

- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
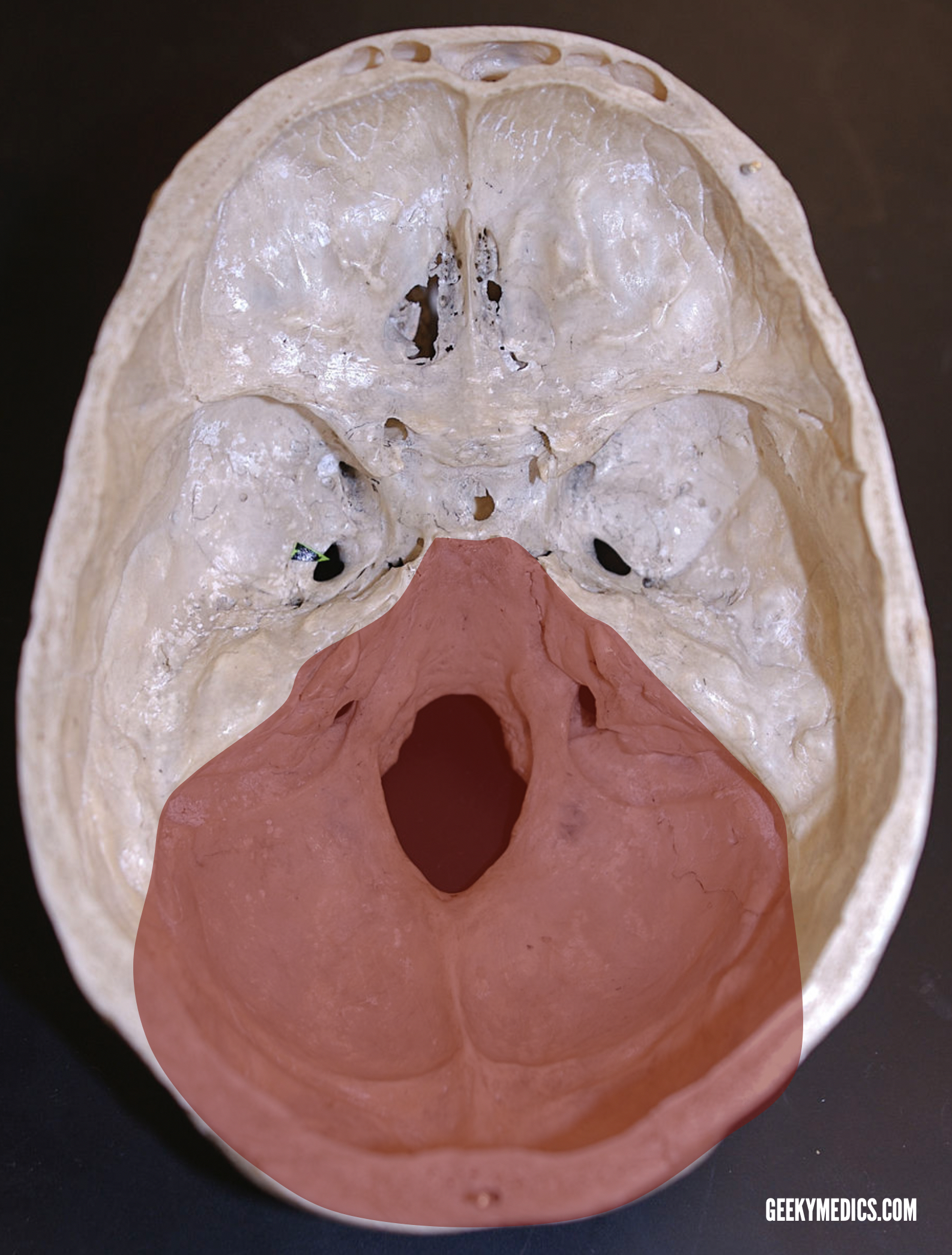
The human skull has numerous openings (foramina), that enable cranial nerves and blood vessels to exit the skull and supply various structures. These openings are collectively referred to as the cranial foramina.
