
- 📖 Geeky Medics OSCE Book
- ⚡ Geeky Medics Bundles
- ✨ 1300+ OSCE Stations
- ✅ OSCE Checklist PDF Booklet
- 🧠 UKMLA AKT Question Bank
- 💊 PSA Question Bank
- 💉 Clinical Skills App
- 🗂️ Flashcard Collections | OSCE, Medicine, Surgery, Anatomy
- 💬 SCA Cases for MRCGP
To be the first to know about our latest videos subscribe to our YouTube channel 🙌
Introduction
Pneumonia is defined as an acute infection of the lung parenchyma caused by various pathogens. It is a term that includes several clinical syndromes caused by various organisms or pathological insults.1
The annual incidence of community-acquired pneumonia in the UK is estimated at 5-10 per thousand adults. The proportion of UK adults requiring hospitalisation due to community-acquired pneumonia is between 22-42%, with a mortality rate of 5-14%.2
This article will focus on the aetiology, risk factors, clinical features, diagnosis and management of pneumonia, including the CURB-65 score.
Aetiology
Pneumonia can be classified according to infective agent, clinical setting, method of transmission and radiographic appearance. This article will focus on the most commonly used classifications.
Community-acquired pneumonia
Community-acquired pneumonia (CAP) is defined as symptoms and signs consistent with an acute lower respiratory tract infection associated with new radiographic shadowing for which there is no other explanation, occurring outside of the hospital or healthcare setting.3
CAP is then generally subclassified according to the infective agent.
Bacterial
Bacterial cases of pneumonia have traditionally been divided into ‘typical’ and ‘atypical’ pneumonia, with the term now outdating its historical usefulness.
Atypical pathogens are often challenging to diagnose early in the illness as they may not be detectable on gram stain or cannot be cultured using standard methods. They are also usually sensitive to antibiotics other than β-lactams.3,4
Typical
Typical bacterial pneumonia is caused by the most common organisms associated with pneumonia. Streptococcus pneumoniae is the leading bacterial cause of CAP across a range of age groups.5
Other bacterial causes include Haemophilus influenzae, Staphylococcus aureus (including MRSA), and Moraxella catarrhalis.6 However, mixed pathogens are not uncommon.
Atypical
Atypical bacterial pneumonia is caused by less common organisms that may be more challenging to diagnose or may be associated with specific patient populations. The most commonly reported atypical bacteria are Mycoplasma pneumoniae, Chlamydophila pneumoniae, and Legionella pneumophila.4
Specific patient populations
Exam questions typically test the aetiology in specific population groups.
Table 1. Common causative organisms in specific patient populations.7
| Patient group/condition | Pathogen(s) |
| Chronic obstructive pulmonary disease (COPD) | Haemophilus influenzae, Pseudomonas aeruginosa |
| Alcoholism | Klebsiella pneumoniae, Streptococcus pneumoniae |
| Post-influenza infection | Staphylococcus aureus, Streptococcus pneumoniae |
| Exposure to birds | Chlamydophila pneumoniae |
| Hotel or cruise ship stay in the previous two weeks | Legionella pneumophila |
| Intravenous drug use | Staphylococcus aureus |
Viral
Viral respiratory tract infections can lead to primary viral pneumonia and predispose to secondary bacterial pneumonia. The most common viruses detected in cases of CAP are influenza A and B.8
Other causes are severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), rhinoviruses, parainfluenza viruses, adenoviruses, respiratory syncytial virus and other coronaviruses (e.g., Middle East respiratory syndrome CoV).8
Fungi
Fungal pneumonia is rare and primarily seen in immunocompromised patients and endemic areas. These include Cryptococcus neoformans, candida species, Aspergillus species, Histoplasma capsulatum and Pneumocystis jirovecii.9
Hospital-acquired pneumonia
There is considerable overlap between community and hospital-acquired pneumonia (HAP). However, HAP is defined as a lower respiratory tract infection acquired after 48 hours of hospital admission, which was not incubating at the time of admission.10
The causative organisms in HAP are typically more prevalent in the hospital environment and have increased rates of antimicrobial resistance. These usually include gram-negative bacilli (Pseudomonas aeruginosa, Escherichia coli, Klebsiella pneumonia) and gram-positive cocci (Streptococcus pneumoniae, Staphylococcus aureus (including MRSA)).11
S. pneumoniae is the most prominent bacteria in infections occurring within the first five days of admission.11
Ventilator-associated pneumonia
This represents a sub-set of hospital-acquired pneumonia, typically occurring in the critical care setting. Ventilator-associated pneumonia is defined as occurring 48 – 72 hours after tracheal intubation. The causative organisms are similar to those of HAP.11
Aspiration pneumonia
Aspiration pneumonia results from inhaling oropharyngeal contents, which can predispose to bacterial infection, chemical pneumonitis (secondary to acidic gastric secretions) and lung injury.
