
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
This OSCE guide provides a clear step-by-step approach to eliciting Hoffman’s sign.
Background
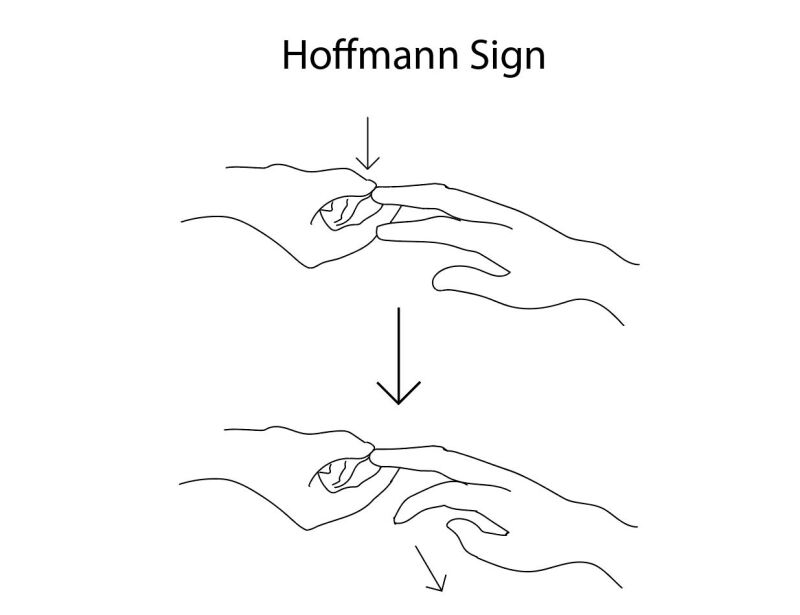
Hoffman’s sign is ‘‘…an involuntary flexion movement of the thumb and or index finger when the examiner flicks the fingernail of the middle finger down.’’1 This is considered abnormal and indicative of neural damage or irritation originating from the cervical spine.
Hoffman’s sign can aid in diagnosing cervical myelopathy or other upper motor neurone lesions.
- Cervical myelopathy refers to compression or damage to the spinal cord resulting from trauma or other pathological process. Degenerative cervical myelopathy (cervical spondylotic myelopathy) is the most common form.1 Common causes include disc degeneration, spinal stenosis, ligament ossification, and malignancy.2 Clinical features include impaired motor function, dexterity, and urinary incontinence, which are usually progressive.
- An upper motor neurone lesion refers to the impaired communication between the brain and spinal cord, also resulting from trauma or a pathological process. It may result from cervical myelopathy, an acquired injury, or a degenerative condition (e.g. brain injury, pyramidal tract lesions, metabolic and neurodegenerative disorders).3 For more information, see our guide to upper vs lower motor neurone lesions.
Clinical significance
The motor nerves originating from the cervical spine innervate muscles of the upper limbs, including the hand and digits. Cervical myelopathy or an upper motor neurone lesion can impair the motor reflex, causing a positive Hoffman’s sign.
However, a positive Hoffman’s sign has been reported in approximately 3% of the population without these conditions (a false-positive test).4 Therefore, a positive Hoffman’s sign does not confirm a diagnosis and further investigations are necessary.
The primary follow-up investigation to a positive Hoffman’s sign is imaging (CT or MRI scan) to establish a diagnosis. Treatments range from conservative management (e.g. physiotherapy, neck brace support, pain medication) to surgical management (e.g. decompression, cervical disc arthroplasty, laminectomy with fusion).5 Treatment choice depends on the duration and severity of signs and symptoms and the underlying cause(s).
Introduction
Wash your hands and don PPE if appropriate.
Introduce yourself to the patient, including your name and role.
Confirm the patient’s name and date of birth.
Briefly explain what the examination will involve using patient-friendly language.
Gain consent to proceed with the examination.
Ask the patient if they have any pain before proceeding with the clinical examination and perform a brief inspection for any wrist or hand deformities which could contradict the test.
Perform the test
1. Ask the patient to sit comfortably, look straight ahead (to avoid looking at the side being tested, which could compromise the results), and remain relaxed throughout the test
2. Using one hand, stabilise the patient’s wrist at the distal radioulnar joint in a prone position using your thumb and index finger
3. Using your opposite hand, clasp the patient’s third middle phalanx between your index and middle finger. Next, use your thumb to passively flex the distal interphalangeal joint (if the patient is not relaxed at this stage, instruct the patient to relax again or give the wrist a gentle shake before proceeding to step 4)
4. Slide your thumb off the end of the distal phalanx in a downward direction – this should cause the digit to ‘flick’ back into extension. This movement is rapid but gentle and should not cause any pain or discomfort
5. Observe for movement of the thumb or index finger.
6. Perform steps 1-4 on the opposite side and document your findings accordingly (e.g. “Positive left Hoffman’s sign as indicated by flickering of thumb and index finger…”)
Interpretation of findings
A positive test is when any involuntary flexion of the distal phalanx of the thumb or fingers occurs.4
A negative test is when none of the above signs are present.
To complete the examination…
Explain to the patient that the examination is now finished.
Thank the patient for their time.
Dispose of PPE appropriately and wash your hands.
Summarise your findings.
Reviewer
Dr Richard Armitage
General Practitioner
References
- Bartels RHMA. A new dimension in degenerative cervical myelopathy. The Lancet Neurology. 2021;20(2):82-83.
- Baptiste DC, Fehlings MG. Pathophysiology of cervical myelopathy. The Spine Journal. 2006;6(6):S190-S197.
- Marc Christopher Emos, Sanjeev Agarwal. Neuroanatomy, Upper Motor Neuron Lesion. Nih.gov. Published December 28, 2018. Available from: [LINK]
- Annaswamy TM, Sakai T, Goetz LL, Pacheco FM, Ozarkar T. Reliability and Repeatability of the Hoffmann Sign. PM&R. 2012;4(7):498-503.
- Zhang AS, Myers C, McDonald CL, Alsoof D, Anderson G, Daniels AH. Cervical Myelopathy: Diagnosis, Contemporary Treatment, and Outcomes. The American Journal of Medicine. 2022;135(4):435-443.
Image references
- Figure 1. StatPearls Publishing LLC and Rian Kabir, MD. Diagram depicting a positive Hoffmann sign. License: [CC BY-NC-ND]
