

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Breech presentation is a type of malpresentation and occurs when the fetal head lies over the uterine fundus and fetal buttocks or feet present over the maternal pelvis (instead of cephalic/head presentation).
The incidence in the United Kingdom of breech presentation is 3-4% of all fetuses.1
Aetiology
Breech presentation is most commonly idiopathic.
Types of breech presentation
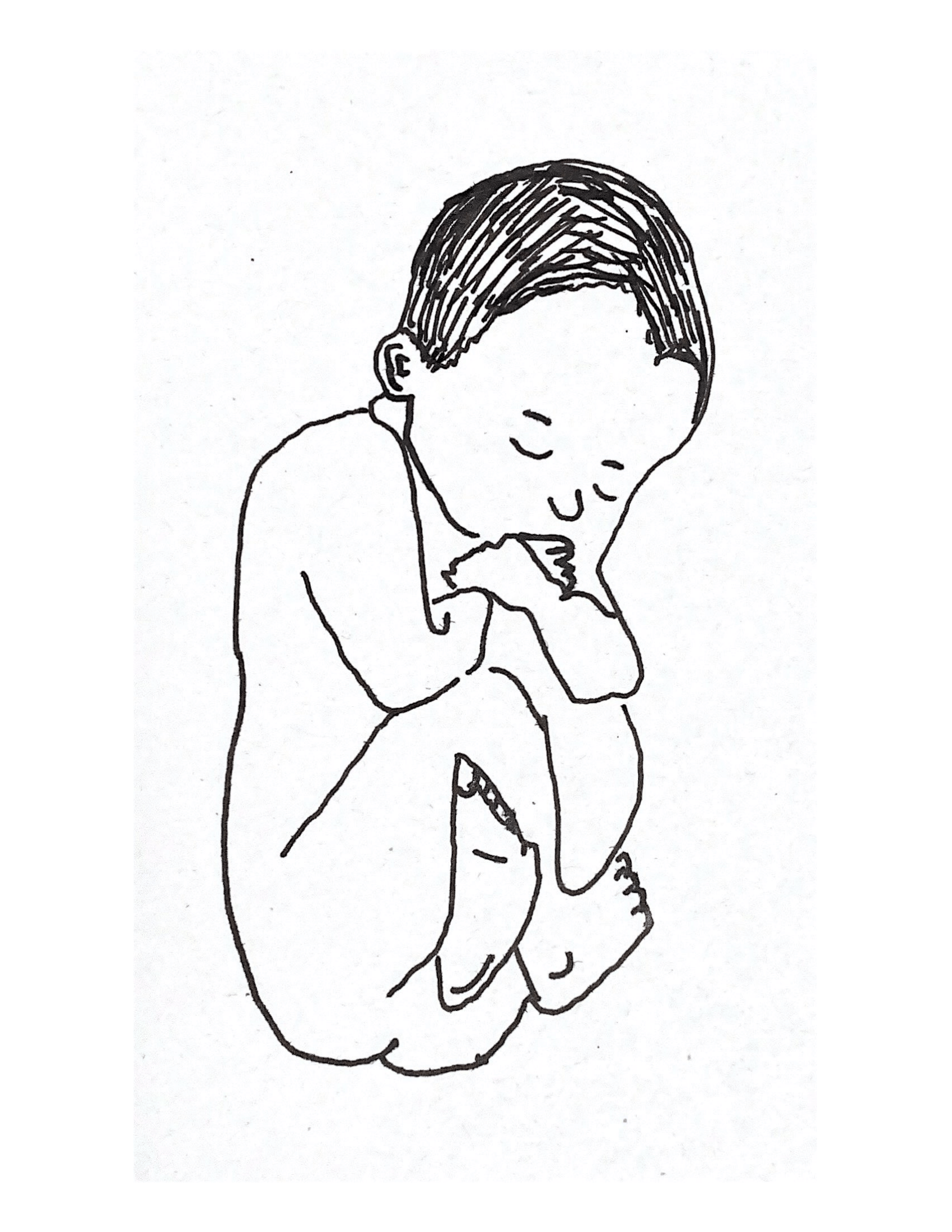
The three types of breech presentation are:
- Complete (flexed) breech: one or both knees are flexed (Figure 1)
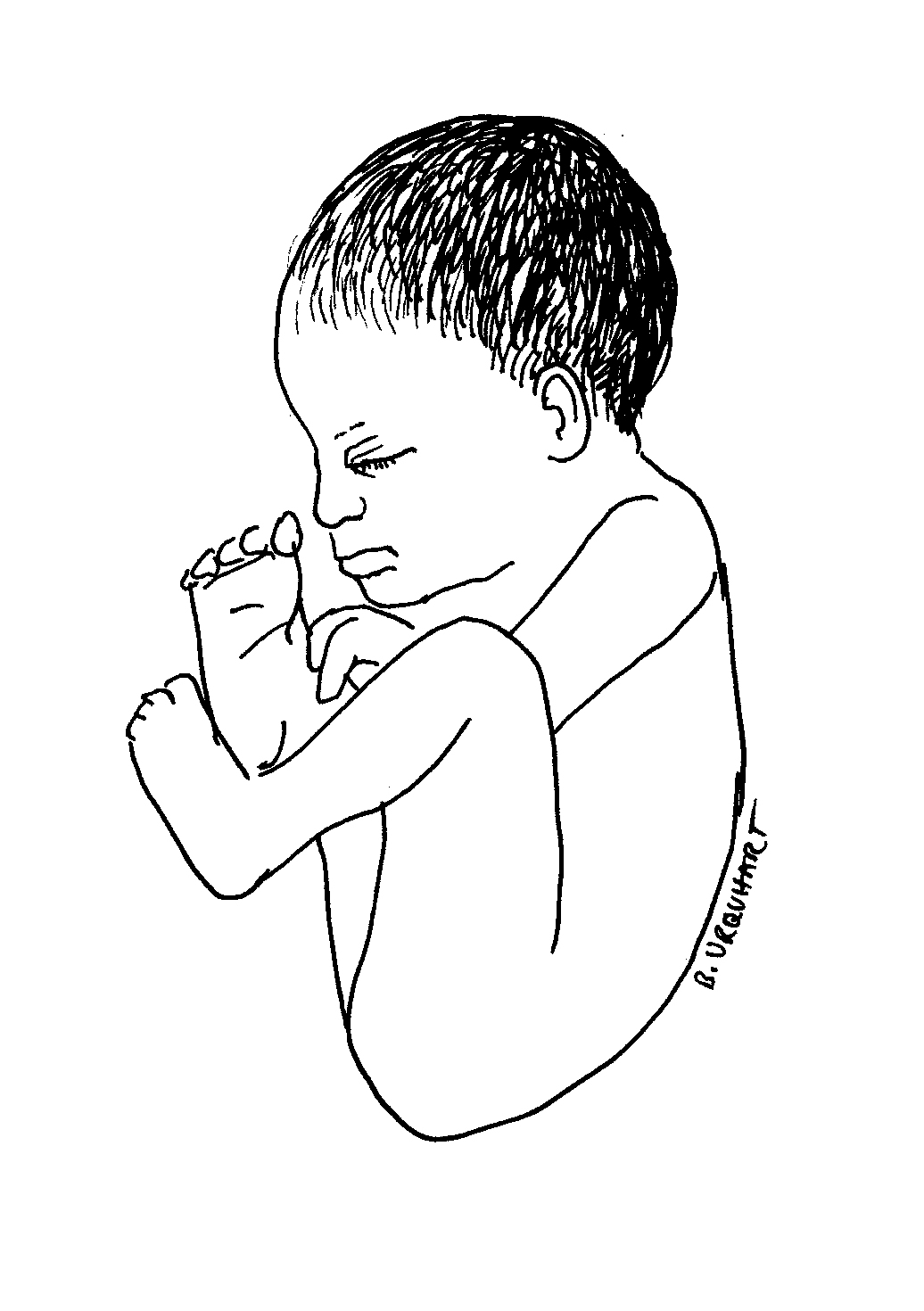
- Footling (incomplete) breech: one or both feet present below the fetal buttocks, with hips and knees extended (Figure 2)
- Frank (extended) breech: both hips flexed and both knees extended. Babies born in frank breech are more likely to have developmental dysplasia of the hip (Figure 3)

Risk factors
Risk factors for breech presentation can be divided into maternal, fetal and placental risk factors:
- Maternal: multiparity, fibroids, previous breech presentation, Mullerian duct abnormalities
- Fetal: preterm, macrosomia, fetal abnormalities (anencephaly, hydrocephalus, cystic hygroma), multiple pregnancy
- Placental: placenta praevia, polyhydramnios, oligohydramnios, amniotic bands
Clinical features
Before 36 weeks, breech presentation is not significant, as the fetus is likely to revert to a cephalic presentation. The mother will often be asymptomatic with the diagnosis being incidental.
The incidence of breech presentation is approximately 20% at 28 weeks gestation, 16% at 32 weeks gestation and 3-4% at term. Therefore, breech presentation is more common in preterm labour. Most fetuses with breech presentation in the early third trimester will turn spontaneously and be cephalic at term.
However, spontaneous version rates for nulliparous women with breech presentation at 36 weeks of gestation are less than 10%.