This is more common in those with swallowing dysfunction (e.g. after a stroke), undergoing general anaesthesia, delayed gastric emptying (e.g. obesity, pregnancy), and those with a poor cough (e.g. neuromuscular disorders, nerve palsies).
Microbiological aetiology varies depending on the source of the aspirate and individual factors. However, recent studies have shown that bacteriology remains similar to non-aspiration pneumonia.12
Risk factors
Risk factors for pneumonia include:6,13
- Age: particularly infants/young children and those >65 years old
- Smoking: particularly pneumococcal pneumonia
- Alcohol use: there is a strong correlation between increased alcohol use and pneumonia
- Pre-existing respiratory conditions: COPD, asthma, malignancy, bronchiectasis
- Intravenous drug use: often associated with Staphylococcus aureus
- Hospitalisation or residence in a healthcare setting (e.g. nursing homes)
- Proton-pump inhibitors: thought to be secondary to increased upper airway colonisation due to reduced gastric acid secretion
- Poor oral hygiene: particularly in aspiration pneumonia
- Child contacts: likely due to increased rates of transmission
Clinical features
History
Typical symptoms of pneumonia include:11
- Productive cough: with mucopurulent sputum in bacterial pneumonia
- Dyspnoea: shortness of breath, particularly on exertion
- Pleuritic chest pain: pain exacerbated on deep inspiration
- Fevers and rigors: feeling hot and sweaty with cold chills
- Confusion: typically seen in the older population
- Constitutional features: including lethargy, malaise, myalgia, anorexia, and headache
For more information, see the Geeky Medics guide to respiratory history taking.
Atypical pneumonia may present with a characteristic history and features depending on the organism.
Table 2. Characteristic features of atypical pneumonia.6,13
| Organism | Characteristic features |
|
Mycoplasma pneumoniae
|
|
|
Chlamydophila pneumoniae
|
|
|
Legionella pneumophila
|
|
Clinical examination
A complete respiratory examination is required in all cases of suspected pneumonia.
Typical clinical findings of pneumonia include:6
- Vital signs: tachypnoea, hypoxia, and tachycardia may all be present
- Course crackles and/or decreased breath sounds: on auscultation of the chest
- Dullness to percussion: over the affected area of the chest wall
- Wheeze: particularly in those with associated respiratory conditions, i.e., asthma/COPD
Differential diagnoses
Differential diagnoses to consider in suspected pneumonia include:6
- Upper respiratory tract infection
- Exacerbation of COPD
- Exacerbation of asthma
- Congestive heart failure
- Coronavirus disease 2019
- Tuberculosis
- Lung cancer
- Empyema
- Pulmonary embolism
Investigations
Investigations beyond basic observations are typically unnecessary for most patients in the community setting. For patients admitted to the hospital, all of the following should be considered.6,11,13
Bedside investigations
Relevant bedside investigations include:
- Basic observations: to assess for hypoxia, fever, tachypnoea, tachycardia and hypotension (in septic shock)
- Polymerase chain reaction (PCR) test: this allows for the rapid identification of various organisms, depending on the test, i.e., an extended viral screen including SARS-CoV-2
Laboratory investigations
Relevant laboratory investigations include:
- Full blood count: may demonstrate a raised white cell count.
- C-reactive protein (CRP): elevated in infection and can be used to aid prognosis.
- Urea and electrolytes: urea is part of the CURB-65 severity score, and patients may present with a comorbid acute kidney injury. Hyponatraemia may be seen in Legionella.
- Liver function tests: baseline hepatic function for antibiotic treatment. These may be deranged in Legionella
- Sputum culture: ideally taken before starting antibiotics, with antibiotics optimised based on sensitivities. The sample should be expedited to microbiology to prevent degradation.
