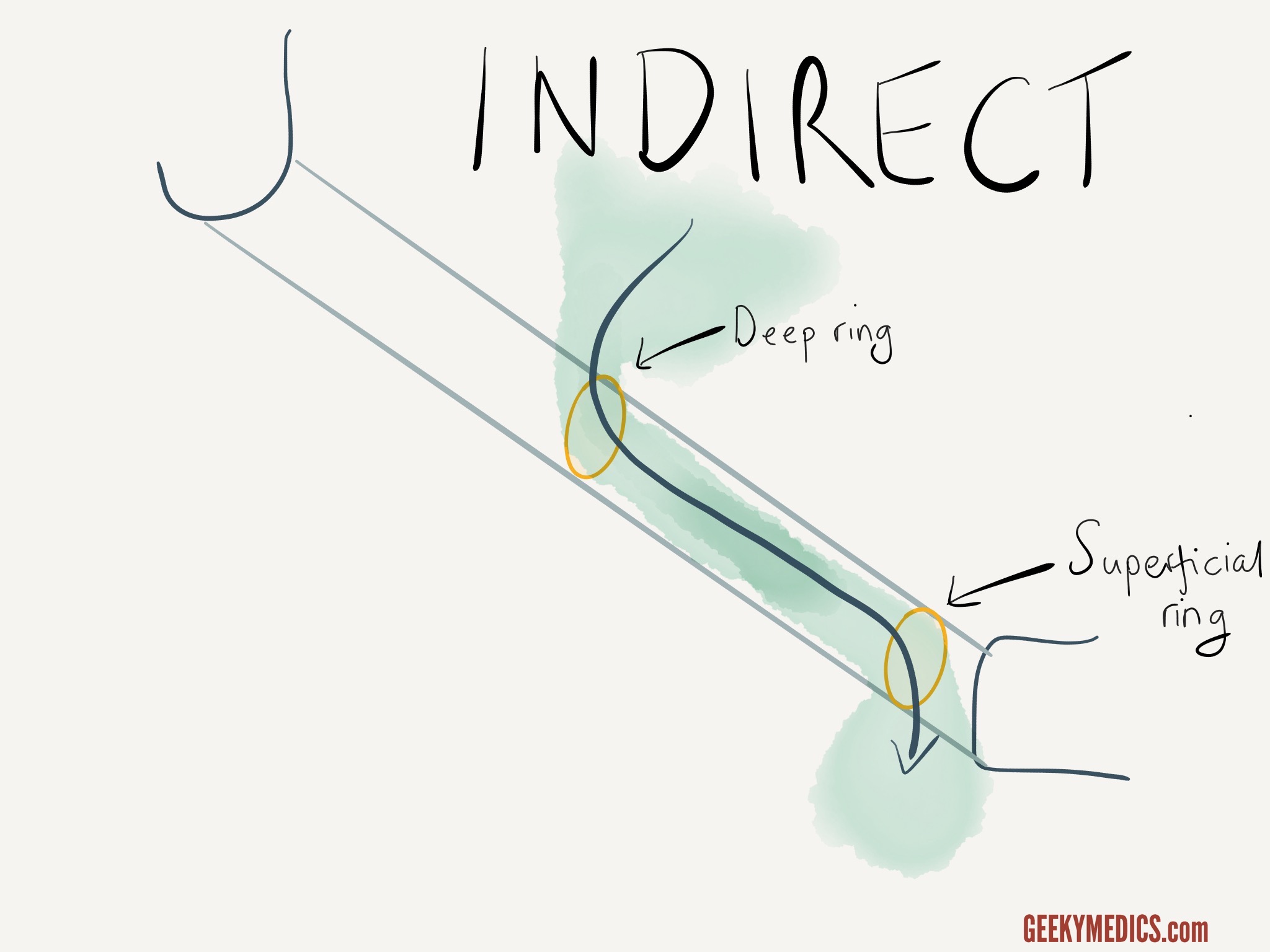
- Indirect: abdominal contents enter the deep ring (the start) of the inguinal canal
In both types of inguinal hernia, abdominal contents exit through the superficial ring of the inguinal canal and can sometimes enter the scrotum. This is known as an inguinoscrotal hernia. It is much more common for indirect hernias to do this as the path through both anatomical inguinal rings offers less resistance.
Direct inguinal hernia
A direct inguinal hernia is caused by a weakness in the posterior wall of the inguinal canal in an area known as Hesselbach’s triangle.
Abdominal contents (usually just fatty tissue, sometimes bowel) are forced “directly” through this defect into the inguinal canal.
The abdominal contents enter the canal medial to the deep ring and exit via the superficial ring.
Indirect inguinal hernia
An indirect inguinal hernia follows a different trajectory.
Instead of piercing the posterior wall, the abdominal contents enter the deep ring (the start of the inguinal canal), pass along the length of the inguinal canal and exit via the superficial ring.
How to distinguish direct vs indirect inguinal hernia
Direct and indirect inguinal hernias are managed in the same way (usually a mesh repair). Distinguishing between direct and indirect inguinal hernias on hernia examination has limited clinical use and is unreliable. However, it can help you understand the anatomical concepts.
If you place your finger over the deep inguinal ring (just above the mid-point of the inguinal ligament), you can control an indirect inguinal hernia that has been reduced (in other words, the hernia does not reappear).
If you press the deep ring and the hernia still protrudes, then the hernia is emerging via a defect in the posterior wall medial to this point and is, therefore, a direct hernia.
Technique
1. Locate the deep inguinal ring (midway between the anterior superior iliac spine and pubic tubercle).
2. Manually reduce the patient’s hernia by compressing it towards the deep inguinal ring, starting at the inferior aspect of the hernia.
3. Once the hernia is reduced, apply pressure over the deep inguinal ring and ask the patient to cough.
If a hernia reappears, it is more likely to be a direct inguinal hernia; if it does not, it is more likely to be an indirect inguinal hernia.
Editor
Dr Chris Jefferies