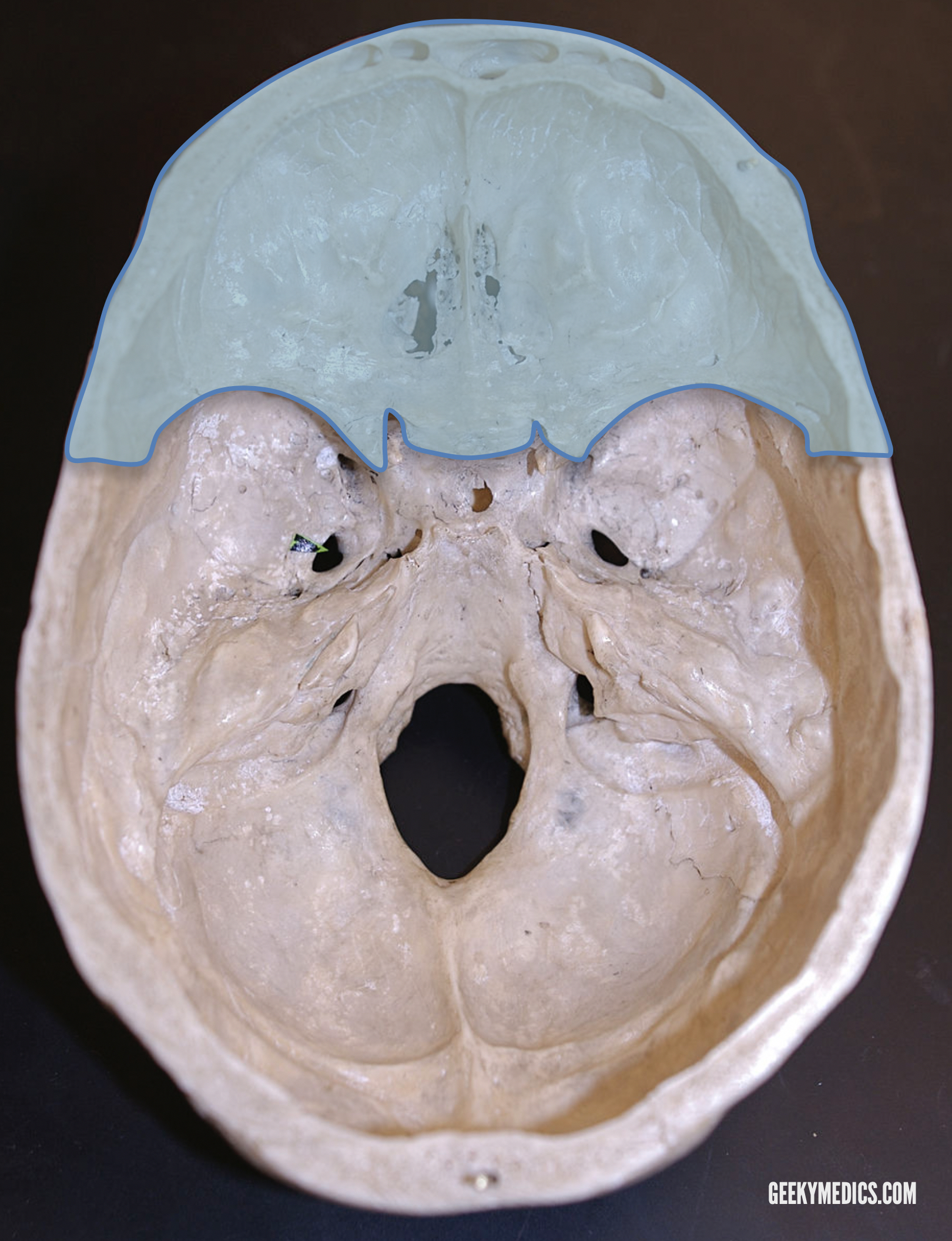
The cranial cavity floor is divided into three distinct recesses: the anterior fossa, middle fossa and, posterior fossa. Each fossa contains specific foramina, through which various anatomical structurespass through.
