

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
The extraocular muscles (EOM) are responsible for controlling the movements of the eyeball and upper eyelid. These muscles are also known as the extrinsic eye muscles, distinguishing them from intrinsic eye muscles which are responsible for controlling the movement of the iris. This article will discuss the anatomy of the EOM including their relevant attachments, innervation and actions.
It is useful to classify the extraocular muscles into two sub-groups; muscles that move the eye and muscles that move the upper eyelid. We discuss both groups below.
Muscles responsible for the movement of the eye
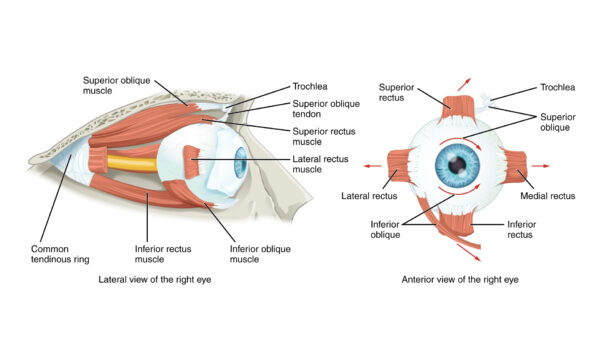
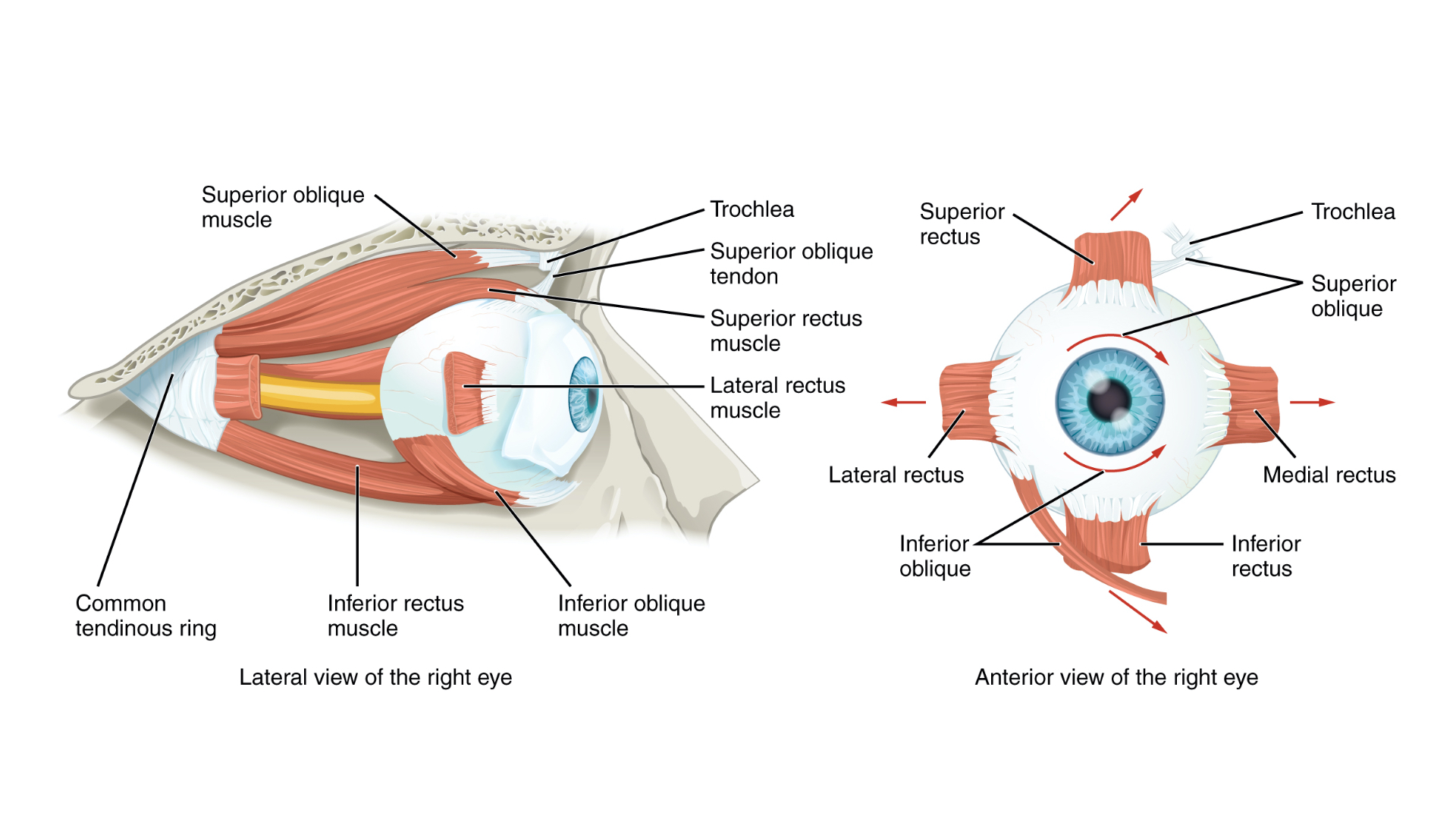
This group contains six muscles; four muscles that run almost a straight course from origin to insertion and hence are called recti (Latin for straight), and two muscles that run a diagonal course, the oblique muscles.
Recti muscles
There are four recti; superior, inferior, medial, and lateral. They all share a common origin, a fibrous ring of connective tissue located posteriorly at the apex of the orbit, called the tendinous ring or the annulus of Zinn.
Superior rectus
- Origin: the superior aspect of the common tendinous ring
- Insertion: the anterosuperior aspect of the sclera of the eye
- Primary action: elevates the eye (directs the eye upwards)