Clinical examination
Typical clinical findings of a breech presentation include:
- Longitudinal lie
- Head palpated at the fundus
- Irregular mass over pelvis (feet, legs and buttocks)
- Fetal heart auscultated higher on the maternal abdomen
- Palpation of feet or sacrum at the cervical os during vaginal examination
For more information, see the Geeky Medics guide to obstetric abdominal examination.
Positions in breech presentation
There are multiple fetal positions in breech presentation which are described according to the relation of the fetal sacrum to the maternal pelvis.
These are: direct sacroanterior, left sacroanterior, right sacroanterior, direct sacroposterior, right sacroposterior, left sacroposterior, left sacrotransverse and right sacrotranverse.5
Investigations
An ultrasound scan is diagnostic for breech presentation. Growth, amniotic fluid volume and anatomy should be assessed to check for abnormalities.
Management
There are three management options for breech presentation at term, with consideration of maternal choice: external cephalic version, vaginal delivery and Caesarean section.
External cephalic version
External cephalic version (ECV) involves manual rotation of the fetus into a cephalic presentation by applying pressure to the maternal abdomen under ultrasound guidance. Entonox and subcutaneous terbutaline are used to relax the uterus.
ECV has a 40% success rate in primiparous women and 60% in multiparous women. It should be offered to nulliparous women at 36 weeks and multiparous women at 37 weeks gestation.
If ECV is unsuccessful, then delivery options include elective caesarean section or vaginal delivery.
Contraindications for undertaking external cephalic version include:
- Antepartum haemorrhage
- Ruptured membranes
- Previous caesarean section
- Major uterine abnormality
- Multiple pregnancy
- Abnormal cardiotocography (CTG)
Vaginal delivery
Vaginal delivery is an option but carries risks including head entrapment, birth asphyxia, intracranial haemorrhage, perinatal mortality, cord prolapse and fetal and/or maternal trauma.
The preference is to deliver the baby without traction and with an anterior sacrum during delivery to decrease the risk of fetal head entrapment.
The mother may be offered an epidural, as vaginal breech delivery can be very painful.6
Contraindications for vaginal delivery in a breech presentation include:
- Footling breech: the baby’s head and trunk are more likely to be trapped if the feet pass through the dilated cervix too soon
- Macrosomia: usually defined as larger than 3800g
- Growth restricted baby: usually defined as smaller than 2000g
- Other complications of vaginal birth: for example, placenta praevia and fetal compromise
- Lack of clinical staff trained in vaginal breech delivery
- Previous caesarean section
Caesarean section
A caesarian section booked as an elective procedure at term is the most common management for breech presentation.
Caesarean section is preferred for preterm babies (due to an increased head to abdominal circumference ratio in preterm babies) and is used if the external cephalic version is unsuccessful or as a maternal preference. This option has fewer risks than a vaginal delivery.
Complications
Fetal complications of breech presentation include:
- Developmental dysplasia of the hip (DDH)
- Cord prolapse
- Fetal head entrapment
- Birth asphyxia
- Intracranial haemorrhage
- Perinatal mortality
Complications of external cephalic version include:
- Transient fetal heart abnormalities (common)
- Fetomaternal haemorrhage
- Placental abruption (rare)
Key points
- There are three types of breech presentation: complete, incomplete and frank breech
- The most common clinical findings include: longitudinal lie, smooth fetal head-shape at the fundus, irregular masses over the pelvis and abnormal placement being required for fetal hear auscultation
- The diagnostic investigation is an ultrasound scan
- Breech presentation can be managed in three ways: external cephalic version, vaginal delivery or elective caesarean section
- Complications are more common in vaginal delivery, such as cord prolapse, fetal head entrapment, intracranial haemorrhage and birth asphyxia
Reviewer
Miss Saba Al Juboori
Consultant in Obstetrics and Gynaecology
Miss Neeraja Kuruba
Consultant in Obstetrics and Gynaecology
Editor
Dr Chris Jefferies
References
- Oxford Handbook of Obstetrics and Gynaecology. Breech Presentation: Overview. Published in 2011.
- Jemimah Thomas. Image: Complete breech.
- Bonnie Urquhart Gruenberg. Footling breech. Licence: [CC BY-SA]
- Bonnie Urquhart Gruenberg. Frank breech. Licence: [CC BY-SA]
- A Comprehensive Textbook of Obstetrics and Gynaecology. Chapter 50: Malpresentation and Malposition: Breech Presentation. Published in 2011.
- Diana Hamilton Fairley. Lecture Notes: Obstetrics and Gynaecology, Malpresentation, Breech Presentation. Published in 2009.