This article discusses each of the aforementioned fossae and their associated foramina. For more information on the bones of the skull, see the Geeky Medics article here.
Anterior fossa
The anterior fossa is the most shallow of the three recesses and surrounds the anteroinferior aspects of the frontal lobes of the cerebrum. Inferior to the anterior fossa lie the nasal cavities, and the orbits. The anterior fossa is comprised of three bones:
- Frontal
- Ethmoid
- Sphenoid (lesser wings)
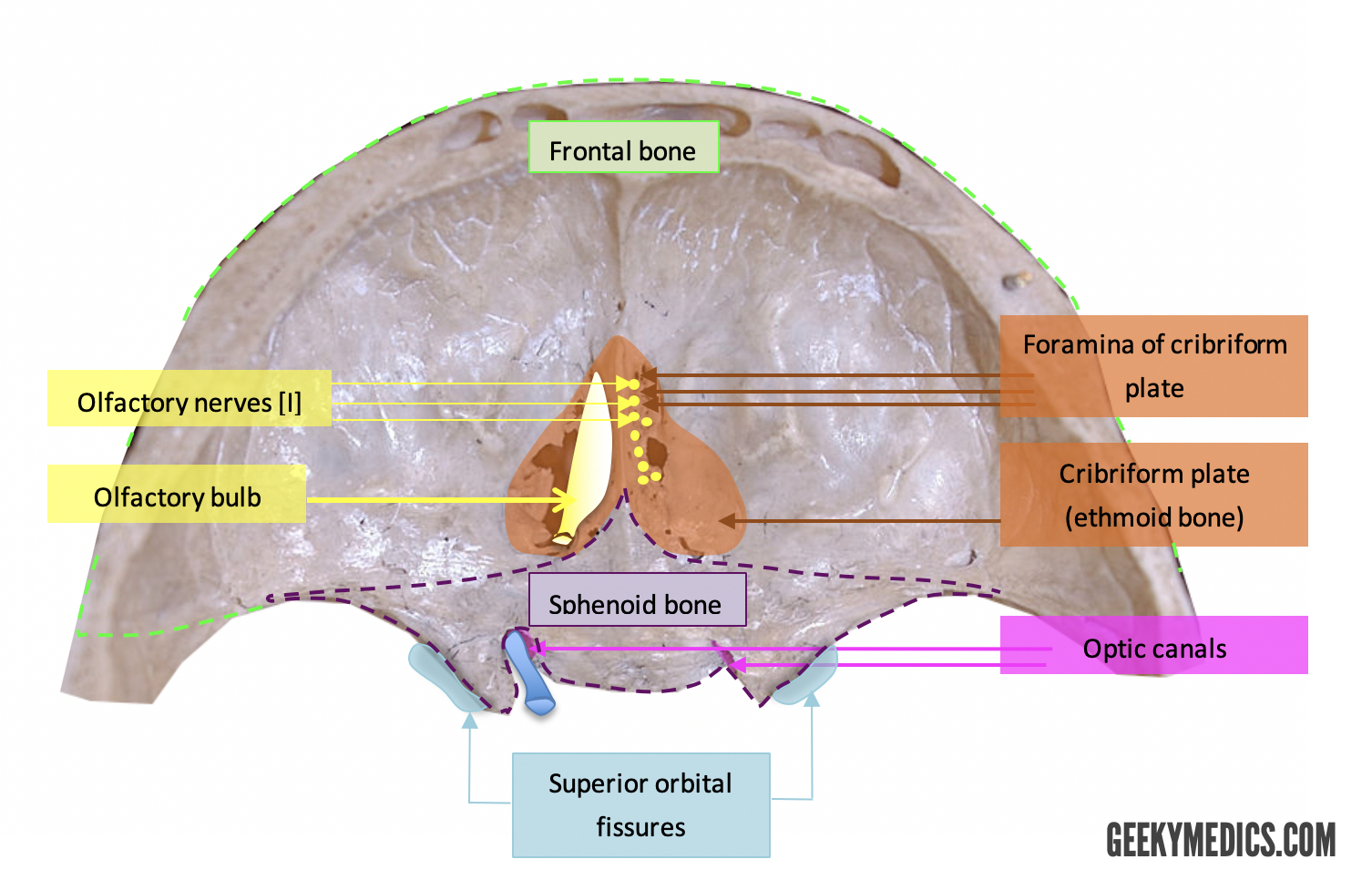
Anterior fossa: foramina
Cribriform plate
This forms part of the ethmoid bone and contains multiple foramina allowing the passage of olfactory nerves from the nasal cavity into the olfactory bulb and then on to the olfactory areas (entorhinal cortex and piriform cortex, among others) within the cerebrum via the olfactory tract.