- Secondary action: assists with medial rotation and adduction
- Innervation: oculomotor nerve (CN III)
Inferior rectus
- Origin: the inferior aspect of the common tendinous ring
- Insertion: the anteroinferior aspect of the sclera of the eye
- Primary action: depresses the eye (directs the eye downwards)
- Secondary action: assists with lateral rotation and adduction
- Innervation: oculomotor nerve (CN III)
Medial rectus
- Origin: the medial aspect of the common tendinous ring
- Insertion: the anteromedial aspect of the sclera of the eye
- Primary action: adducts the eye
- Innervation: oculomotor nerve (CN III)
Lateral rectus
- Origin: the lateral aspect of the common tendinous ring
- Insertion: the anterolateral aspect of the sclera of the eye
- Primary action: abducts the eye
- Innervation: abducens nerve (CN VI)
Oblique muscles
There are two oblique muscles, the superior and inferior oblique. They do not originate from the common tendinous ring but rather have bony origins within the orbital cavity.
Superior oblique
- Origin: the body of the sphenoid bone (posterior wall of the orbital cavity)
- Insertion: it travels across the medial edge of the roof of the orbit and then hooks around the trochlea, a pully-like structure at the superior-medial corner of the orbital cavity. After hooking around the trochlea it turns posteriorly to be inserted into the posterior-lateral quadrant of the superior surface of the sclera.