- Blood cultures: should be requested in all patients with moderate or high-severity pneumonia. Ideally, cultures should be taken before antibiotics are given. Antibiotics should then be optimised based on sensitivities.
- Arterial blood gas: recommended in hypoxic patients, those at risk of hypercapnia or who are graded as high-risk pneumonia, depending on the patient it may show type 1 or type 2 respiratory failure.
- Legionella and pneumococcal urinary antigen: this should be requested in those with moderate or high-severity CAP or where other risk factors exist.
Imaging
Relevant imaging investigations include:
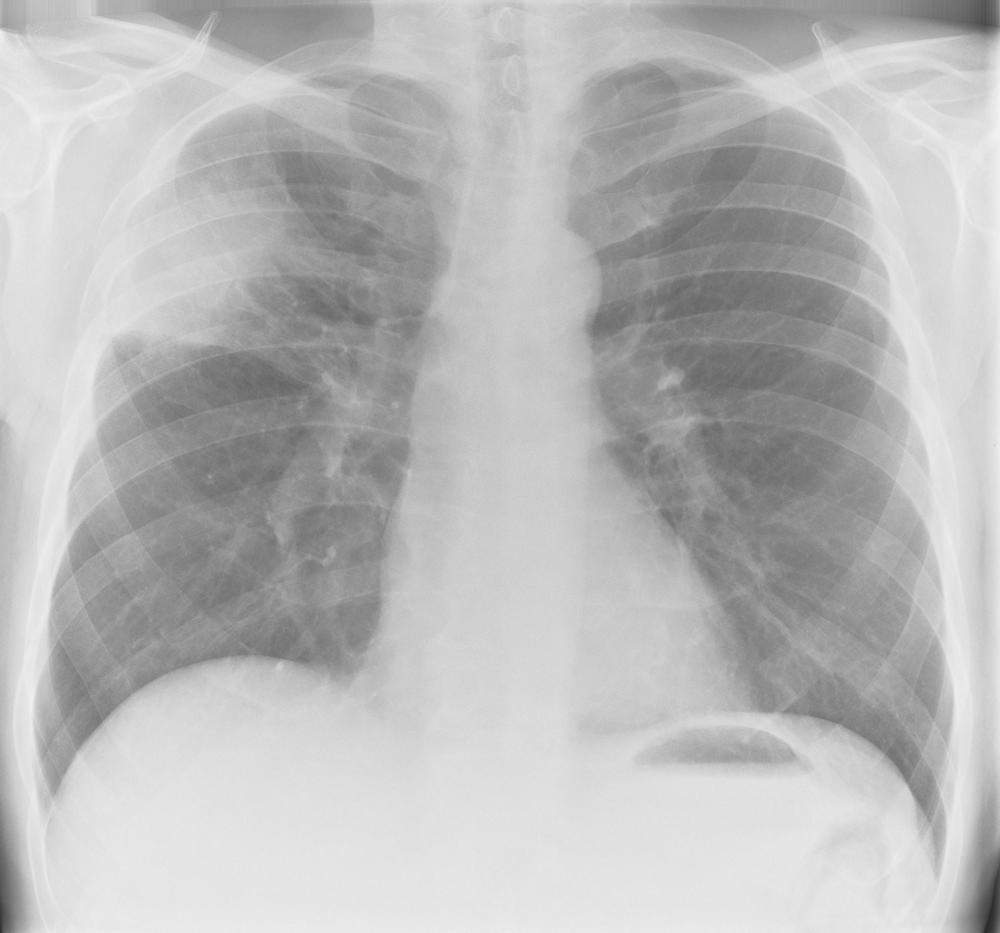
- Chest X-ray: the diagnostic investigation for pneumonia. Evidence of consolidation is seen.
- CT thorax: this is only considered where there is diagnostic doubt or if a chest X-ray suggests abnormalities which require further imaging.
Diagnosis
A diagnosis of pneumonia can be reached with typical features in the history and on clinical examination, alongside radiological evidence on a chest X-ray.
CURB-65
The severity of community-acquired pneumonia can then be calculated using the CURB-65 score.6
- Confusion: new onset, which may be defined as an abbreviated mental test (AMT-10) score ≤8
- Urea: of >7 mmol/L
- Respiratory rate: ≥30 breaths/minute
- Blood pressure: <90 mmHg systolic or ≤60 mmHg diastolic
- Age: ≥65 years
Each criterion scores one point, with the total used to guide hospital admission, treatment, critical care escalation and mortality. However, CURB-65 is an arbitrary scoring system and should complement clinical judgment.