Clinical relevance: Cribriform plate fracture
Trauma resulting in fracture of the cribriform plate can very commonly result in cerebrospinal fluid (CSF) rhinorrhoea.1 Applying the sample to filter paper, if mixed with blood, can identify CSF leakage. The CSF moves away on the paper, whereas the blood moves closer inwards, resulting in two rings on the paper (target or halo sign).
This leakage of CSF can, in rare cases, put such patients at risk of serious complications including meningitis, encephalitis or brain abscess. Fracture of the cribriform plate can also result in anosmia due to the shearing of the olfactory nerves running through the perforations within the plate.
Superior orbital fissure: between anterior and middle fossae
Bounded superiorly by the lesser wing of sphenoid, and inferiorly by the greater wing of sphenoid, the superior orbital fissure allows transmission from the cavernous sinus into the orbit, of:
- Lacrimal nerve [branch of V1]
- Frontal nerve [branch of V1]
- Trochlear nerve [IV]
- Superior division of oculomotor nerve [III]
- Nasociliary nerve [branch of V1]
- Inferior division of oculomotor nerve [III]
- Abducens nerve [VI]
The above are listed in order going from superior to inferior as they pass through the fissure. It can be appreciated that this includes nerves supplying motor innervation to the eyes.
Middle cranial fossa
The middle cranial fossa comprises three bones:
- Sphenoid
- Two temporal bones
The temporal bones surround the temporal lobes laterally within the middle fossa, and the sphenoid bone sits more centrally. The sphenoid bone contains a deep depression known as the sella turcica (‘Turkish saddle’ – Latin etymological origin). This is a centrally located deep depression within the sphenoid bone. The most inferior part of the sella turcica, the hypophyseal fossa, contains the pituitary gland.

Middle fossa: foramina
Sphenoid bone
Optic canal
This transmits to the orbit, the:
- Optic nerve [II]
- Ophthalmic artery
Foramen rotundum
Transmits maxillary division of the trigeminal nerve [V2].
Foramen ovale
Transmits mandibular division of the trigeminal nerve [V3].
Foramen lacerum
This is filled with cartilage and lies at the intersection between temporal, sphenoid and occipital bones.
Foramen spinosum
This foramen transmits the middle meningeal artery (as well as the middle meningeal vein), and a branch of the mandibular division of the trigeminal nerve [V].
Temporal bone
Carotid canal
The internal carotid artery runs through the carotid canal before continuing to form the middle cerebral artery and running across the circle of Willis to supply blood to the brain.