- Action: medial rotation, depression and abduction
- Innervation: trochlear nerve (CN IV)
Inferior oblique
- Origin: the inferomedial aspect of the orbital floor
- Insertion: lateral aspect of the inferior surface of the sclera, posterior to the lateral rectus
- Action: lateral rotation, elevation and abduction
- Innervation: oculomotor nerve (CN III)

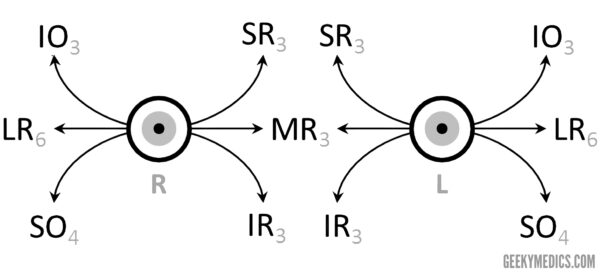
Mnemonic
A useful mnemonic for remembering the nerve supply to the extraocular muscles is:
LR6SO4AO3
- LR = Lateral rectus: innervated by the sixth nerve
- SO = Superior oblique: innervated by the fourth nerve
- AO = All other extraocular muscles: innervated by the third nerve

Levator palpebrae superioris
The levator palpebrae superioris is a solitary triangular-shaped muscle responsible for elevation of the superior eyelid (striated muscle). Levator palpebrae superioris also contains smooth muscle fibres which are known as the superior tarsal muscle.
- Origin: the lesser wing of the sphenoid bone
- Insertion: the superior tarsal plate of the upper eyelid
- Action: elevates the superior eyelid
- Somatic innervation: oculomotor nerve (CN III)
- Sympathetic innervation: sympathetic nerve fibres from the internal carotid artery pass within the superior division of the oculomotor nerve (CN III) to innervate the superior tarsal muscle

Clinical relevance: cranial nerve palsy
Damage to any of the three cranial nerves innervating the extraocular muscles can result in paralysis of the corresponding muscles.
Oculomotor nerve palsy (CN III)
The oculomotor nerve supplies all extraocular muscles except the superior oblique (CNIV) and the lateral rectus (CNVI). Oculomotor palsy (a.k.a. ‘third nerve palsy’), therefore, results in the unopposed action of both the lateral rectus and superior oblique muscles, which pull the eye inferolaterally. As a result, patients typically present with a ‘down and out’ appearance of the affected eye.
Oculomotor nerve palsy can also cause ptosis (due to a lack of innervation to levator palpebrae superioris) as well as mydriasis due to the loss of parasympathetic fibres responsible for innervating to the sphincter pupillae muscle.
Trochlear nerve palsy (CN IV)
The only muscle the trochlear nerve innervates is the superior oblique muscle. As a result, trochlear nerve palsy (‘fourth nerve palsy’) typically results in vertical diplopia when looking inferiorly, due to loss of the superior oblique’s action of pulling the eye downwards. Patients often try to compensate for this by tilting their head forwards and tucking their chin in, which minimises vertical diplopia. Trochlear nerve palsy also causes torsional diplopia (as the superior oblique muscle assists with intorsion of the eye when the head tilts). To compensate for this, patients with trochlear nerve palsy tilt their head to the opposite side, in order to fuse the two images.
Abducens nerve palsy (CN VI)
The abducens nerve (CN VI) innervates the lateral rectus muscle. Abducens nerve palsy (‘sixth nerve palsy’) results in unopposed adduction of the eye (by the medial rectus muscle), resulting in a convergent squint. Patients typically present with horizontal diplopia which is worsened when they attempt to look towards the affected side.
Reviewers
Dr James Nott
Anatomy Lecturer and Anatomy Lead for Geeky Medics
Dr Muhammad Shoaib
General Medicine Advanced Trainee
MRCP-UK
References
Text references
- Moore, K. L., Dalley, A. F., & Agur, A. M. (2013). Clinically oriented anatomy. Lippincott Williams & Wilkins.
- Snell, R. S. (2010). Clinical neuroanatomy. Lippincott Williams & Wilkins.
- D.J. Bell and A. Manickam et al. Radiopaedia: Extraocular muscle nerve supply mnemonic. [LINK]
Image references
1. Adapted by Geeky Medics. Au.yousef. Extraocular muscle actions and innervation. Licence: [CC BY-SA].
2. Openstax College. Extraocular muscles. Licence: [CC BY].
3. CFCF. The extrinsic eye muscles right eye lat. Licence: [CC BY-SA].