Score 0-1: low risk
- Consider outpatient treatment
Score 2: moderate risk
- Consider inpatient or hospital-supervised outpatient treatment
Score 3-5: high risk
- Admission for inpatient treatment with consideration for discussion with critical care if achieving the higher end of the range
In the community setting, urea may be removed, with CRB-65 utilised instead.
Management
Acute management
The acute management of pneumonia consists of supportive measures, such as rest and oral hydration, alongside medical management, such as antibiotics. Acutely unwell patients should be assessed with an ABCDE approach.
Patients well enough to remain in the community can generally be managed with supportive measures and oral antibiotics.
Those who require hospital admission may require more intense medical management alongside antibiotics:
- Oxygen: to maintain appropriate oxygen saturations.
- Intravenous fluids: rate and volume dependent on the clinical stability and degree of volume depletion. (See the Geeky Medics article on IV fluid prescribing)
- Analgesia and antipyretics: simple analgesia such as paracetamol and non-steroidal anti-inflammatory drugs (providing no contraindications) or a weak opioid (e.g., codeine), if required.
- Venous thromboembolism (VTE) prophylaxis: all hospitalised patients should undergo a VTE risk assessment and receive appropriate prophylaxis.
Antibiotic prescribing
Local guidelines should be followed for antibiotic prescribing due to local resistance and sensitivities. NICE recommends initial antibiotic treatment based on pneumonia severity, typically lasting five days.
All antibiotics should be reviewed at 48-72 hours in conjunction with culture sensitivities, inflammatory markers and the patient’s clinical signs. The antimicrobial of choice, dose and route should be considered. Speak to a senior clinician or microbiologist if you have concerns.
Intravenous antibiotics should be prescribed in patients with clinical features of severe infection or sepsis or where gastrointestinal absorption is not reliable (i.e., vomiting, severe diarrhoea).
Community-acquired pneumonia
These are some antimicrobial options based on NICE guidelines for CAP in adults.14 As mentioned above, always consult local guidelines.
Low severity
First choice oral antibiotic:
- Amoxicillin: 500 mg – 1 g three times a day
Alternative oral antibiotics:
- Doxycycline: 200 mg on day one, then 100 mg a day
- Clarithromycin: 500 mg twice a day
Moderate severity
First choice combination of:
- Amoxicillin: 500 mg – 1 g three times a day
- Clarithromycin: 500 mg twice a day
Alternative oral antibiotics:
- Doxycycline: 200 mg on day one, then 100 mg a day
- Clarithromycin: 500 mg twice a day
- Erythromycin (in pregnancy): 500 mg four times a day
High severity
First choice combination of:
- Co-amoxiclav: 500/125 mg three times a day orally, or 1.2 g three times a day IV
- Clarithromycin: 500 mg twice a day
Hospital-acquired pneumonia
These are some antimicrobial options based on NICE guidelines for HAP in adults.15 As mentioned above, always consult local guidelines.
Non-severe
First choice oral antibiotic:
- Co-amoxiclav: 500/125 mg three times a day orally
Alternative oral antibiotics:
- Co-trimoxazole: 960 mg twice a day
- Doxycycline: 200 mg on day one, then 100 mg a day
Severe
First choice IV antibiotics:
- Piperacillin with tazobactam: 4.5 g three times a day (four times a day if severe infection)
- Meropenem: 0.5 g – 1 g three times a day
- Ceftriaxone: 2 g once a day
Vaccination
There are also vaccinations available to protect against various causes of pneumonia. See the Geeky Medics childhood immunisations article for more information on the childhood vaccine schedule.
Pneumococcal
Two forms of pneumococcal vaccine are currently used in the UK; the pneumococcal polysaccharide vaccine (PPV) and the pneumococcal conjugate vaccine (PCV). Both are inactivated vaccines.16
The pneumococcal conjugate vaccine (PCV) is offered for infants at 12 weeks of age and at one year old. Additional doses are required for those with asplenia, splenic dysfunction, complement disorder, or severe immunocompromise.