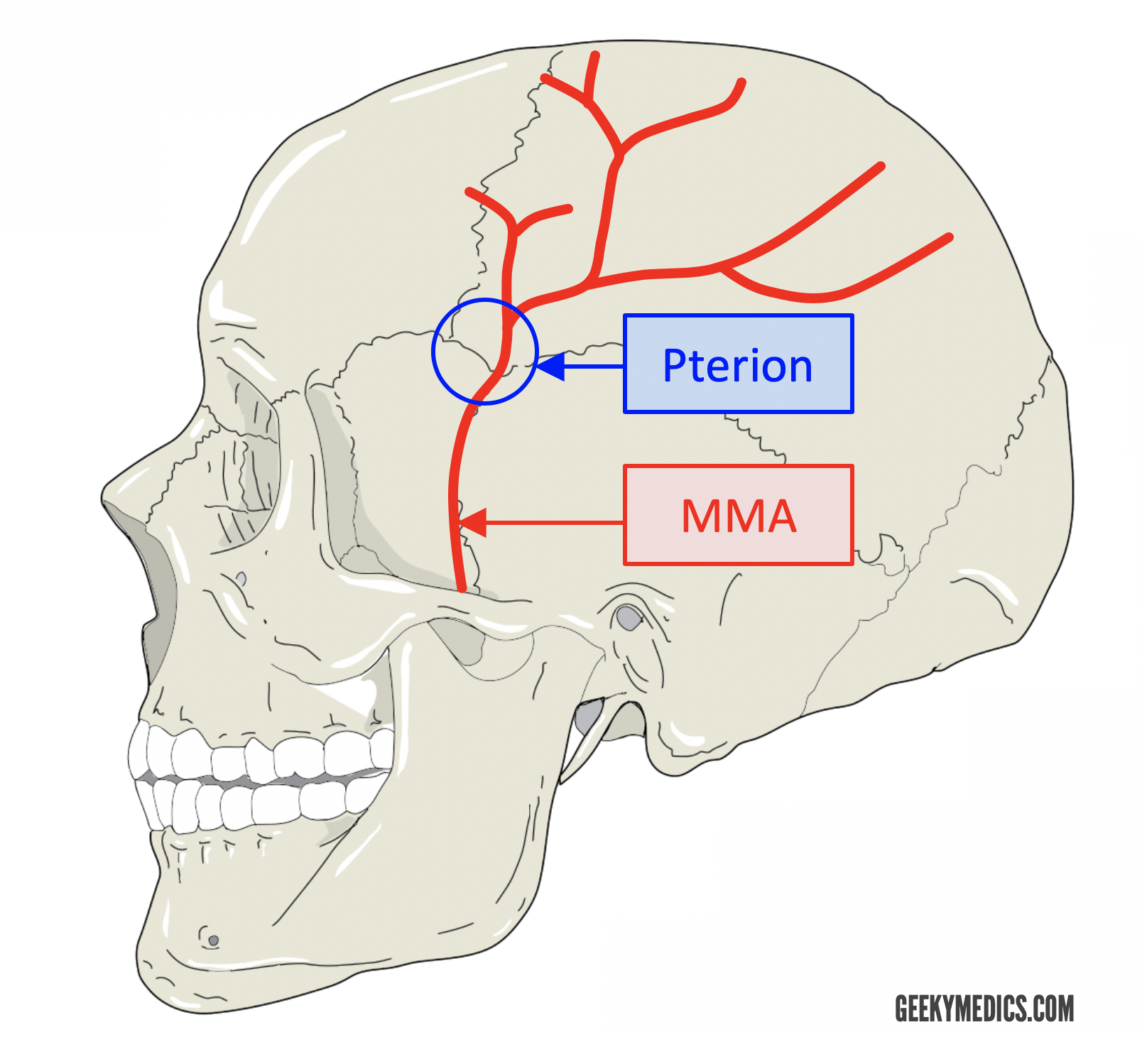
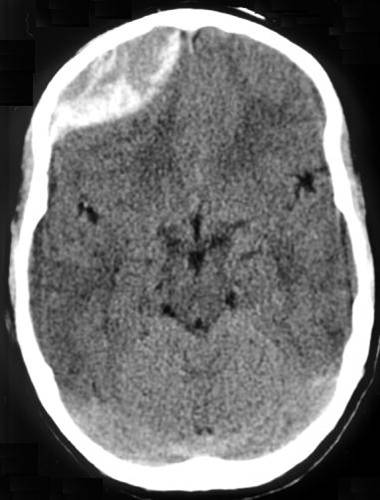
Clinical relevance: middle meningeal artery
The middle meningeal artery, a branch of the maxillary artery, enters the middle cranial fossa via the foramen spinosum. It ultimately splits into anterior and posterior divisions. It is the anterior division that runs anterolaterally along the greater sphenoid wing until it eventually passes under the pterion and giving off its terminal branches. The pterion is the site of a junction between four bones, and is the weakest point in the skull:
- Frontal
- Parietal
- Greater sphenoid
- Temporal bone (squamous)
A fracture in this region can result in damage to the middle meningeal artery and subsequent extradural haemorrhage. The pterion is also a common neurosurgical approach to access the middle cranial fossa for a range of procedures.
Posterior fossa
The posterior fossa or the cranial cavity is the deepest of the three recesses that comprise the three cranial fossae. This fossa surrounds the cerebellum and the brainstem, and is made up of three bones:
- Two temporal bones
- Occipital
Posterior fossa foramina
Temporal bone
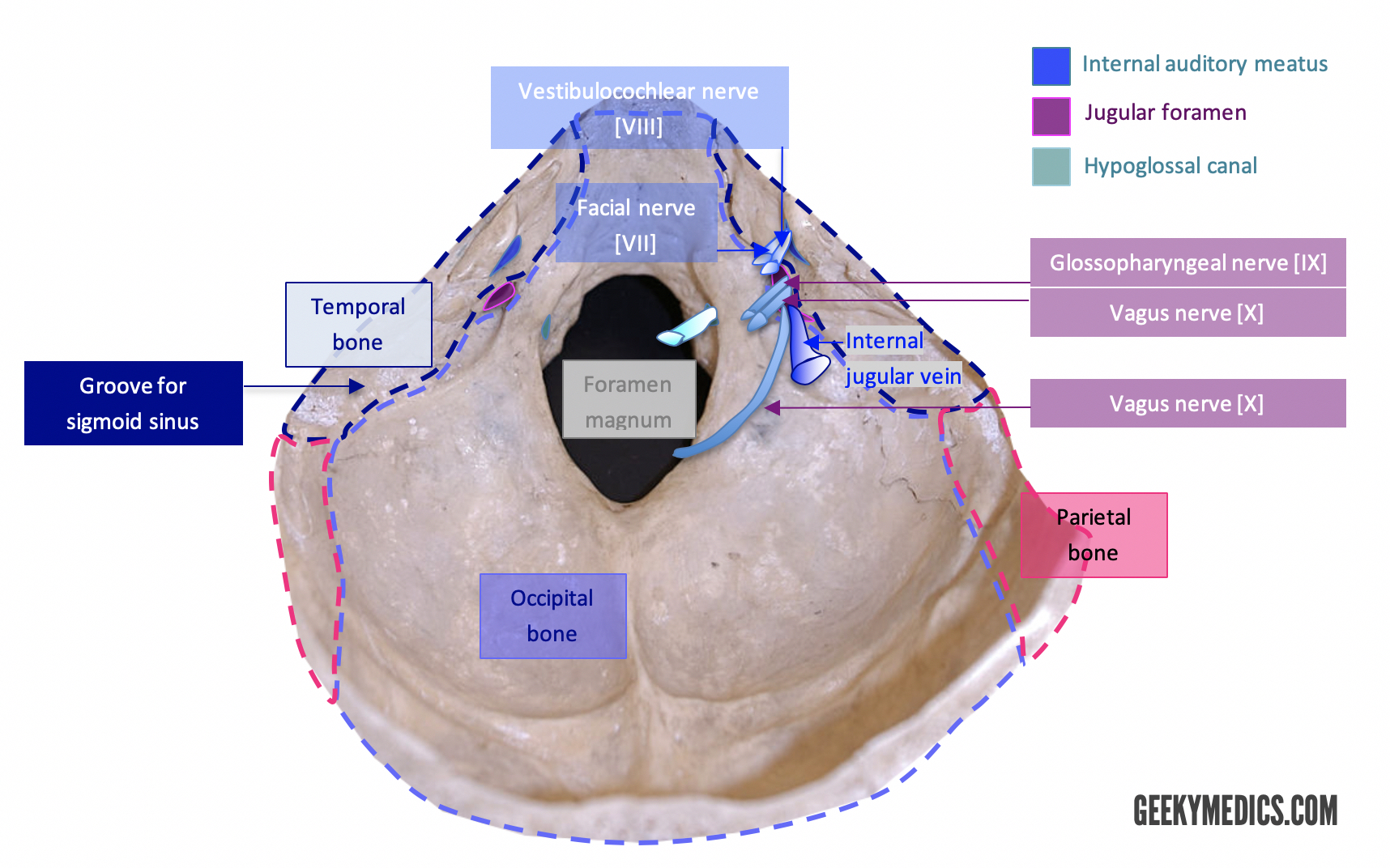
Internal acoustic meatus
This opening lies within the posterior component of the petrous portion of the temporal bone and comprises the start of a bony canal linking the posterior fossa to the inner ear. Two cranial nerves pass through the internal acoustic meatus:
- Facial nerve [VII]
- Vestibulocochlear nerve [VIII]
The labyrinthine artery also traverses the internal acoustic meatus.
Occipital bone
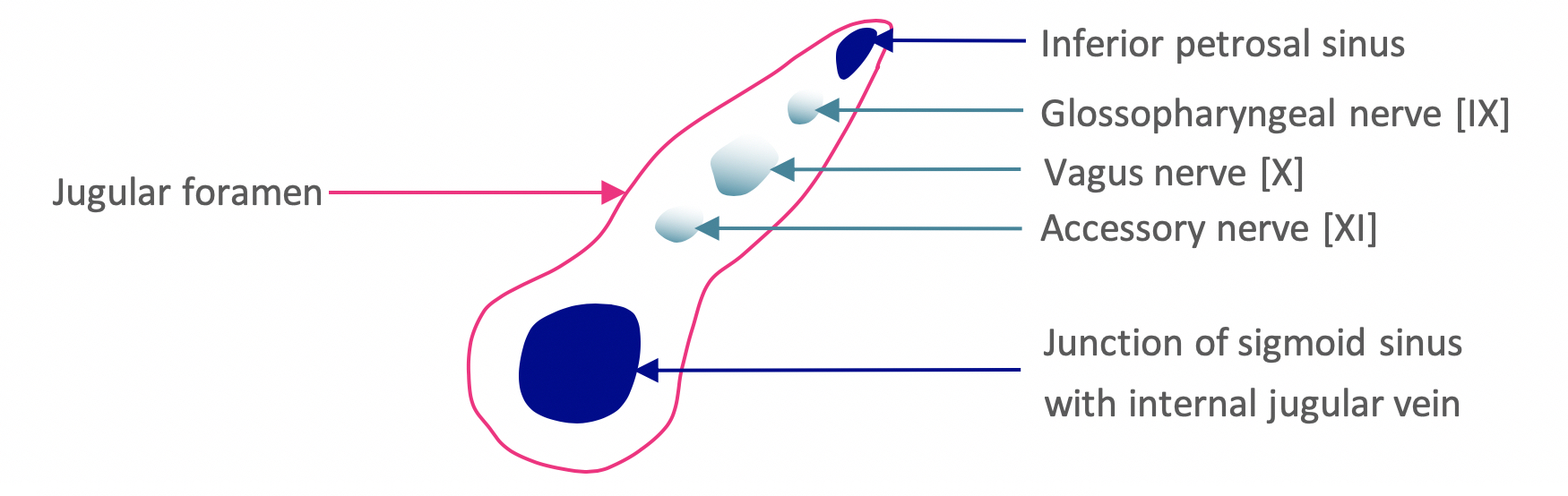
Jugular foramen
This foramen is superiorly bordered by the petrous portion of the temporal bone, and inferiorly by the occipital bone. Three cranial nerves are communicated by the jugular foramen:
- Glossopharyngeal nerve [IX]
- Vagus nerve [X]
- Descending spinal accessory nerve [XI]
The jugular foramen is often divided into three sections – the above cranial nerves pass through the middle compartment.