The pneumococcal polysaccharide vaccine (PPV) is offered for adults 65 years and older and at different ages for those in clinical risk groups, including:
- Asplenia or splenic dysfunction
- Chronic respiratory disease
- Chronic heart disease
- Chronic kidney disease
- Chronic liver disease
- Diabetes (medication or insulin-dependent)
- Immunosuppression
- Cochlear implants
- Cerebrospinal fluid leak (including trauma)
- Occupational risk
Haemophilus influenzae type b (Hib)
A polysaccharide conjugate vaccine is offered as part of the childhood immunisation schedule at 8, 12 and 16 weeks, and one year. Hib is typically combined with other vaccines.17
Complications
Complications of pneumonia include6,13:
- Septic shock: pneumonia can lead to sepsis, which can rapidly progress to multi-organ failure and shock.
- Acute respiratory distress syndrome (ARDS): consists of non-cardiogenic pulmonary oedema and severe lung inflammation.
- Pleural effusion: associated with increased pneumonia severity and risk of treatment failure.
- Empyema: a collection of pus within the pleural space.
- Lung abscesses: rare but more commonly seen in Klebsiella or Staphylococcal pneumonia.
- Post-infective bronchiectasis: permanent dilation and thickening of the airways.
Key points
- Pneumonia is defined as an acute infection of the lung parenchyma with radiological evidence of consolidation.
- Pneumonia can be characterised based on pathogen aetiology and the pathogenesis of the infection.
- CURB-65 can be used to risk stratify community-acquired pneumonia and guide management.
- Sputum cultures should always be obtained in hospitalised patients.
- Broad-spectrum antibiotics should be started initially and reviewed with culture sensitivities, inflammatory markers and clinical features.
- Pneumonia can progress to septic shock and multi-organ failure, and early antibiotic prescribing can prevent this.
Reviewer
Dr Ahmed Abou-Haggar
Respiratory Consultant
Editor
Dr Jess Speller
References
- Mackenzie G. The definition and classification of pneumonia. Pneumonia. 2016;8(1). doi:10.1186/s41479-016-0012-z
- NICE. Pneumonia in adults: diagnosis and management. Published online 2014. Available from: [LINK]
- Lim WS, Baudouin SV, George RC, et al. BTS guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009;64(Suppl 3):iii1-iii55.
- BMJ Best Practice. Atypical pneumonia (non-COVID-19). Published 2021. Available from: [LINK]
- Chapman SJ, Robinson GV, Shrimanker R, Turnbull CD, Wrightson JM. Respiratory infection—bacterial. In: Chapman SJ, Robinson GV, Shrimanker R, Turnbull CD, Wrightson JM, eds. Oxford Handbook of Respiratory Medicine. Oxford University Press; 2021:517-558.
- BMJ Best Practice. Community-acquired pneumonia (non-COVID-19). Published 2023. Available from: [LINK]
- File TM. Community-Acquired Pneumonia, Bacterial. In: Netter’s Infectious Diseases. Elsevier; 2012:127-136.
- Ramirez J. Overview of community-acquired pneumonia in adults. UpToDate. Published 2023. Available from: [LINK]
- Li Z, Lu G, Meng G. Pathogenic Fungal Infection in the Lung. Front Immunol. 2019;10:1524.
- BMJ Best Practice. Hospital-acquired pneumonia (non-COVID-19). Published 2023. Available from: [LINK]
- Shebl E, Gulick PG. Nosocomial Pneumonia. In: StatPearls. StatPearls Publishing; 2023. Available from: [LINK]
- BMJ Best Practice. Aspiration pneumonia. Published 2023. Available from: [LINK]
- Knott L. Pneumonia. Patient.info. Published 2020. Available from: [LINK]
- NICE. Pneumonia (community-acquired): antimicrobial prescribing. Published online 2019. Available from: [LINK]
- NICE. Pneumonia (hospital-acquired): antimicrobial prescribing. Published online 2019. Available from: [LINK]
- Public Health England. Chapter 25: Pneumococcal. In: Immunisation against Infectious Disease. ; 2023.
- Public Health England. Chapter 16: Haemophilus influenzae type b (Hib). In: Immunisation against Infectious Disease. ; 2013.
Image references
- Figure 1. Pneumonia right side segmental X-ray 1. theSimTech. Available from: [LINK]