Furthermore, components of the cerebral drainage system pass through this foramen:
- Inferior petrosal sinus (anteriorly within the foramen)
- Sigmoid sinus (posteriorly within the foramen)
Hypoglossal canal
This canal transmits the hypoglossal nerve [XII].
Foramen magnum
This is a large opening within the floor of the cranial cavity. The largest foramen within the skull conveys significant structures such as:
- Medulla
- Vertebral arteries
- Anterior/posterior spinal arteries
This foramen also transmits the ascending spinal accessory nerve [XI] and dural veins.
Clinical relevance: Chiari malformation
German pathologist Hans Chiari described a number of brainstem and inferior cerebellar irregularities.
Chiari type I malformations commonly arise from calvarial abnormalities and result in the displacement of the cerebellar tonsils through the foramen magnum.
Chiari type II malformations are characterised by displacement of the medulla, fourth ventricle, as well as the cerebellum, through the foramen magnum. Chiari type II malformations are usually due to a small posterior fossa and are almost always associated with myelomeningocoele.3
Both types I and II malformations result in varying degrees of herniation (displacement of the aforementioned structures into the upper cervical spinal cord). Types III and IV are much rarer and, as such, are not well-described. Some common symptoms due to compression of the brainstem include:
- Sub-occipital headaches: type I
- Dizziness, hearing loss, and nystagmus
- Gradual loss of function
- Spastic quadriparesis (plus upper motor neurone features): type II
Treatment is guided by the anatomical irregularity. For example, surgical decompression via sub-occipital craniectomy and C1 laminectomy is used to achieve foramen magnum decompression.
You can purchase a licence for the Complete Anatomy software we use in our videos here (we also get a percentage of your purchase fee if you use this link).
References
- Abuabara A. (2007) Cerebrospinal fluid rhinorrhoea: diagnosis and management. Med Oral Patol Oral Cir Bucal. 12: E397–E400
- Silver, M. J., McAllister, T. W., Yudofsky S. C. (2011) Textbook of Traumatic Brain Injury. 2nd American Psychiatric Publishing Incorporated.
Figures
- Matthew S. Cain (2008), A photograph of the lower inner surface of a human skull. License: [Public domain] (modified by Melissa Gough, 2019)
- Matthew S. Cain (2008), A photograph of the lower inner surface of a human skull. License: [Public domain] (modified by Melissa Gough, 2019)
- Matthew S. Cain (2008), A photograph of the lower inner surface of a human skull. License: [Public domain] (modified by Melissa Gough, 2019)
- Matthew S. Cain (2008), A photograph of the lower inner surface of a human skull. License: [Public domain] (modified by Melissa Gough, 2019)
- GDJ (2016), Realistic human skull profile view. License: [Public domain] (modified by Melissa Gough, 2019)
- Jpogi (2012), Non-contrast CT scan of an acute epidural haematoma. License: [Public domain] (modified by Melissa Gough, 2019)
- Matthew S. Cain (2008), A photograph of the lower inner surface of a human skull. License: [Public domain] (modified by Melissa Gough, 2019)
- Jugular foramen compartments (Melissa Gough, 2019)
- Matthew S. Cain (2008), A photograph of the lower inner surface of a human skull. License: [Public domain] (modified by Melissa Gough, 2019)
